Page 28 of 34
PE26.{10-15,17} | Hemato-Oncology Examination and Investigations — SDL Guide (Part 4)
Self-Assessment and Consolidation
This section provides a structured self-check across all seven competencies covered in this module. Self-assessment in clinical medicine is more than answering a list of questions — it is the deliberate practice of identifying the boundaries of your own knowledge and skill so that you can target further study and supervised practice. Research on deliberate practice (Ericsson's framework, cited in ciar-std-0013) shows that high-achieving clinicians consistently outperform peers not because of innate talent but because of higher-quality, more targeted self-directed review. This section operationalises that principle: for each competency domain below, first attempt the question from memory, then check your answer against the module content and your cited references (Ghai Ch 14, Nelson Part XIX), and then honestly assess whether you reached the level expected at a final-year MBBS student — SH (supervised hands-on) for examination and smear technique, K (knowledge) for electrophoresis indications and splenectomy indications. Where you find gaps, revisit the relevant section of this module and schedule a practical session on the peripheral smear teaching set or the BMA manikin. The reflective questions at the end are designed for small-group discussion or written portfolio reflection under the Kolb experiential learning cycle (ciar-std-0011): concrete experience → reflective observation → abstract conceptualisation → active experimentation.
Provided image
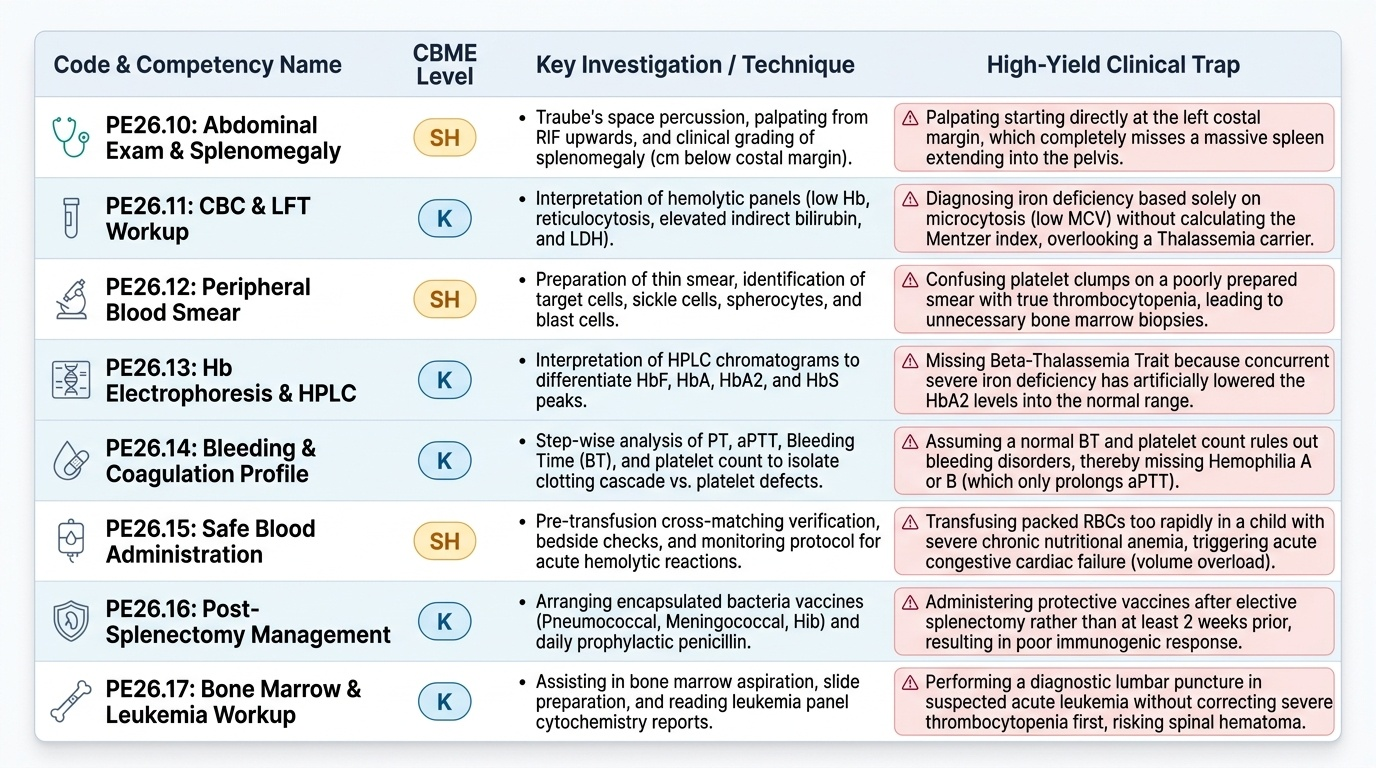
Examination skills (PE26.10):
- Can you demonstrate the correct sequence for abdominal examination in a child with suspected haemato-oncological disease — starting with inspection and Traube's space percussion, then palpation from the right iliac fossa?
- How do you measure and grade splenomegaly? What does a spleen palpable 10 cm below the costal margin suggest in an Indian child?
CBC and LFT interpretation (PE26.11):
- Given a CBC with Hb 7.5 g/dL, MCV 59 fL, RDW 18%, platelets 520,000/µL — what is the likely diagnosis, and what would the peripheral smear show?
- What does unconjugated hyperbilirubinaemia with normal transaminases indicate in a child with anaemia?
Peripheral smear (PE26.12):
- Describe the smear preparation technique: what angle for the spreader slide, which zone to read, and what findings distinguish megaloblastic from IDA?
- What morphological finding is pathognomonic of AML on a peripheral smear?
Haemoglobin electrophoresis (PE26.13):
- A child has HbA2 4.8%. What does this mean, and what is the most important next clinical step?
- Why must iron deficiency be corrected before interpreting HbA2 on electrophoresis?
Bone marrow aspiration (PE26.14):
- What are the two main sites for BMA in children, and what determines the choice?
- What is the most common technical error in BMA aspiration, and how does it affect the result?
Referral criteria (PE26.15):
- List three absolute same-day referral criteria for a child with haematological disease.
- A child with Hb 8 g/dL has completed 6 weeks of iron therapy with no response. What is your next step?
Splenectomy (PE26.17):
- What are the vaccines that MUST be given before elective splenectomy, and what is the minimum age typically observed for hereditary spherocytosis?
- What is OPSI, and why is the risk highest in children under 5 years?
SELF-CHECK
A 3-year-old child with known HbSS sickle cell disease suddenly develops massive splenomegaly over 12 hours with haemoglobin dropping from a baseline of 8.5 g/dL to 4.2 g/dL. What is the most appropriate immediate action?
A. Order haemoglobin electrophoresis to confirm the diagnosis
B. Arrange urgent splenectomy within 24 hours at the primary care centre
C. Administer PRBC transfusion and arrange emergency transfer for acute splenic sequestration crisis
D. Start high-dose prednisolone and observe for 48 hours
Reveal Answer
Answer: C. Administer PRBC transfusion and arrange emergency transfer for acute splenic sequestration crisis
This is an acute splenic sequestration crisis — a haematological emergency unique to sickle cell disease in which large volumes of blood become trapped in the spleen, causing rapid haemoglobin drop and hypovolaemic shock. Immediate management is careful PRBC transfusion (to raise Hb without over-transfusing, as sequestered blood is released on recovery and can cause Hb to overshoot dangerously) and emergency transfer to a tertiary centre. Splenectomy is not an emergency at the primary level, and steroids are not indicated. The diagnosis is clinical and already known; electrophoresis is not the priority.