Page 4 of 23
PE25.2 | Epiglottitis — SDL Guide
Learning Objectives
- Describe the etio-pathogenesis of epiglottitis including the role of Haemophilus influenzae type b and post-vaccine-era organisms
- Recognise the clinical features of epiglottitis including tripod position, drooling, muffled voice, and rapid progression
- Identify the contraindication to throat examination in suspected epiglottitis and explain why
- Describe the radiological thumbprint sign on lateral neck X-ray
- Outline the emergency management of epiglottitis including airway securing in OT and appropriate antibiotic therapy with weight-based dosing
INSTRUCTIONS
Epiglottitis is a paediatric emergency in which hours — sometimes minutes — determine survival. The condition is rare in vaccinated populations but remains a life-threatening diagnosis that every clinician must be able to recognise and manage correctly. The single greatest danger is a well-meaning attempt to examine the throat at the bedside, which can precipitate complete airway obstruction in a child who is maintaining a partially patent airway by their own positioning. This module equips you with the pattern recognition, the critical safety rules, and the management algorithm needed to handle this emergency correctly from the first moment.
References
- Ghai Essential Pediatrics, 9th ed., Ch 17 — Upper Airway Emergencies (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 412 — Epiglottitis (textbook)
- IAP Textbook of Pediatrics, 6th ed. — Respiratory Emergencies (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-year-old boy is brought to the emergency department at midnight with a 6-hour history of high fever (39.8°C), rapidly worsening sore throat, and what his parents describe as 'a funny voice.' On entry to the triage room, you notice he is sitting bolt upright on his father's lap, leaning forward with both hands on his knees, neck extended, mouth open, and a thin strand of saliva drooling from his lip. He appears anxious and is breathing with an audible soft inspiratory noise. The nurse asks you to lie him down for examination. What is your immediate priority — and what must you never do?
WHY THIS MATTERS
Epiglottitis is one of the few paediatric emergencies where an incorrect initial action — attempting to examine the throat at the bedside — can kill the child in seconds. The swollen epiglottis in this condition acts as a ball valve: the child is maintaining a precarious partial airway by adopting the tripod position and by voluntary muscle tone. Any disturbance — lying the child supine, depressing the tongue with a spatula, or even crying from distress — can cause the inflamed epiglottis to shift and completely obstruct the airway. Although Hib vaccination has made classic epiglottitis rare in India's expanding immunised population, unvaccinated children remain at risk, and the condition still occurs in older children and adults due to other organisms. Recognising epiglottitis instantly and activating the correct response pathway is a life-saving clinical skill.
RECALL
Recall from your anatomy of the larynx that the epiglottis is a leaf-shaped fibroelastic cartilage attached to the inner surface of the thyroid cartilage at the angle of the V. During swallowing, it folds backward over the glottis to prevent aspiration. The epiglottis and the aryepiglottic folds that connect it to the arytenoids form the supraglottic airway — the region involved in epiglottitis. Recall also from your microbiology that Haemophilus influenzae type b (Hib) is an encapsulated organism whose polysaccharide capsule (polyribosylribitol phosphate, PRP) is the key virulence determinant; this capsule allows it to evade phagocytosis and produce invasive disease. Hib immunisation (as part of the pentavalent vaccine in India's NIS at 6, 10, and 14 weeks with a booster at 16-24 months) generates anti-PRP antibodies that are protective. This is why classic epiglottitis is now rare in adequately vaccinated children.
Clinical Presentation of Epiglottitis
Epiglottitis typically presents in children aged 2-7 years (peak 3-5 years in the pre-vaccine era; now older with broader age range) with a strikingly rapid onset over 4-12 hours. The speed of progression distinguishes it from most other upper respiratory infections and is itself a diagnostic clue. The child who appeared well at dinner is in extremis by midnight. This rapidity reflects the highly vascular and loose submucosal tissue of the supraglottic larynx, which responds to bacterial invasion with rapid oedema formation that can narrow the airway to a critical degree within hours. Unlike croup, which builds gradually over days, epiglottitis demands immediate recognition — a delay of even an hour in calling the anaesthetic team can be fatal. Recognising the full clinical constellation, understanding the anatomical reason for each sign, and knowing immediately what NOT to do, constitutes the most critical skill this module teaches.
Provided image
The classic tetrad of epiglottitis is:
- High fever (typically ≥39°C) — abrupt onset, toxic appearance
- Severe sore throat and dysphagia — the child refuses to eat or drink; drooling is a cardinal sign because the child cannot swallow saliva
- Muffled ("hot-potato") voice — the inflamed supraglottic structures muffle the voice without producing the barky cough characteristic of subglottic croup; the child sounds as if speaking with a mouthful of food
- Inspiratory stridor — soft and low-pitched (supraglottic), often less noisy than the steeple-sign stridor of croup
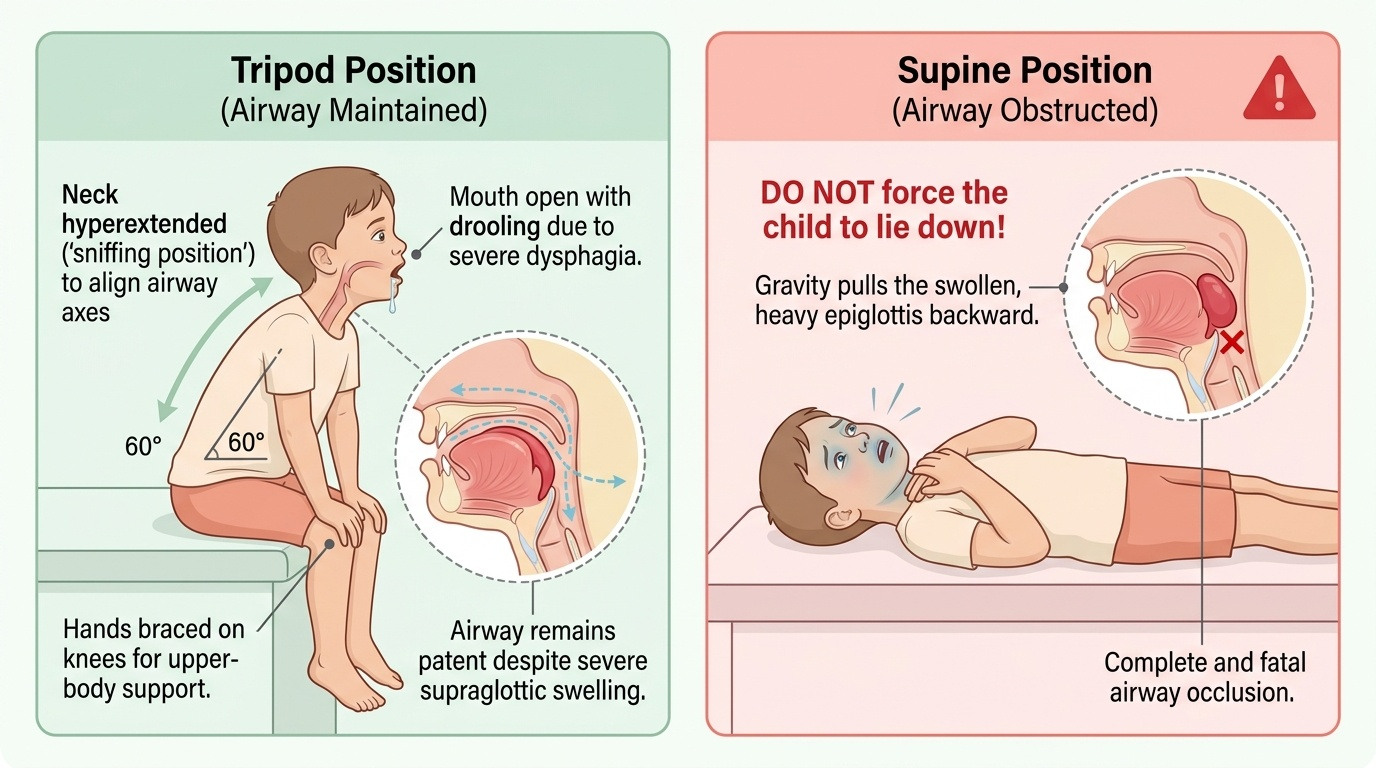
The tripod position (also called the sniffing position or "drooling-tripod"): the child sits upright, leans forward with hands on knees or the bed, hyperextends the neck, and opens the mouth. This is the child's instinctive way of maximising airway patency by aligning the oropharyngeal, laryngeal, and tracheal axes and reducing supraglottic soft-tissue prolapse. This position must be preserved. Do not force the child to lie down.
Additional features: anxiety and restlessness (from hypoxia), preference for sitting on parent's lap, and refusal to speak or eat. Cough is notably absent or minimal — a key distinguishing feature from croup.
IMPORTANT: the absence of all four classic features does NOT exclude epiglottitis. Post-Hib-vaccine presentations may be atypical — less dramatic, older age group, milder fever.
Pathophysiology and Aetiology
The pathogenesis of epiglottitis begins with bacteraemia (bloodstream invasion) following mucosal colonisation by the causative organism, in contrast to croup where local viral replication drives inflammation. Haemophilus influenzae type b (Hib) remains the classical and historically dominant pathogen. Its polysaccharide capsule enables evasion of innate immune defences and haematogenous seeding of the highly vascular loose connective tissue of the epiglottis and aryepiglottic folds. This triggers an intense acute inflammatory response with oedema, hyperaemia, and neutrophil infiltration of the supraglottic submucosa. The epiglottis, normally a thin, pale, crescent-shaped structure, becomes a massively swollen, cherry-red, rounded mass that occupies the base of the tongue. The aryepiglottic folds are similarly engorged. Progressive airway narrowing leads to turbulent airflow (stridor), increased respiratory effort, and ultimately complete obstruction if untreated.
In the post-Hib-vaccine era, the microbial landscape has shifted:
- Streptococcus pyogenes (Group A Streptococcus) — increasingly common cause
- Streptococcus pneumoniae — capsulated organism with similar invasive potential
- Staphylococcus aureus (including MRSA) — less common but important in immunocompromised children
- Hib still causes epiglottitis in unvaccinated children and vaccine failures
Differential diagnosis comparison — Epiglottitis vs Croup (LTB):
| Feature | Epiglottitis | Croup (LTB) |
|---|---|---|
| Age | 2-7 years (peak) | 6 months-3 years |
| Pathogen | Hib (bacteria) | Parainfluenza (virus) |
| Onset | Rapid (hours) | Gradual (days) |
| Location | Supraglottic | Subglottic |
| Voice | Muffled, hot-potato | Hoarse |
| Cough | Absent/mild | Barking, brassy |
| Drooling | Prominent | Absent |
| Position | Tripod (leaning forward) | No preference |
| Fever | High (≥39°C) | Low-grade |
| X-ray sign | Thumbprint (lateral neck) | Steeple sign (AP view) |
| Throat exam | CONTRAINDICATED | Safe |
| Management | Airway in OT + IV antibiotics | Nebulised adrenaline + oral dexamethasone |
Diagnosis and Investigation
The most important diagnostic rule for epiglottitis is this: when the clinical diagnosis is suspected, investigation takes a subordinate role to airway management. No investigation should delay or compromise the airway — this principle overrides the usual clinical instinct to gather information before acting.
The diagnosis of epiglottitis is first and foremost a clinical one, based on the clinical presentation described above. However, several investigations support the diagnosis or are obtained after the airway is secured:
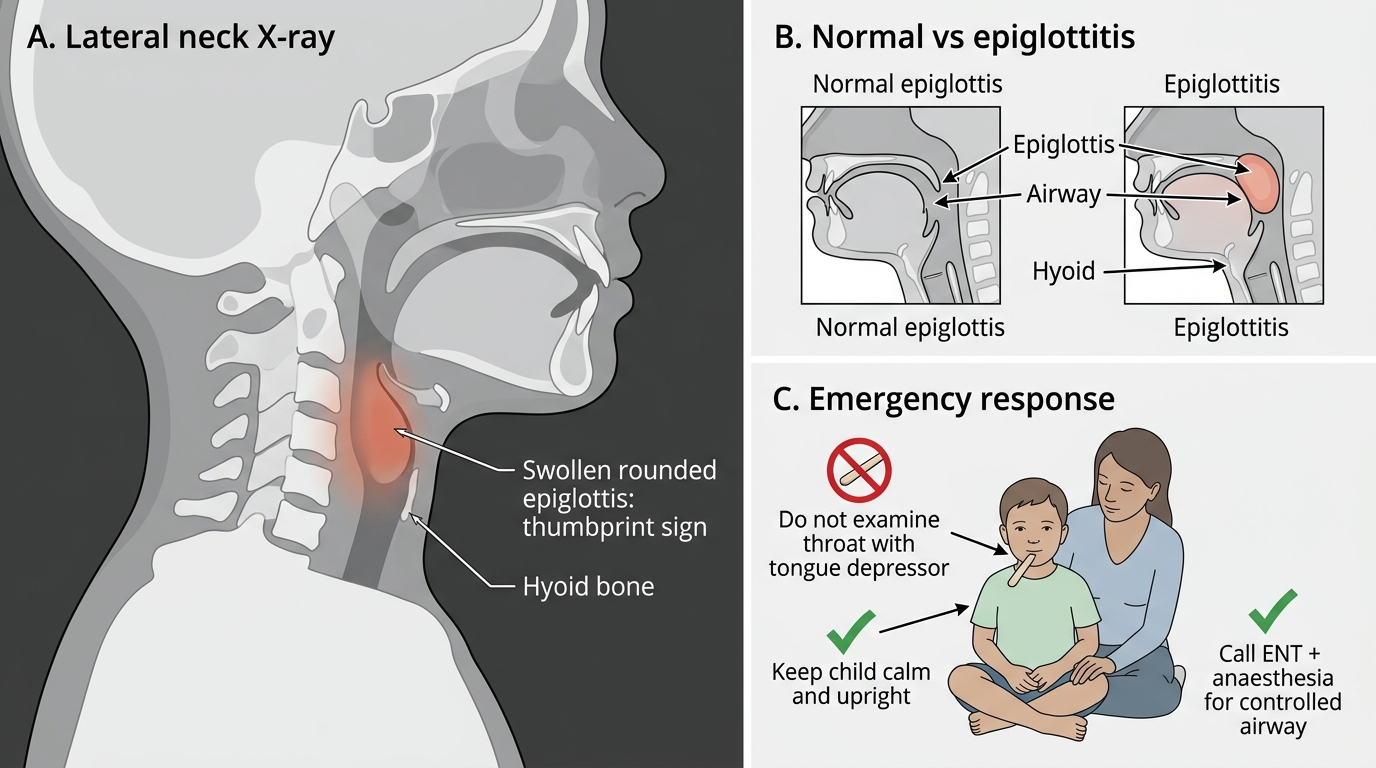
Lateral neck X-ray (the most useful diagnostic radiograph): If the child is stable enough to move (never leave a child with suspected epiglottitis unaccompanied), a lateral soft-tissue neck X-ray classically shows the thumbprint sign: the swollen, rounded epiglottis projects from the base of the tongue like an adult's raised thumb, occupying the vallecula and hypopharynx. This contrasts sharply with the normal thin, elongated epiglottic silhouette. The aryepiglottic folds may also appear thickened. The X-ray must be done with the child upright and awake — never supine or sedated until the airway is secured.
IMPORTANT: A normal lateral neck X-ray does NOT exclude epiglottitis if the clinical picture is consistent. Do not be falsely reassured by a negative film.
Blood cultures: Obtained after airway is secured; positive in 50-80% of bacterial epiglottitis cases; guides targeted antibiotic therapy and confirms the pathogen.
Full blood count: Typically shows leukocytosis with neutrophilia reflecting bacterial aetiology — obtained after airway is secured.
Throat swab / direct laryngoscopy culture: Culture of the epiglottic surface is obtained at the time of airway instrumentation in OT; do NOT attempt this in the ED.
THE RULE — repeat it until automatic: Do NOT examine the throat, do NOT depress the tongue, do NOT place the child supine, do NOT perform nasopharyngoscopy in the ED. Any of these manoeuvres in a child with epiglottitis can precipitate complete and fatal airway obstruction.
Thumbprint Sign in Acute Epiglottitis
SELF-CHECK
A 5-year-old child presents with high fever, drooling, and the classic tripod position. The nurse wants to look in the throat to confirm the diagnosis before calling ENT. What is the correct immediate response?
A. Allow a brief look with a tongue depressor in a well-lit room before calling ENT
B. Decline the throat examination, keep the child calm and upright, call ENT and anaesthesia immediately for controlled airway in OT
C. Obtain a lateral neck X-ray first to confirm thumbprint sign before any action
D. Administer nebulised adrenaline immediately as for croup while awaiting ENT
Reveal Answer
Answer: B. Decline the throat examination, keep the child calm and upright, call ENT and anaesthesia immediately for controlled airway in OT
In suspected epiglottitis, throat examination with a tongue depressor or spatula is absolutely contraindicated in the emergency setting because it can trigger complete airway obstruction by displacing the swollen epiglottis. The immediate priority is to keep the child calm and sitting upright in their parent's lap, call ENT and anaesthesia for controlled intubation in OT with surgical backup available, and avoid any intervention that may distress the child or change their position. The lateral neck X-ray may support the diagnosis but should never delay calling for definitive airway management. Nebulised adrenaline is used for subglottic croup, not for supraglottic epiglottitis.