Page 5 of 23
PE25.2 | Epiglottitis — SDL Guide (Part 2)
Management of Epiglottitis
The management of epiglottitis is a team emergency requiring immediate coordination between the paediatrician, anaesthetist, and ENT surgeon. Every step in the management algorithm follows from a single overriding principle: maintain the airway and do nothing to threaten it until the airway is definitively secured under controlled conditions. This principle explains every rule in the management protocol — including why blood draws, IV cannulation, and even parental separation should be deferred until the child is in OT if they may cause distress. Understanding WHY each rule exists — why the child must stay upright, why IV access waits, why the team must convene before anyone touches the child — is what allows these rules to be applied consistently under the pressure of a real emergency rather than memorised and forgotten. The sequence below follows the time-critical priority order: airway first, then team activation, then antibiotics.
Step 1 — Immediate assessment and stabilisation (Emergency Department):
- Keep child calm, sitting upright in parent's lap, do NOT force supine
- Administer supplemental humidified oxygen by blow-by or face mask held near (not forced on) the child's face — avoid anything that distresses them
- Do NOT perform throat examination or any procedure that may distress the child
- Do NOT attempt IV cannulation or blood draw in the ED if it will agitate the child
- Activate team: senior paediatrician + anaesthesist + ENT surgeon must be called simultaneously
Step 2 — Secure the airway (Operating Theatre — controlled, urgent):
- Endotracheal intubation under general anaesthesia (gas induction in the child's position of comfort) — performed by an experienced anaesthetist
- ENT surgeon must be present for emergency tracheotomy if intubation fails due to complete obstruction
- After intubation: direct laryngoscopy confirms the diagnosis (cherry-red, swollen epiglottis) and surface cultures are obtained
- Child transferred to PICU for monitoring and care of intubated airway
Step 3 — Antibiotic therapy (IV, weight-based):
- First-line: Ceftriaxone 50-100 mg/kg/day IV (once daily, maximum 2 g/dose) — covers Hib and most streptococcal causes; may be given once IV access is established in OT
- Alternative: Cefotaxime 150-200 mg/kg/day in 3-4 divided doses IV
- Duration: IV antibiotics until clinically improved (fever settling, oedema resolving, typically 48-72 h), then oral step-down for a total of 7-10 days
- If MRSA is a concern (particularly in immunocompromised or unresponsive cases): add vancomycin or clindamycin
Step 4 — Adjunct therapy:
- Dexamethasone 0.6 mg/kg IV (single dose or short 2-day course) to reduce supraglottic oedema — commonly used in clinical practice, though evidence base for benefit specifically in epiglottitis is less robust than in croup
- Adequate analgesia and antipyretics once airway is secured
- Humidified ventilator circuit for the intubated child
Step 5 — Extubation and discharge:
- Extubation is considered after 24-48 h once fever resolves and direct laryngoscopy (or repeat imaging) confirms oedema resolution
- Child can be stepped down from PICU and discharged on oral antibiotics to complete the course
Post-exposure prophylaxis:
- Rifampicin prophylaxis for unvaccinated household contacts and index case (if <2 years) — eradicates Hib nasopharyngeal carriage in close contacts
- Ensure immunisation status of all household contacts is updated
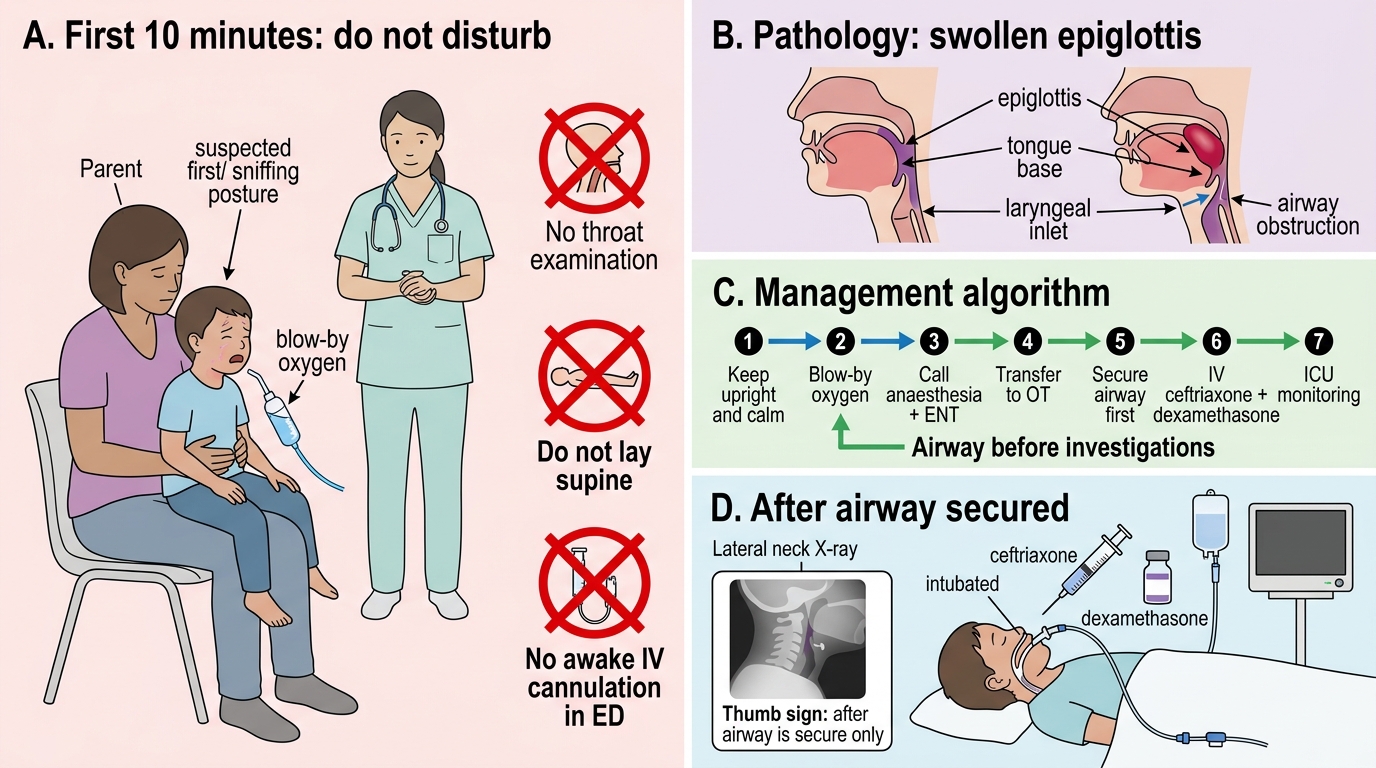
Suspected Epiglottitis: Airway-First Management Algorithm
CLINICAL PEARL
The most dangerous moment in epiglottitis management is the first 10 minutes in the emergency department. The three actions most likely to precipitate fatal airway obstruction are: (1) attempting direct throat examination with a tongue depressor, (2) placing the child supine for examination or chest X-ray, and (3) attempting IV cannulation in the ED while the child is awake and uncooperative. All three distress the child, cause crying and Valsalva, and can shift the swollen epiglottis to completely occlude the airway. Keep the child on the parent's lap, upright, calm, with blow-by oxygen — and use that time to summon the team to OT. The airway must be secured before any other investigation or treatment.
Self-Assessment — Epiglottitis
Epiglottitis requires you to override the usual instinct to examine and investigate before treating — the diagnosis is clinical, the treatment is airway management, and investigation follows after the airway is secure. Before testing yourself, consider whether you can answer these three questions confidently: (1) Which single clinical sign tells you the child has adopted the optimal airway-preserving posture and must not be disturbed? (2) What is the name and appearance of the radiological sign on lateral neck X-ray? (3) What is the first-line intravenous antibiotic and its weight-based dose? If you can answer all three without hesitation, you are prepared to recognise and begin managing this emergency correctly. This means understanding not just the facts — the organism, the X-ray sign, the antibiotic dose — but also the clinical logic that links them: why Hib colonises the supraglottis haematogenously rather than by direct extension, why the thumbprint sign appears as it does, and why ceftriaxone is superior to ampicillin in the post-vaccine era when beta-lactamase-producing strains are encountered.
Test yourself with the quiz below.
SELF-CHECK
A child with confirmed epiglottitis has been intubated in OT. IV access is now established. Which antibiotic is the most appropriate first-line IV treatment and at what dose?
A. Ampicillin 200 mg/kg/day IV in 4 divided doses
B. Ceftriaxone 50-100 mg/kg/day IV once daily (max 2 g)
C. Azithromycin 10 mg/kg/day IV
D. Amoxicillin-clavulanate 90 mg/kg/day IV
Reveal Answer
Answer: B. Ceftriaxone 50-100 mg/kg/day IV once daily (max 2 g)
Ceftriaxone 50-100 mg/kg/day IV (once daily, maximum 2 g/dose) is the first-line antibiotic for epiglottitis. It provides excellent coverage against Haemophilus influenzae type b, Streptococcus pyogenes, and S. pneumoniae — the principal causative organisms. Ampicillin alone is inadequate because many Hib strains produce beta-lactamase and are ampicillin-resistant. Azithromycin is not appropriate for systemic bacterial epiglottitis. Amoxicillin-clavulanate is an oral formulation used for AOM (not IV epiglottitis). Cefotaxime is an acceptable alternative to ceftriaxone.