Page 10 of 23
PE25.4 | Stridor — SDL Guide
Learning Objectives
- Define stridor and classify it by phase (inspiratory, expiratory, biphasic) and aetiology (acute vs chronic)
- Explain the anatomical basis of stridor phase as a localising sign for the level of airway obstruction
- Identify the most common causes of acute and chronic stridor in children with their distinguishing clinical features
- Describe laryngomalacia as the most common cause of chronic inspiratory stridor in infants and its clinical course
- Outline the immediate assessment and cause-specific management of a child presenting with stridor
INSTRUCTIONS
Stridor is not a diagnosis — it is a symptom that demands a diagnosis. The noisy breathing of a stridulous child is alarming to parents and, in the acute setting, can represent a immediately life-threatening airway emergency. However, stridor can equally be a benign, self-limiting condition in an otherwise thriving infant. The key clinical skill is to distinguish the acutely distressed child who needs immediate intervention from the chronically stridulous infant who needs reassurance and monitoring. This module provides the anatomical framework for localising stridor and the clinical framework for systematically evaluating its cause.
References
- Ghai Essential Pediatrics, 9th ed., Ch 17 — Stridor in Children (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 412 — Stridor (textbook)
- IAP Textbook of Pediatrics, 6th ed. — Respiratory Emergencies (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two children arrive at your outpatient clinic on the same afternoon with noisy breathing. The first is a 6-week-old boy whose parents report a soft, gurgling, crowing sound since birth that worsens when he cries or feeds but improves when he lies prone; he is gaining weight normally. The second is a 2-year-old girl with a 2-day history of barking cough, 38.5°C fever, and a new harsh inspiratory noise that her parents say has been getting louder since last night. Both children have 'stridor.' Are they the same emergency? How does the character, timing, and context of stridor guide your next action?
WHY THIS MATTERS
Stridor is one of the most common respiratory symptoms prompting urgent paediatric consultation, and it spans the full spectrum from the benign (laryngomalacia in a thriving infant) to the immediately life-threatening (acute epiglottitis, foreign body, anaphylaxis). A clinician who cannot rapidly assess stridor — localise its anatomical origin from its phase, determine acuity from the history, and match the clinical pattern to a diagnosis — will either over-treat the benign infant (unnecessary hospital admission, anxiety) or, far more dangerously, under-treat or mismanage the acutely obstructed child. This module builds the systematic framework that allows confident, safe decision-making for every child presenting with stridor.
RECALL
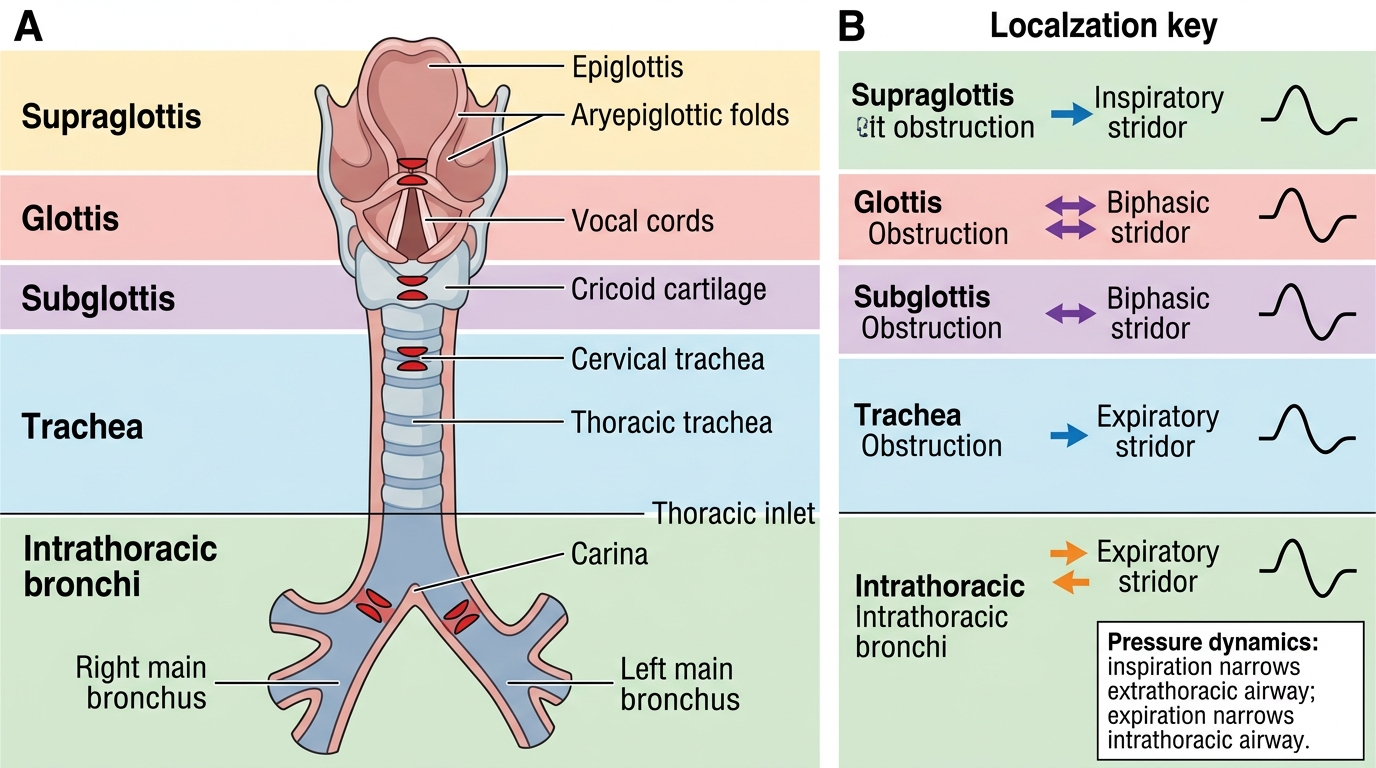
Recall the anatomy of the upper and lower airways. The larynx is divided into three regions: the supraglottis (epiglottis, aryepiglottic folds, arytenoids), the glottis (true and false vocal cords), and the subglottis (the region below the vocal cords to the lower border of the cricoid cartilage — the narrowest fixed portion of the paediatric airway). The trachea continues below the cricoid into the mediastinum (intrathoracic), bifurcating into the right and left main bronchi. This anatomy is the map for localising stridor: the level of obstruction determines the phase of noisy breathing. Also recall from physiology that the extrathoracic airway is subjected to atmospheric pressure outside and negative intraluminal pressure during inspiration — this dynamic is the key to understanding why inspiratory stridor localises to the extrathoracic airway.
Approach to a Child with Stridor — Clinical Assessment
The clinical assessment of a stridulous child begins with a rapid determination of whether the child is in immediate danger of airway compromise. This triage step must precede any history-taking or examination in the acutely distressed child. A child who is pale, cyanosed, severely retracting, unable to maintain their posture, or has a declining oxygen saturation requires immediate airway intervention — attempting to complete a systematic assessment in such a child wastes the time available for life-saving management. Once the child is determined to be stable (or stabilised), a structured history and examination follows to identify the underlying cause. The two-step triage (is the child distressed? is this acute or chronic?) is a rapid, high-yield framework that can be applied at the bedside, in a consultation room, or in a resuscitation bay — and applying it correctly is the most important single skill this module trains.
Immediate red flags (act first, ask later):
- Cyanosis (central, circumoral)
- SpO₂ <92% despite supplemental oxygen
- Severe retractions (suprasternal, subcostal) with exhaustion
- Tripod position with drooling (epiglottitis — do NOT examine throat)
- Silent chest (no air movement — pre-arrest)
- Rapidly progressive symptoms over minutes
Structured assessment — key history questions:
1. Age of onset: Congenital at birth or within 2 weeks (laryngomalacia, subglottic stenosis, haemangioma, vascular ring); acquired acute onset (croup, epiglottitis, FB aspiration, anaphylaxis)
2. Phase of noisy breathing: Inspiratory only, expiratory only, or biphasic? (See pathophysiology block)
3. Quality of sound: Barking cough (croup), muffled voice (epiglottitis), high-pitched crowing (laryngomalacia), low-pitched rhonchi (secretions)
4. Positional variation: Worse supine, better prone (laryngomalacia — hallmark feature); worse with extension (vascular ring); no positional variation (FB)
5. Feeding: Worsens with feeds (laryngomalacia); refusal to eat, drooling (epiglottitis, acute obstruction)
6. Associated symptoms: Fever (infection); no fever (FB, congenital causes); barking cough + URTI prodrome (croup); rash/urticaria (anaphylaxis)
7. Past episodes: Recurrent (laryngomalacia, asthma, recurrent croup in atopic child); first episode acute (FB, epiglottitis)
8. Vaccinations: Hib-vaccinated? (reduces epiglottitis risk substantially)
Examination:
- Respiratory rate, SpO₂, work of breathing (nasal flaring, retractions, accessory muscles)
- Voice quality: normal (FB/laryngomalacia), hoarse (croup), muffled hot-potato (epiglottitis)
- Neck examination: anterior neck masses (cystic hygroma, goitre compressing trachea); post-auricular swelling (mastoiditis)
- Chest: air entry symmetry (asymmetric = FB); wheeze (lower airway)
- Skin: haemangiomas (may indicate subglottic haemangioma in infants with beard-distribution cutaneous lesion)
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Anatomical Localisation of Stridor
Pathophysiology of Stridor and Anatomical Localisation
Stridor is produced by turbulent airflow through a narrowed segment of the airway, generating audible vibrations in the airway walls and mucosa. The phase of stridor — whether it occurs on inspiration, expiration, or both — is not random; it reflects a predictable relationship between airway pressure dynamics and the location of the obstruction. Understanding this relationship allows the clinician to use the phase of stridor as an anatomical localising sign — a non-invasive, instantaneous tool that narrows the differential diagnosis before any investigation is performed. This localising power derives from the different pressure environments the extrathoracic and intrathoracic airways experience during the respiratory cycle.
The pressure-dynamics basis of stridor phase:
During INSPIRATION: The diaphragm descends, creating negative (subatmospheric) intrathoracic pressure. This negative pressure:
- DILATES the intrathoracic (below the thoracic inlet) airway — because the pressure inside the trachea and bronchi is more negative than the surrounding pleura, the walls are pulled outward
- NARROWS the extrathoracic airway — the Bernoulli effect causes the airway wall to be pulled inward at any point of narrowing above the thoracic inlet
Therefore, obstruction in the EXTRATHORACIC airway (supraglottis, glottis, subglottis) worsens on INSPIRATION → inspiratory stridor.
During EXPIRATION: Positive intrathoracic pressure is generated:
- COMPRESSES the intrathoracic airway — the bronchi and trachea are narrowed by the surrounding increased thoracic pressure
- DILATES the extrathoracic airway — positive pressure below the obstruction splints the extrathoracic lumen open
Therefore, obstruction in the INTRATHORACIC airway worsens on EXPIRATION → expiratory stridor (wheeze).
Summary of stridor localisation:
| Phase | Anatomical level | Examples |
|---|---|---|
| Inspiratory only | Extrathoracic (supraglottis, glottis, subglottis) | Laryngomalacia, epiglottitis, croup, FB at larynx |
| Expiratory only | Intrathoracic (lower trachea, bronchi) | Lower tracheal mass, airway compression by vascular ring below thoracic inlet, asthma |
| Biphasic (both) | Trachea (thoracic inlet level) or fixed subglottic obstruction | Subglottic stenosis (fixed), tracheal FB, bacterial tracheitis |
Aetiology — Causes of Stridor by Onset Pattern
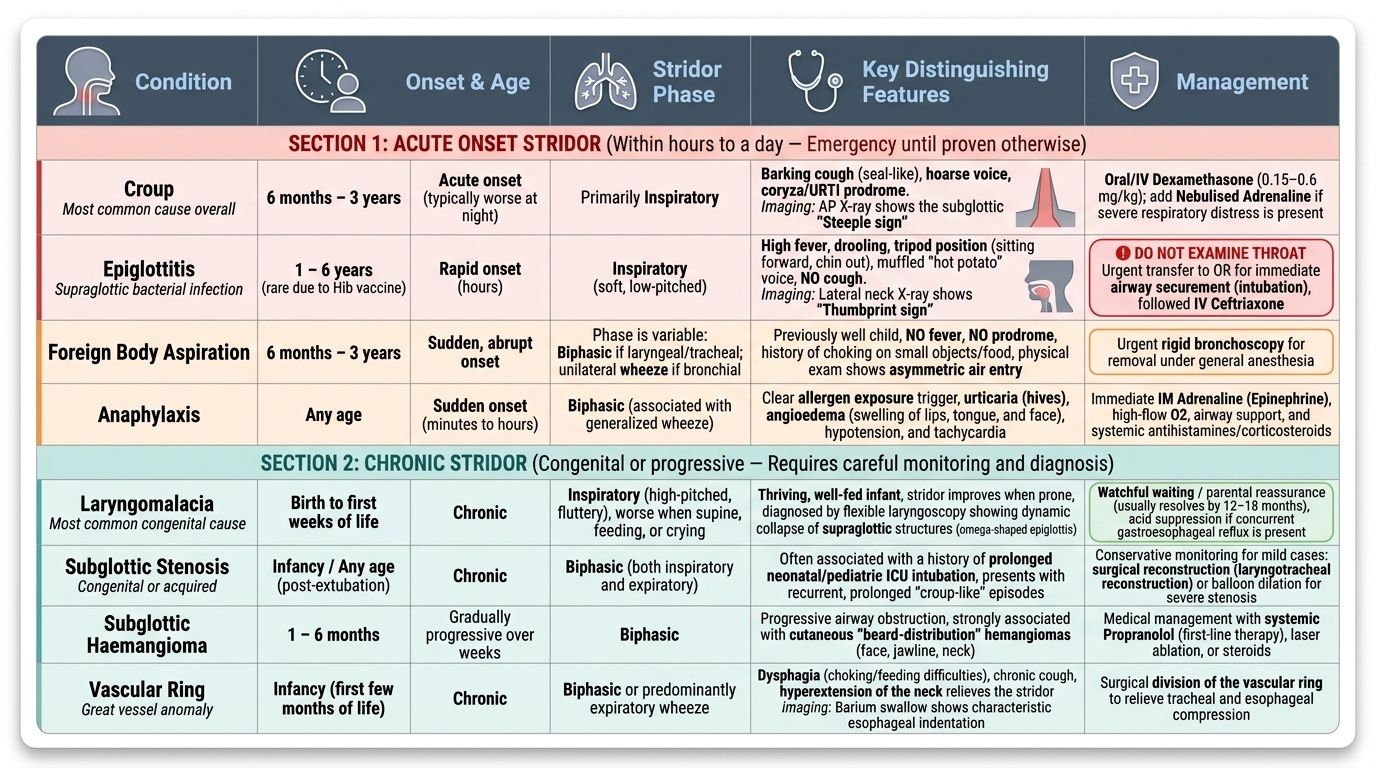
The single most useful discriminator in the aetiology of stridor is the onset pattern — whether the stridor began acutely (within hours to a day) or has been present chronically since early infancy. Acute-onset stridor in a previously well child is an emergency until proven otherwise; chronic stridor from birth or early infancy in a thriving, well-fed infant is usually laryngomalacia and requires careful monitoring rather than immediate intervention. The age at onset further narrows the differential: congenital anatomical causes present in the neonatal period or first weeks of life, while acquired viral and bacterial causes dominate the 6-month to 5-year age group. Applying onset pattern × age × phase × associated features creates a powerful discriminating matrix that covers the vast majority of clinical scenarios a final-year student will encounter.
Provided image
ACUTE STRIDOR causes:
- Croup (Acute Laryngotracheobronchitis) — most common cause of acute stridor overall; 6 months-3 years; parainfluenza; barking cough + hoarse voice + URTI prodrome; subglottic steeple sign on AP X-ray; treat with dexamethasone ± nebulised adrenaline
- Epiglottitis — supraglottic bacterial infection (Hib/post-vaccine); rapid onset hours; high fever, drooling, tripod position, muffled voice, NO cough; thumbprint sign on lateral neck X-ray; DO NOT examine throat; secured airway in OT + IV ceftriaxone
- Foreign body aspiration (FBA) — sudden onset in a well child aged 6 months-3 years with NO fever and NO prodrome; unilateral wheeze or asymmetric air entry suggests bronchial FB; laryngeal/tracheal FB may give biphasic stridor; often history of playing with small objects; requires urgent bronchoscopy
- Anaphylaxis — acute stridor from laryngeal oedema; associated urticaria, facial swelling, haemodynamic instability; precipitated by allergen exposure; treat with intramuscular adrenaline 0.01 mg/kg (1:1000)
- Bacterial tracheitis — rare; S. aureus; mimics severe croup but child is toxic and fails to respond to nebulised adrenaline; pseudomembranous tracheal obstruction; requires IV antibiotics + often intubation
CHRONIC / RECURRENT STRIDOR causes:
- Laryngomalacia — most common cause of chronic inspiratory stridor in infants, accounting for approximately 60-70% of congenital laryngeal anomalies; onset in first 2 weeks of life; intermittent inspiratory stridor that worsens with feeds, crying, and supine position, and improves prone; caused by prolapse of immature, hypotonic supraglottic structures (omega-shaped epiglottis, floppy arytenoid cartilages) into the airway during inspiration; the child is otherwise thriving; resolves spontaneously by 18-24 months in 90% of cases; supraglottoplasty is reserved for the 10% with severe apnoeas or failure to thrive
- Subglottic stenosis — congenital (narrowed cricoid ring) or acquired (post-prolonged intubation); presents with recurrent croup-like episodes at mild viral triggers; biphasic stridor; managed with serial endoscopic or open laryngotracheal reconstruction
- Subglottic haemangioma — appears at 4-6 weeks of age (haemangiomas grow rapidly in the first 6 months); associated with "beard distribution" cutaneous haemangiomas; biphasic stridor; treated with oral propranolol 2-3 mg/kg/day
- Vocal cord paralysis — unilateral (left recurrent laryngeal nerve; cardiac surgery, mediastinal mass) or bilateral (CNS causes: Arnold-Chiari, birth asphyxia); biphasic stridor with aspiration and weak cry
- Vascular ring — aberrant great vessels (double aortic arch, right-sided aortic arch) forming a complete or partial ring around the trachea and oesophagus; presents with biphasic stridor AND dysphagia; diagnosed on CT angiography; treated with surgical division
SELF-CHECK
A 3-week-old boy has had a soft, crowing inspiratory noise since day 10 of life. It worsens when he cries and during feeds but completely disappears when he is prone and sleeping. He is gaining weight appropriately and has no cyanosis. SpO₂ is 99%. What is the most likely diagnosis and appropriate management?
A. Epiglottitis — admit immediately and call ENT for airway management
B. Laryngomalacia — reassure parents, prone positioning, monitor weight; refer only if feeding difficulty or apnoea
C. Subglottic stenosis — perform laryngoscopy and plan laryngotracheal reconstruction
D. Croup — prescribe oral dexamethasone 0.15 mg/kg
Reveal Answer
Answer: B. Laryngomalacia — reassure parents, prone positioning, monitor weight; refer only if feeding difficulty or apnoea
This is the classic presentation of laryngomalacia: onset in first 2 weeks of life, soft inspiratory stridor that worsens with feeds/crying/supine and improves prone, normal weight gain, and normal SpO₂. Laryngomalacia is caused by prolapse of floppy supraglottic structures during inspiration and is the most common cause of congenital inspiratory stridor (60-70% of laryngeal anomalies). In a thriving infant with no apnoea or failure to thrive, management is parental reassurance and monitoring; 90% resolve by 18-24 months. Epiglottitis is impossible at 3 weeks (no fever, no drooling, improves prone). Croup is a viral illness, not congenital. Subglottic stenosis produces biphasic stridor and recurrent croup-like episodes, not this typical feed-related pattern.