Page 4 of 34
PE26.{2,5,16} | Iron Deficiency Anaemia — SDL Guide
Learning Objectives
- Describe the epidemiology of iron deficiency anaemia in Indian children and the risk groups most affected
- Explain the pathophysiology of iron deficiency, including the three sequential stages from iron depletion to frank anaemia
- Identify the clinical features of IDA, including symptoms, signs, and features specific to chronic severe deficiency
- Interpret a CBC, peripheral smear, and iron studies to diagnose IDA and distinguish it from thalassaemia trait and anaemia of chronic disease
- Prescribe iron therapy at the correct dose and duration, and counsel caregivers on dietary sources, enhancers, and inhibitors of iron absorption
- Describe the National Anaemia Control Programme, its target groups, IFA supplementation schedule, and monitoring indicators
INSTRUCTIONS
Iron deficiency anaemia is the single most common nutritional deficiency disorder in Indian children, affecting over two-thirds of children under five by national survey data. It is also a preventable condition — one that slips through primary-care encounters because early stages are asymptomatic and the haemoglobin falls gradually. By the time pallor is visible, stores have been depleted for months. This module equips you to diagnose IDA accurately using iron studies, prescribe iron at the right dose for the right duration, and deliver counselling that changes dietary behaviour rather than just handing over a prescription. It also places IDA in the national programmatic context through the Anaemia Control Programme — essential knowledge for community paediatric postings.
References
- Ghai Essential Pediatrics, 9th ed, Ch 17 (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 483 (textbook)
- IAP Guidelines on Management of Iron Deficiency Anaemia, 2020 (guideline)
- National Anaemia Control Programme, MoHFW India (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
An 18-month-old boy is brought to the rural health centre by his grandmother. He has been eating mainly rice gruel and diluted cow's milk since he was weaned at 6 months. He is irritable, not as active as other children his age, and eats soil from the courtyard (pica). His weight is on the 25th centile. On examination: severe conjunctival pallor, tachycardia (HR 132/min), no jaundice, no hepatosplenomegaly. CBC: Hb 7.2 g/dL, MCV 61 fL, MCH 17 pg, RDW 21%, RBC 5.6 × 10¹²/L. You suspect iron deficiency anaemia. What do the iron studies need to show to confirm it? What dose of iron do you prescribe, and for how long? And how do you make sure it doesn't recur?
WHY THIS MATTERS
Iron deficiency anaemia is the most common haematological condition in Indian children and the most prevalent micronutrient deficiency disorder worldwide. India's National Family Health Survey-5 (2019–21) reports that 67.1% of children aged 6–59 months are anaemic — the majority due to iron deficiency. Beyond the haemoglobin number, IDA in infancy and early childhood causes measurable and partially irreversible cognitive deficits: the iron-deficient brain has impaired myelination, reduced dopaminergic neurotransmission, and diminished hippocampal function, translating into lower IQ scores and worse school performance that persist even after iron stores are corrected. IDA also impairs immune function (lymphocyte proliferation, neutrophil killing) and reduces physical work capacity. As a clinician, recognising and treating IDA early — and counselling caregivers effectively — is among the highest-impact preventive interventions available in primary care.
RECALL
Consolidate these prerequisites before proceeding:
• MCV-based classification: IDA is a microcytic (MCV <80 fL) hypochromic anaemia; recall that MCV and RDW together differentiate IDA (high RDW) from thalassaemia trait (normal RDW, Mentzer <13).
• Iron absorption physiology: dietary iron is absorbed as ferrous (Fe²⁺) iron in the duodenum and proximal jejunum; ferric iron in food is reduced by duodenal cytochrome b (DcytB); absorbed iron is exported via ferroportin; hepcidin blocks ferroportin in inflammation, reducing absorption.
• Iron storage: stored as ferritin (the most sensitive marker of body iron stores) in hepatocytes and macrophages; circulating ferritin reflects total body stores proportionally unless an inflammatory state is present (ferritin is an acute-phase reactant and can be falsely normal in infection).
• Haemoglobin cut-offs by age: <11 g/dL for children under 5 years; <11.5 g/dL for ages 5–11; <12 g/dL for adolescent girls 12–14 years.
Epidemiology and Why IDA Tops the Paediatric Anaemia List
Iron deficiency anaemia occupies the top position in the paediatric anaemia hierarchy in India because several powerful risk factors converge during the period of maximal brain and body growth. The first two years of life represent the most iron-demanding period: an infant's blood volume roughly doubles in the first year while the iron available from breast milk (despite its high bioavailability at ~50%) is insufficient to meet demand beyond 4–6 months. This window — sometimes called the weaning gap — is when iron must come from complementary feeds, and it is precisely when most Indian families offer iron-poor foods: rice porridge, diluted animal milk, and vegetable-based preparations with low bioavailability. The result is a near-universal iron gap in infancy that, left unaddressed, progresses silently from storage depletion to frank anaemia before any parent notices.
Key risk groups in the paediatric population:
• Infants 6–24 months: exclusive breastfeeding beyond 6 months without iron-rich complementary foods; premature infants (depleted fetal iron stores — 80% of fetal iron accrues in the third trimester); low-birth-weight infants; twins.
• School-age children in hookworm-endemic areas: chronic intestinal blood loss depletes iron stores even with adequate dietary intake; a single Necator americanus worm loses ~0.03 mL blood/day.
• Adolescent girls: onset of menstruation creates a recurring monthly iron loss of ~30 mg per cycle that is rarely compensated by the typical Indian diet; rapid growth further increases demand.
• Children with cow's milk protein intolerance: cow's milk (>500 mL/day in toddlers) causes chronic occult intestinal bleeding and simultaneously inhibits iron absorption — a double hit.
Presenting picture: the clinical onset is insidious. Parents often attribute pallor and irritability to other causes. Pica — the eating of non-nutritive substances — appears in up to 50% of children with IDA and is an important clinical clue in the history, particularly eating of soil or clay (geophagia) and ice (pagophagia).
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Sequential Stages of Iron Deficiency
Pathophysiology and Aetiology of IDA
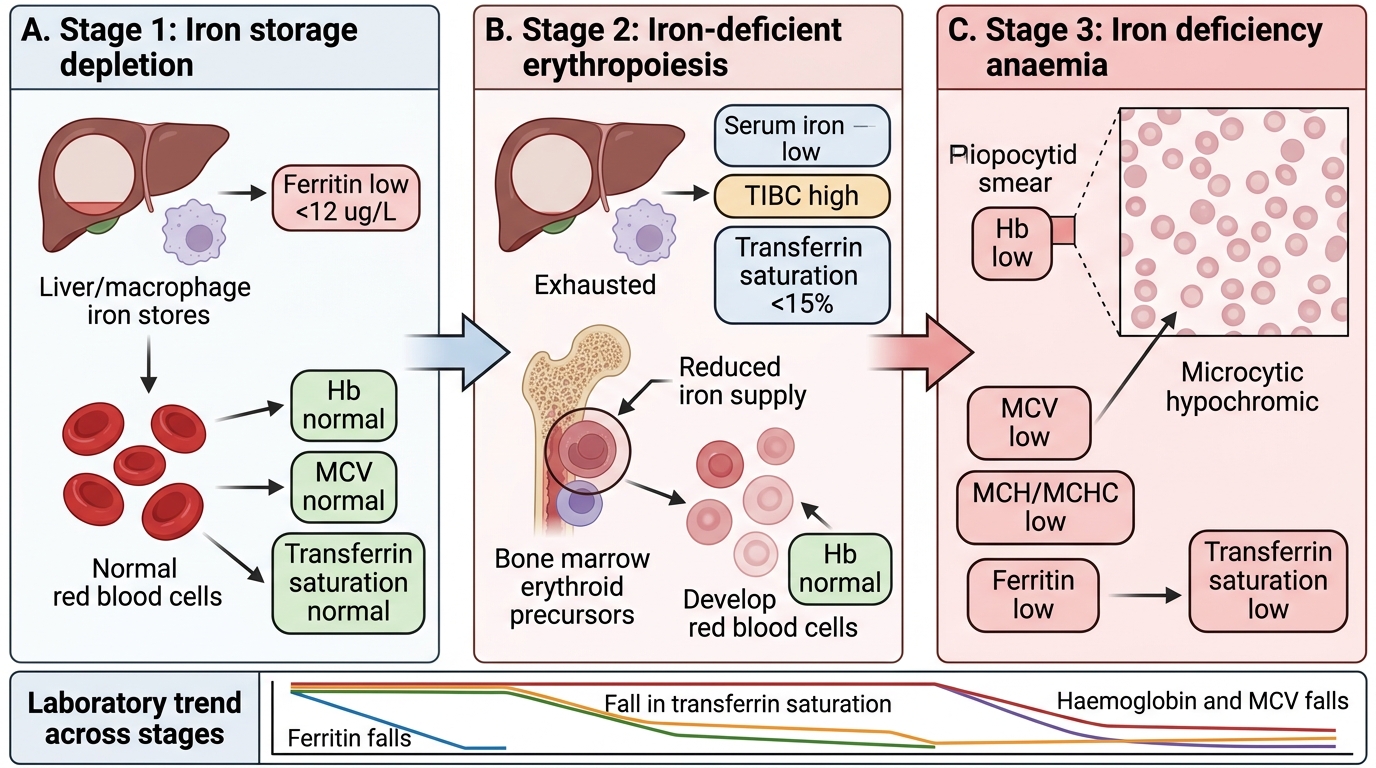
The pathophysiology of IDA proceeds through three sequential stages, each with a distinct laboratory signature, which is why a single CBC at the anaemia stage misses earlier disease. Understanding this progression allows you to diagnose IDA at stage 1 or 2 — before haemoglobin falls — and intervene preventively.
Stage 1 — Iron storage depletion: body iron stores (ferritin) are reduced, but circulating iron (serum iron and transferrin saturation) remains sufficient for erythropoiesis. Haemoglobin and MCV are normal. The only abnormality is a low serum ferritin (<12 µg/L). This is subclinical iron deficiency — no anaemia yet, but stores are empty and any further demand (growth spurt, infection) will precipitate stage 2.
Stage 2 — Iron-deficient erythropoiesis: stores are exhausted; serum iron falls and TIBC (total iron-binding capacity) rises as the body synthesises more transferrin to scavenge iron. Transferrin saturation (serum iron ÷ TIBC × 100%) falls below 15%. Bone marrow erythropoiesis is now substrate-limited, producing slightly smaller, less haemoglobinised cells — MCV may begin to fall, but haemoglobin is still near-normal. Free erythrocyte protoporphyrin (FEP) rises as haem synthesis is blocked but protoporphyrin continues to be produced.
Stage 3 — Frank iron deficiency anaemia: haemoglobin falls below the age-specific cut-off. MCV is microcytic (<80 fL), MCH reduced, MCHC may be low (hypochromic). RDW is markedly elevated (>14.5%, often >18%) as the marrow produces progressively smaller cells while older larger cells circulate simultaneously — creating marked anisocytosis. This is the stage at which most IDA cases in India are clinically diagnosed.
Aetiological causes of IDA in children (Ghai classification):
• Inadequate intake: late introduction of iron-rich complementary foods, exclusive cow's milk diet in toddlers (low iron + absorption inhibitor), cereal-predominant diet with high phytate content
• Increased demand: prematurity, low birth weight, twins (reduced fetal stores), rapid growth in infancy and adolescence
• Impaired absorption: coeliac disease, chronic diarrhoea, intestinal resection, Helicobacter pylori infection (mechanism: HP uses iron preferentially and reduces ascorbic acid)
• Chronic blood loss: hookworm infestation, cow's milk protein-induced enteropathy, Meckel's diverticulum, inflammatory bowel disease; in adolescent girls — menorrhagia
Clinical Features of IDA
The clinical features of IDA in children span a spectrum from entirely asymptomatic (early stages) to life-threatening high-output cardiac failure (severe, long-standing cases). The presenting severity depends on both the absolute haemoglobin and the rate of decline — chronic slow-onset IDA is better tolerated physiologically than acute haemorrhage.
Symptoms: fatigue, lethargy, reduced playfulness, and irritability are the most common parental complaints; in school-age children, declining academic performance and poor concentration are significant early indicators. Dyspnoea on exertion occurs in moderate-to-severe anaemia. Pica — consumption of non-food substances — is present in up to 50% of children with IDA; geophagia (eating soil/clay) is the most common form in Indian children. Anorexia is common and contributes to a vicious cycle of inadequate intake and worsening deficiency.
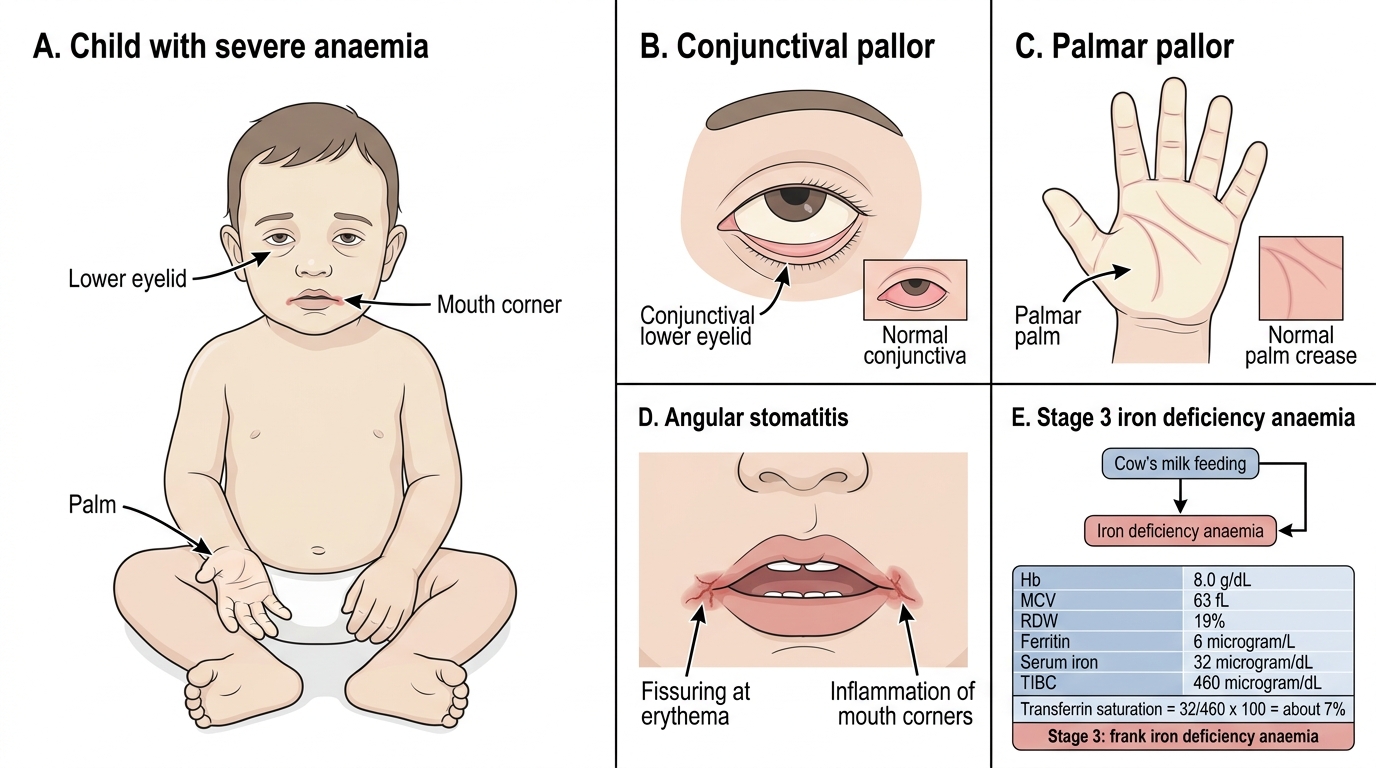
General signs of anaemia: conjunctival pallor (most reliable site), palmar pallor, pallor of nail beds and buccal mucosa. Tachycardia and a systolic flow murmur develop in moderate-to-severe anaemia as the heart increases output to compensate for reduced oxygen-carrying capacity.
Iron-deficiency-specific signs:
• Koilonychia (spoon-shaped nails, lateral ridging) — brittle nails that curve upward; a late sign of severe, chronic IDA
• Angular stomatitis (painful fissures at the corners of the mouth)
• Glossitis (smooth, sore, atrophic tongue — loss of papillae)
• Brittle, fine hair
• Blue sclerae in severe long-standing cases (due to thinning of collagen in the sclera, allowing choroid to show through)
Severe-anaemia signs: Hb <5 g/dL produces high-output cardiac failure — cardiomegaly (hyperdynamic apex, enlarged cardiac silhouette on CXR), hepatomegaly (cardiac failure causing hepatic congestion), oedema, and marked respiratory distress. This is a paediatric emergency.
Neurodevelopmental impact (often underappreciated): iron-deficient infants show reduced activity, social withdrawal, and developmental delays even before frank anaemia. Bayley developmental scores are consistently lower in iron-deficient groups. Some deficits in executive function and attention are not fully reversed even after iron therapy — emphasising the need for early intervention.
Clinical Signs and Laboratory Stage of Severe Iron Deficiency Anaemia
SELF-CHECK
A 14-month-old exclusively cow's milk-fed child has Hb 8.0 g/dL, MCV 63 fL, RDW 19%, serum ferritin 6 µg/L, serum iron 32 µg/dL, TIBC 460 µg/dL. What is the transferrin saturation, and which stage of iron deficiency does this represent?
A. Transferrin saturation ~7%; Stage 3 (frank iron deficiency anaemia)
B. Transferrin saturation ~7%; Stage 1 (storage depletion only)
C. Transferrin saturation ~25%; Stage 2 (iron-deficient erythropoiesis)
D. Transferrin saturation ~7%; Stage 2 (iron-deficient erythropoiesis)
Reveal Answer
Answer: A. Transferrin saturation ~7%; Stage 3 (frank iron deficiency anaemia)
Transferrin saturation = (serum iron ÷ TIBC) × 100 = (32 ÷ 460) × 100 ≈ 7% (normal ≥20%). With Hb 8.0 g/dL (below the <11 g/dL cut-off for under 5 years), MCV 63 fL (microcytic), ferritin 6 µg/L (depleted stores), and low transferrin saturation, this is Stage 3 — frank IDA with all three compartments affected: stores, transport iron, and red-cell haemoglobin. Stage 2 would have low ferritin and low transferrin saturation but Hb still above the cut-off.