Page 20 of 34
PE26.8 | Acute Lymphoblastic Leukemia — SDL Guide (Part 2)
Management of ALL
The management of childhood ALL is one of the great success stories of modern oncology — the result of 60 years of iterative clinical trial refinement. Treatment is intensive, multi-agent, risk-stratified, and typically spans 2–3 years. The goals are to achieve remission (blast eradication from marrow and blood), eliminate minimal residual disease (MRD — submicroscopic leukaemic cells detectable by flow cytometry or PCR), prevent CNS and extramedullary relapse, and maintain remission with maintenance therapy long enough to achieve cure.
Phase 1 — Induction (weeks 1–4): The goal is to achieve complete remission — defined as <5% blasts in the marrow and recovery of normal haematopoiesis. Achieved in >95% of children with modern protocols. Standard backbone: vincristine (weekly IV — blocks mitotic spindle via tubulin binding) + prednisolone (or dexamethasone; oral — promotes blast apoptosis via glucocorticoid receptor) + L-asparaginase (IM/IV — depletes asparagine, an amino acid ALL blasts cannot synthesise from scratch, unlike normal cells). Higher-risk patients receive an anthracycline (daunorubicin or doxorubicin — intercalates DNA, inhibits topoisomerase II). CNS prophylaxis via intrathecal methotrexate (IT-MTX) (injected directly into the CSF via LP) is given from induction onward — this has replaced prophylactic cranial irradiation, which caused neurocognitive sequelae.
Phase 2 — Consolidation/Intensification (months 2–8 approximately): Designed to eliminate residual disease and prevent emergence of resistant clones. Agents include high-dose systemic methotrexate (HDMTX) with leucovorin rescue, 6-mercaptopurine (6-MP), cyclophosphamide, cytarabine, and continued intrathecal therapy. Risk stratification determines the intensity of this phase — high-risk patients receive more intensive regimens and may proceed to allogeneic haematopoietic stem cell transplantation (HSCT) if an MRD-positive status persists or relapse occurs.
Phase 3 — Maintenance (~2 years): The longest phase; designed to maintain remission. Core agents: daily 6-mercaptopurine (6-MP) + weekly oral methotrexate. These are given at home with regular clinic monitoring of CBC to ensure adequate but not excessive marrow suppression. Dose intensity during maintenance is critical — underdosing increases relapse risk.
Tumour lysis syndrome (TLS) prophylaxis and management: Rapid blast destruction (especially at induction in high-WBC patients) releases large quantities of intracellular potassium, phosphate, and nucleic acids (metabolised to uric acid). This causes the tetrad of hyperkalaemia, hyperphosphataemia, hyperuricaemia, and hypocalcaemia (secondary to phosphate chelating calcium). Consequences: acute renal failure (urate nephropathy, calcium phosphate precipitation), cardiac arrhythmias from hyperkalaemia, and seizures from hypocalcaemia. Prophylaxis: aggressive IV hydration (2–3× maintenance), allopurinol (xanthine oxidase inhibitor; blocks uric acid synthesis — use BEFORE chemotherapy), and rasburicase (recombinant urate oxidase; rapidly degrades pre-formed uric acid — preferred for high-risk cases or established TLS). Frequent monitoring of electrolytes, uric acid, creatinine, and calcium every 6–12 hours during high-risk induction.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
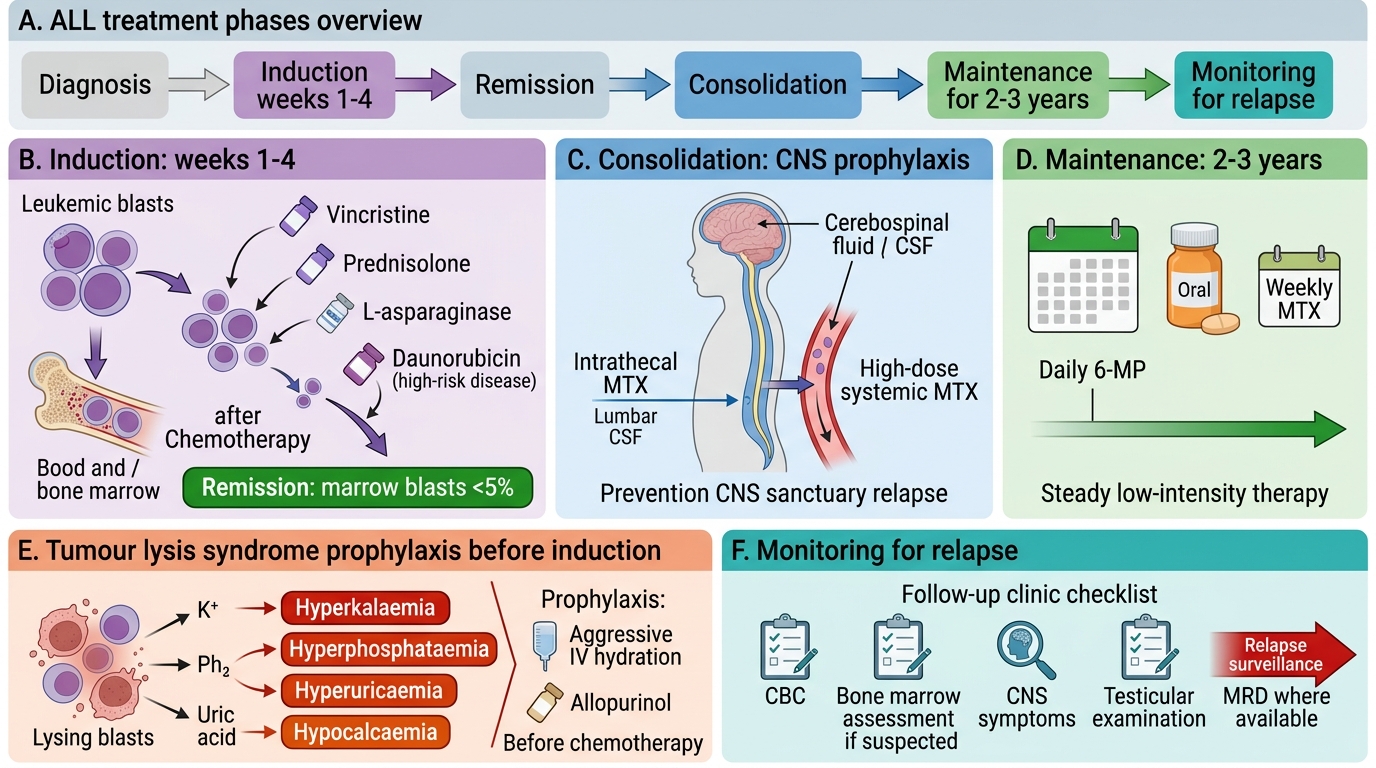
Treatment Phases of Acute Lymphoblastic Leukemia
SELF-CHECK
A 5-year-old boy with newly diagnosed ALL and a WBC of 110,000/µL is about to start induction chemotherapy. Which of the following best describes tumour lysis syndrome (TLS), and what is the FIRST-LINE prophylactic measure?
A. TLS = hypocalcaemia, hyperkalaemia, hypophosphataemia, hypouricaemia; treat with calcium gluconate alone
B. TLS = hyperkalaemia, hyperphosphataemia, hyperuricaemia, hypocalcaemia; prophylaxis with aggressive IV hydration + allopurinol before chemotherapy
C. TLS = hyponatraemia and hypoglycaemia from liver infiltration; prophylaxis with glucose infusion
D. TLS = DIC from blast procoagulants; prophylaxis with FFP
Reveal Answer
Answer: B. TLS = hyperkalaemia, hyperphosphataemia, hyperuricaemia, hypocalcaemia; prophylaxis with aggressive IV hydration + allopurinol before chemotherapy
Tumour lysis syndrome is a metabolic emergency caused by rapid release of intracellular contents from lysing blasts: potassium (hyperkalaemia), phosphate (hyperphosphataemia, which chelates calcium → hypocalcaemia), and nucleic acids → uric acid (hyperuricaemia). Together these can cause acute kidney injury (urate nephropathy), cardiac arrhythmias, and seizures. First-line prophylaxis: aggressive IV hydration (2–3× maintenance) to maximise urinary excretion, plus allopurinol (xanthine oxidase inhibitor) started BEFORE chemotherapy to prevent new uric acid production. Rasburicase is used for high-risk cases or established TLS.
Self-Assessment
Consolidate your learning with this case-based exercise.
Case: A 4-year-old girl presents with 3 weeks of fever, pallor, easy bruising, and bilateral cervical lymphadenopathy. Examination: HR 138/min, pale, axillary and cervical lymph nodes 1.5–2 cm; liver 4 cm and spleen 5 cm below costal margin. CBC: Hb 5.8 g/dL, WBC 94,000/µL, platelets 12,000/µL. Peripheral smear: 78% blasts (fine chromatin, scant cytoplasm).
Q1: What is the most likely diagnosis?
Answer: Acute lymphoblastic leukaemia — the clinical triad of marrow failure (anaemia, thrombocytopenia), hepatosplenomegaly, lymphadenopathy, and blasts on peripheral smear is diagnostic of acute leukaemia. ALL is far more common than AML in this age group.
Q2: What immediate investigations are required before starting treatment?
Answer: Bone marrow aspiration/biopsy (confirm ≥25% blasts + immunophenotyping + cytogenetics), CSF examination (CNS status), chest X-ray (mediastinal mass), baseline electrolytes/uric acid/creatinine/LDH (TLS monitoring), coagulation screen, blood cultures (given fever).
Q3: Why should the house surgeon's suggestion to start prednisolone to 'treat the thrombocytopenia' be rejected?
Answer: Steroids will transiently raise the platelet count in both ITP and ALL (blasts are steroid-sensitive), masking the leukaemia diagnosis, delaying curative chemotherapy, and potentially selecting for steroid-resistant clones. Bone marrow examination must be performed first.
Q4: Her WBC is 94,000/µL. What complication are you most vigilant for at the start of induction?
Answer: Tumour lysis syndrome — aggressive IV hydration and allopurinol are started before chemotherapy. Electrolytes (K+, Ca2+, phosphate), uric acid, and creatinine are monitored every 6–12 hours.
SELF-CHECK
Which cytogenetic finding in childhood B-ALL carries the BEST prognosis and is associated with a good response to antimetabolite-based therapy?
A. BCR-ABL1 (Philadelphia chromosome, t(9;22))
B. KMT2A rearrangement (infant ALL)
C. Hyperdiploidy (>50 chromosomes)
D. Hypodiploidy (<44 chromosomes)
Reveal Answer
Answer: C. Hyperdiploidy (>50 chromosomes)
Hyperdiploidy (>50 chromosomes per blast cell) is associated with the best prognosis in childhood B-ALL — approximately 90% event-free survival with modern therapy. Hyperdiploid blasts accumulate higher intracellular levels of methotrexate and 6-MP polyglutamates, explaining their sensitivity to antimetabolite therapy. BCR-ABL1 (Philadelphia chromosome) historically carried the worst prognosis (now improved with TKI addition); KMT2A rearrangement in infant ALL is also very high risk; hypodiploidy (<44 chromosomes) is associated with poor outcomes.