Page 8 of 23
PE25.3 | Acute Laryngotracheobronchitis — SDL Guide (Part 2)
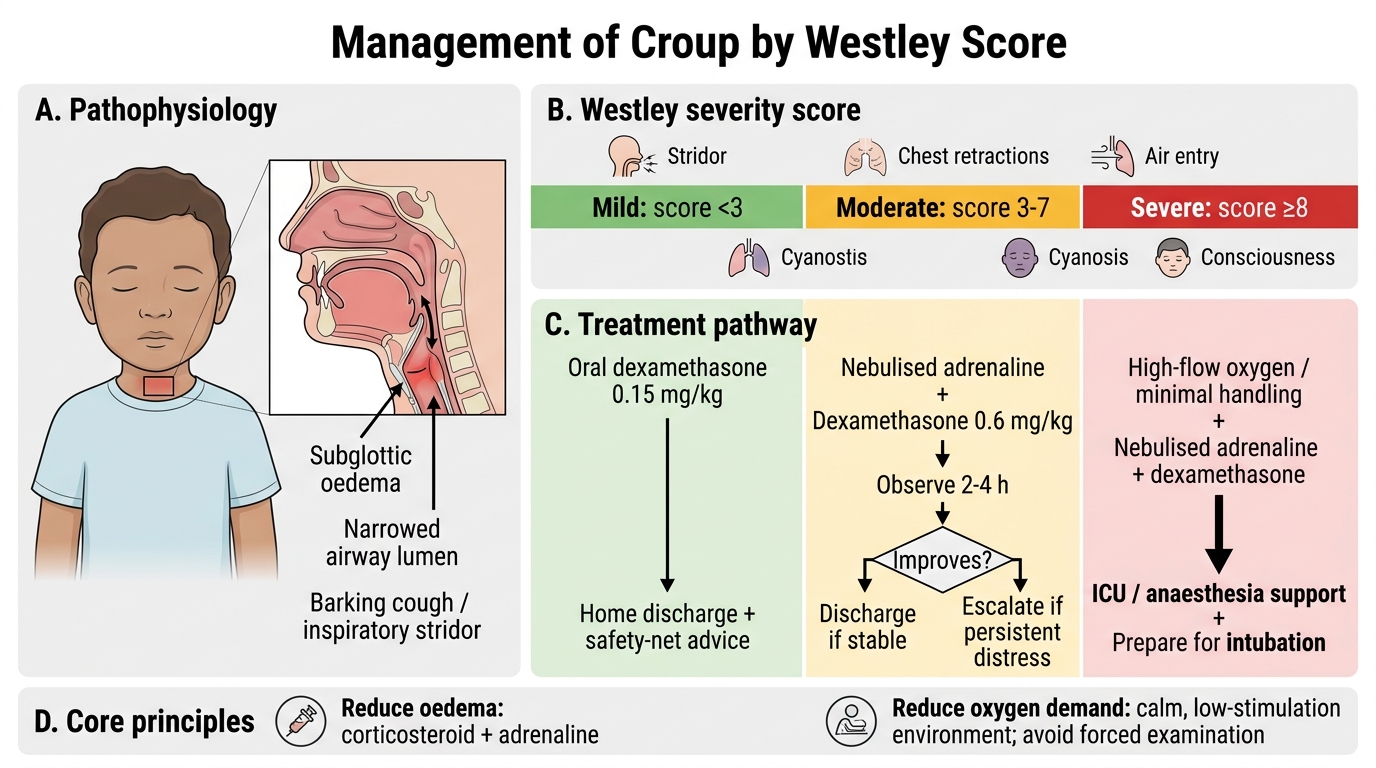
Management of Croup
The management of croup is stratified by Westley severity score and is built around two pharmacological interventions — corticosteroids for their anti-inflammatory effect on the subglottic mucosa and nebulised adrenaline for its rapid vasoconstrictor-mediated reduction in mucosal oedema. Both are weight-based in paediatric practice, and both have evidence bases strong enough to make them standard of care in all moderate-to-severe cases. The overarching goal is to reduce subglottic oedema sufficiently to restore comfortable breathing and prevent progression to respiratory failure. A calm, low-stimulation environment reduces the child's work of breathing by minimising agitation-driven increased airflow demand — for this reason, unnecessary procedures and forced examinations should be avoided. Applied calmly, these two principles — pharmacological reduction of oedema and behavioural reduction of oxygen demand — are enough to manage the majority of moderate croup cases safely.
Corticosteroids (cornerstone of management at all but the very mildest severity):
- Dexamethasone is the corticosteroid of choice due to its long half-life (~36-72 h) and excellent oral bioavailability
- Mild croup (Westley <3): 0.15 mg/kg orally, single dose — reduces duration of symptoms and risk of re-presentation; can be given and child discharged
- Moderate-severe croup (Westley ≥3): 0.6 mg/kg orally/IM/IV, single dose — maximum 10 mg
- Oral dexamethasone is preferred; it is as effective as IM/IV and avoids the distress of injection
- Prednisolone 1-2 mg/kg/day is an alternative if dexamethasone is unavailable
- Budesonide nebulised (2 mg) may be used when the oral or IM route is not feasible (vomiting, severe distress)
Nebulised adrenaline (epinephrine) — for moderate-severe croup:
- Mechanism: alpha-adrenergic vasoconstriction of the subglottic mucosal vasculature reduces oedema within 10-30 minutes
- Dose: L-epinephrine (1:1000) 5 mL nebulised, OR racemic epinephrine 0.5 mL/kg (max 5 mL) of 2.25% solution diluted to 3-5 mL with normal saline
- Onset: 10-30 minutes; Duration: 1-2 hours
- Rebound phenomenon: symptoms can return to pre-treatment severity 2-3 hours after nebulisation as the vasoconstrictor effect wanes. Therefore, every child receiving nebulised adrenaline must be observed for a minimum of 2-4 hours post-nebulisation before discharge. Discharge is safe only when stridor at rest has resolved and the child remains stable off nebulisation.
- Nebulised adrenaline can be repeated every 20-30 minutes in severe cases while preparing for definitive airway management
Oxygen:
- Supplemental oxygen for oxygen saturation <92% or in moderate-severe distress
- High-flow humidified oxygen via face mask (avoid forcing the mask; blow-by acceptable in a distressed infant)
Indications for hospitalisation:
- Westley score ≥3 (moderate)
- Failure to improve with nebulised adrenaline
- Rebound after nebulised adrenaline requiring repeat dosing
- Age <6 months
- Unable to maintain adequate oral hydration
Indications for intubation:
- Westley score ≥8 with progressive respiratory failure, rising PCO₂, or depressed consciousness
- Intubation in croup uses a tube 0.5-1 mm smaller than age-appropriate (due to subglottic narrowing); extubation is typically possible within 2-3 days as oedema resolves
What NOT to use:
- Antibiotics are not indicated for viral croup (LTB)
- Mist therapy (steam/humidified air) was a traditional recommendation but is NOT supported by evidence and is no longer recommended
- Sedation is contraindicated (risks respiratory depression)
Management of Croup by Westley Score
CLINICAL PEARL
Two croup management rules that must be automatic: (1) Every child receiving nebulised adrenaline must be observed for at least 2-4 hours post-nebulisation before being discharged — the rebound phenomenon means that symptoms can return to pre-treatment levels once the vasoconstrictor wanes, and a child who looks well at 30 minutes may deteriorate at 2 hours. (2) Oral dexamethasone is as effective as IM or IV dexamethasone and is preferred — it avoids the distress of injections and the injection-induced crying that increases the child's work of breathing. Give dexamethasone orally at 0.6 mg/kg (moderate-severe) or 0.15 mg/kg (mild) as a single dose and reassess.
Self-Assessment — Croup
Croup is a condition where pattern recognition, scoring, and decisive treatment combine to transform a frightening middle-of-the-night emergency into a safe, manageable encounter. Before attempting the self-assessment quiz, mentally rehearse the full clinical picture: a child between 6 months and 3 years, barking cough waking them from sleep, low-grade fever, a 1-3 day URTI prodrome, and inspiratory stridor at rest indicating at least moderate severity. The Westley score tells you the exact treatment tier. A single oral dose of dexamethasone at the correct weight-based dose and observation for rebound after nebulised adrenaline are the two actions that most directly improve outcomes. The ability to calculate these doses accurately by weight — never using a fixed adult dose — is what separates safe paediatric prescribing from dangerous practice.
Test yourself with the case-based quiz below.
SELF-CHECK
A 2-year-old child with moderate croup (Westley score 5) receives nebulised adrenaline in the emergency department and improves dramatically — the barking cough stops and stridor resolves within 20 minutes. The parents ask if they can take him home. What is the correct response?
A. Yes, he has responded well — discharge with oral dexamethasone and return if worsening
B. No, he must be admitted to PICU immediately despite the improvement
C. No, observe for at least 2-4 hours post-nebulisation for rebound; give dexamethasone before discharge
D. Give a second dose of nebulised adrenaline prophylactically before discharge to prevent rebound
Reveal Answer
Answer: C. No, observe for at least 2-4 hours post-nebulisation for rebound; give dexamethasone before discharge
The rebound phenomenon after nebulised adrenaline means that symptoms can return to pre-treatment severity 2-3 hours after nebulisation as the vasoconstrictor effect wanes. Immediate apparent resolution does NOT mean the child is safe to discharge. He must be observed for a minimum of 2-4 hours post-nebulisation and must have received dexamethasone (0.6 mg/kg for moderate croup) before discharge. Discharge is appropriate only if stridor at rest has completely resolved and the child has been stable throughout the observation window. PICU admission is not necessary if he remains stable. A prophylactic second adrenaline dose is not standard practice and does not prevent rebound.