Page 11 of 23
PE25.4 | Stridor — SDL Guide (Part 2)
Management of Stridor
Management of stridor is fundamentally cause-specific — there is no single treatment for stridor as a symptom, and the approach differs entirely depending on whether the child has laryngomalacia, croup, epiglottitis, foreign body aspiration, or a fixed subglottic anomaly. However, the initial stabilisation steps are universal and apply before the definitive diagnosis is confirmed: maintain the airway, support oxygenation, and avoid manoeuvres that worsen the obstruction. This framework applies regardless of the suspected cause, and the few universal steps are completed within the first 2-3 minutes before cause-specific treatment is initiated. Understanding both the universal steps and the cause-specific pathways — and knowing which investigations are appropriate for each — allows a final-year student to manage the full range of stridulous children they will encounter in primary and referral practice.
Provided image
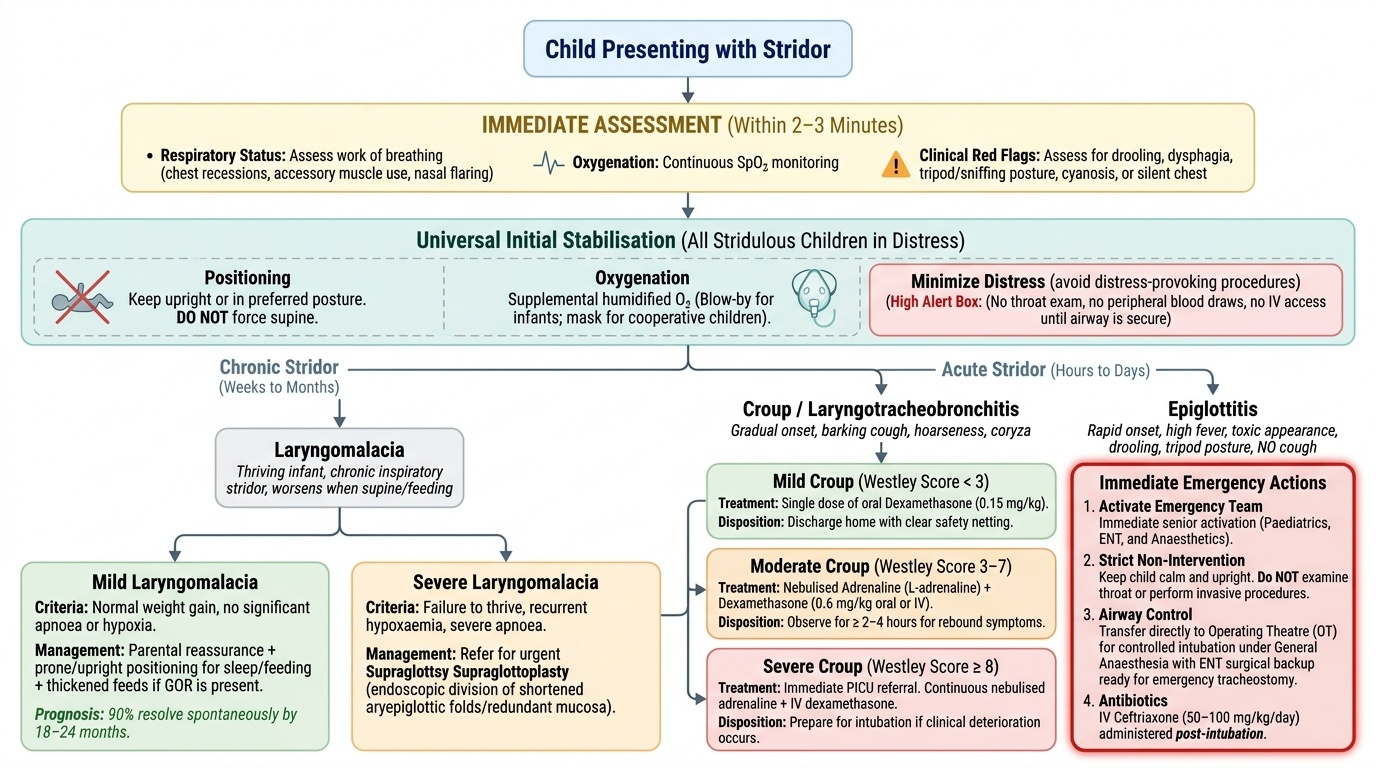
Universal initial stabilisation (all stridulous children with respiratory distress):
- Position the child upright or in their preferred posture (do NOT force supine)
- Administer supplemental humidified oxygen — blow-by in infants, mask in cooperative children
- Monitor SpO₂ continuously
- Avoid distress-provoking procedures (blood draw, throat examination, forced examination) until the child is stable
- Call for senior paediatric, ENT, and anaesthetic support if severe
Cause-specific management:
Laryngomalacia (chronic, thriving infant):
- Mild (normal weight gain, no apnoea): Parental reassurance + prone positioning for feeding and sleep + thickened feeds if GOR contributes; 90% spontaneous resolution by 18-24 months
- Severe (failure to thrive, recurrent apnoea, hypoxia): Supraglottoplasty (endoscopic division of shortened aryepiglottic folds and/or redundant arytenoid mucosa) — the definitive surgical treatment for refractory laryngomalacia
Croup (LTB):
- Mild (Westley <3): Single oral dexamethasone 0.15 mg/kg, discharge home
- Moderate (Westley 3-7): Nebulised adrenaline + dexamethasone 0.6 mg/kg, observe ≥2-4 h for rebound
- Severe (Westley ≥8): PICU, intubation if needed
Epiglottitis:
- Immediate team activation (paediatrics + ENT + anaesthetics)
- Keep child upright and calm; do NOT examine throat; do NOT place supine
- Controlled airway in OT under general anaesthesia + ENT surgical backup
- IV ceftriaxone 50-100 mg/kg/day post-intubation
Foreign body aspiration:
- Urgent rigid bronchoscopy for extraction
- Back blows and abdominal thrusts (Heimlich) only if child is choking and unable to breathe at all (complete obstruction) — do NOT perform blind finger sweeps
- Do NOT delay for X-ray if total obstruction is suspected
Subglottic haemangioma:
- Oral propranolol 2-3 mg/kg/day — first-line, induces involution; monitor heart rate and blood glucose during initiation; contraindicated in reactive airway disease
Anaphylaxis:
- IM adrenaline 0.01 mg/kg (1:1000 solution = 0.01 mL/kg) into the anterolateral thigh — FIRST priority
- Followed by IV fluids, antihistamines, corticosteroids
Investigations (after stabilisation, cause-directed):
- AP and lateral soft-tissue neck X-ray: steeple sign (croup), thumbprint sign (epiglottitis)
- Chest X-ray: asymmetric lung inflation or unilateral hyperinflation (FB in bronchus), mediastinal mass
- Flexible fibreoptic laryngoscopy (awake, in OPD): gold-standard for laryngomalacia, vocal cord paralysis — dynamic assessment under physiological conditions
- CT neck/thorax: vascular ring (CT angiography), subglottic mass
- Microlaryngoscopy and bronchoscopy (under GA): definitive assessment + biopsy of subglottic lesions
CLINICAL PEARL
The most important single rule for clinical assessment of stridor is: inspiratory stridor localises to the extrathoracic airway (supraglottis, glottis, or subglottis). This rule applies to both acute and chronic stridor and immediately narrows the differential from the entire airway to the larynx and upper trachea. Conversely, an infant with inspiratory stridor since birth that worsens with feeds and improves prone almost certainly has laryngomalacia — the single most common cause of chronic stridor in infancy, accounting for 60-70% of congenital laryngeal anomalies, and one that resolves spontaneously in 90% of cases by 18-24 months. The clinical skill is to distinguish this thriving, well-oxygenated, feed-related stridor from the acute, progressive, obstructive stridor of croup, epiglottitis, or foreign body — because the management is entirely different.
Self-Assessment — Stridor
Stridor is a synthesis topic — it requires integrating anatomy (stridor phase as a localising tool), clinical reasoning (acute vs chronic, cause-specific patterns), and management decision-making (which child needs immediate intervention versus monitoring). Before testing yourself, consider how you would approach a completely new clinical scenario: you encounter a stridulous child for the first time, and you have 30 seconds before you must decide whether to activate the emergency team. The two questions that resolve that decision are: (1) Is this child in immediate distress (SpO₂, work of breathing, cyanosis, tripod position)? and (2) Is this acute new-onset stridor or chronic stridor since early infancy? If the child is in distress or the stridor is acutely new, the emergency pathway activates. If the stridor is chronic, positional, feed-related, and the child is thriving, you have time for a systematic evaluation. Internalising this two-step triage is the practical payoff of this module.
Test yourself with the case-based quiz below.
SELF-CHECK
A 2-year-old is brought to the ED after her parents found her coughing and gagging suddenly while playing with small toys. She now has a persistent harsh expiratory wheeze on the right side only, with reduced air entry on the right. She is afebrile and had no URTI prodrome. What is the most likely diagnosis and first-line management?
A. Croup — prescribe oral dexamethasone and observe for 2-4 hours
B. Epiglottitis — keep upright, call ENT, prepare for airway management in OT
C. Foreign body aspiration in the right main bronchus — arrange urgent rigid bronchoscopy for extraction
D. Bronchiolitis — supportive care with hydration and supplemental oxygen
Reveal Answer
Answer: C. Foreign body aspiration in the right main bronchus — arrange urgent rigid bronchoscopy for extraction
The clinical pattern is classic for right-sided foreign body aspiration: sudden onset while playing with small objects, unilateral wheeze and reduced air entry (right side), afebrile, no URTI prodrome, and age 2 years (exploration age — peak for FB aspiration). Expiratory wheeze and asymmetric air entry suggest a bronchial (right main bronchus — anatomically more vertical) foreign body causing a check-valve partial obstruction. Management is urgent rigid bronchoscopy for foreign body extraction — this is not a medical condition and does not respond to bronchodilators or steroids. Croup presents with barking cough, fever, and URTI prodrome. Epiglottitis presents with fever, drooling, and tripod position. Bronchiolitis presents in infants under 2 years with diffuse bilateral wheeze and crackles in the context of RSV illness.