Page 5 of 34
PE26.{2,5,16} | Iron Deficiency Anaemia — SDL Guide (Part 2)
Diagnosis and Investigation of IDA
The diagnosis of IDA requires the synthesis of CBC, iron studies, and peripheral blood smear findings. No single test is pathognomonic; the combination of a microcytic hypochromic CBC, low ferritin, elevated TIBC, and low transferrin saturation in the appropriate clinical context is diagnostic without requiring bone marrow examination. The investigation strategy follows a logical hierarchy: the CBC provides the first clue (MCV, RDW), the peripheral smear adds morphological detail (hypochromia, pencil cells), and the iron study panel confirms the aetiology and distinguishes IDA from the two most important mimics — thalassaemia trait and anaemia of chronic disease. Ordering the full iron panel at the first visit is more cost-effective than a sequential approach in a child with strong clinical features of IDA, because it avoids repeat visits and allows definitive diagnosis and prescription in one encounter.
Provided image
CBC findings in IDA:
• Hb below age-specific cut-off
• MCV <80 fL (microcytic)
• MCH reduced (<26 pg)
• MCHC may be low (<30 g/dL — hypochromic)
• RDW markedly elevated (often >18%) — anisocytosis from progressive cell-size reduction as stores deplete
• RBC count may be low-normal or reduced
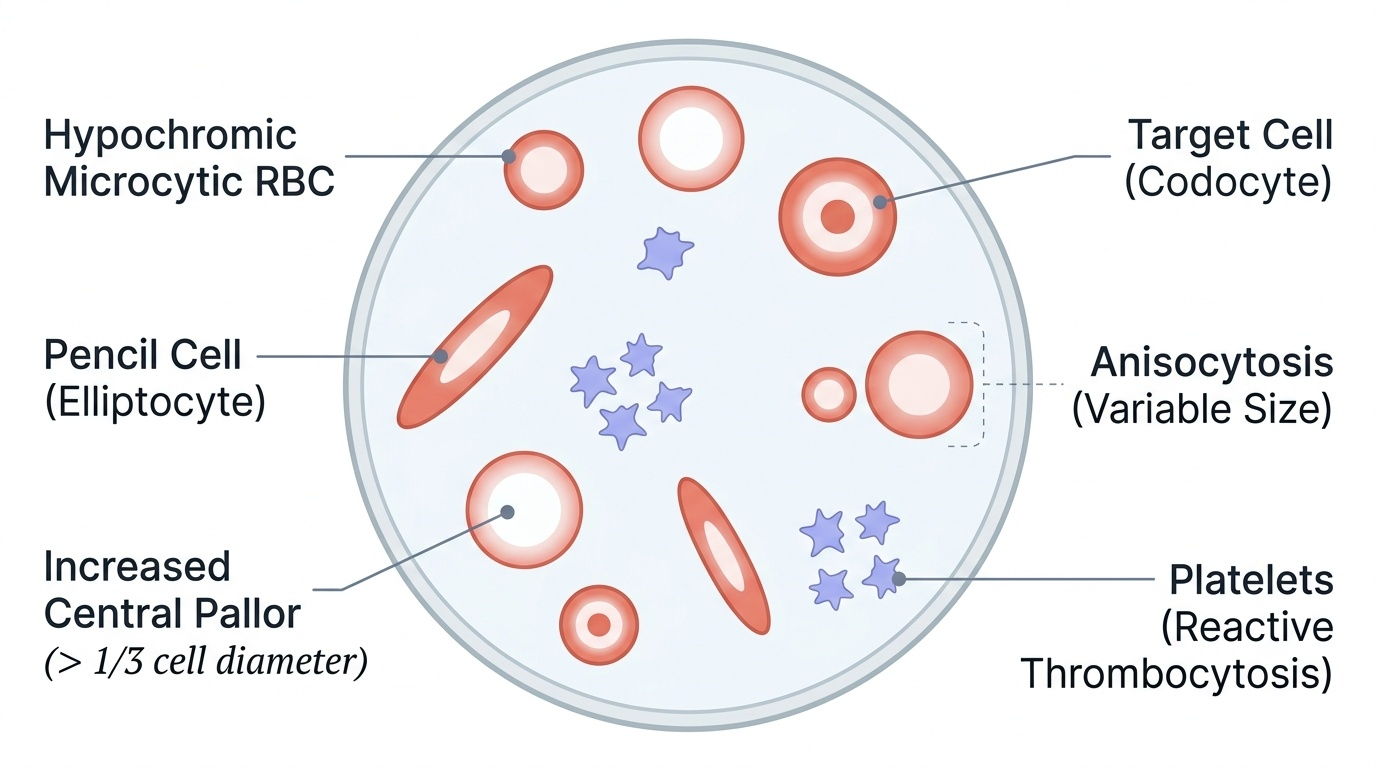
• Platelets are often elevated (reactive thrombocytosis) in IDA — a useful corroborating finding
• Mentzer index (MCV ÷ RBC): >13 favours IDA
Peripheral blood smear: hypochromic (pale) microcytic RBCs with enlarged central pallor (>1/3 of cell diameter), pencil cells (cigar/elliptocyte-shaped cells — highly specific for IDA), target cells in severe cases, and marked anisocytosis.
Iron studies — interpretation:
• Serum ferritin: most sensitive and specific marker of iron stores; <12 µg/L = depleted stores; important caveat: ferritin is an acute-phase reactant — it rises with infection/inflammation, masking IDA. A ferritin in the 12–30 µg/L range in a febrile child should be interpreted cautiously.
• Serum iron: reduced in IDA; also reduced in anaemia of chronic disease
• TIBC (Total Iron-Binding Capacity): elevated in IDA (body upregulates transferrin synthesis to capture scarce iron); reduced in ACD
• Transferrin saturation: <15% in IDA
Differentiating IDA from thalassaemia trait and ACD:
| Parameter | IDA | Thalassaemia Trait | ACD |
|---|---|---|---|
| MCV | ↓↓ | ↓ | Normal or ↓ |
| RDW | ↑↑ (>18%) | Normal or mildly ↑ | Normal |
| Serum ferritin | ↓↓ (<12 µg/L) | Normal | Normal or ↑ |
| Serum iron | ↓ | Normal | ↓ |
| TIBC | ↑ | Normal | ↓ or normal |
| Mentzer index | >13 | <13 | Variable |
| Hb electrophoresis | Normal | HbA2 ↑ (beta-thal trait) | Normal |
CLINICAL PEARL
Serum ferritin is an acute-phase reactant — it rises during active infection or inflammation even when iron stores are depleted. A child with IDA who has a concurrent respiratory infection may have a ferritin of 25–30 µg/L (falsely 'normal'). If clinical suspicion for IDA remains high despite a borderline ferritin, check the CRP or ESR to confirm the inflammatory state, or repeat the ferritin after treating the infection. A therapeutic trial of iron (Hb rise ≥1 g/dL at 4 weeks) is also diagnostic in resource-limited settings.
Management of IDA: Iron Therapy and Dietary Counselling
Effective management of IDA requires not just prescribing iron but prescribing it correctly, for the right duration, with concurrent dietary modification and attention to the underlying cause. The most common failure in IDA management in paediatric practice is stopping iron therapy when the haemoglobin normalises — typically at 4–6 weeks — without continuing for the additional 2 months needed to replenish body iron stores. A child whose Hb corrects but whose ferritin remains depleted will relapse as soon as the next growth spurt or infection places additional iron demand on the body. Treatment success therefore has two measurable endpoints that must both be achieved: a normal haemoglobin AND a ferritin above 30 µg/L. This requires a minimum of three months of continuous therapy, regardless of how quickly the haemoglobin rises.
Provided image
Therapeutic iron — dosing:
• Dose: 3–6 mg/kg/day of elemental iron in 2–3 divided doses (the most commonly cited IAP recommendation is 3 mg/kg/day as a single dose between meals for practical adherence; 6 mg/kg/day is used in severe anaemia or when rapid response is needed)
• Formulation: ferrous sulphate is cheapest and most widely used (each 200 mg tablet = 65 mg elemental iron; paediatric syrups contain 25–30 mg elemental iron per 5 mL); ferrous gluconate is better tolerated gastrointestinally; ferric polymaltose has lower GI side effects but reduced bioavailability
• Timing: between meals (1 h before or 2 h after), not with food — food (especially phytates and calcium) reduces absorption by up to 75%
• Duration: minimum 3 months — first month to normalise Hb, subsequent 2 months to replenish ferritin stores to >30 µg/L
• Response monitoring: reticulocytosis is the earliest response, detectable by day 7–10; haemoglobin should rise ~1 g/dL per week; at 4 weeks, Hb rise ≥1 g/dL confirms diagnosis and adequacy of treatment
Side effects and adherence: nausea, constipation, and dark stools are common; warn the family in advance to prevent premature discontinuation. Iron stains teeth if liquid iron is not diluted or given with a dropper; instruct brushing after each dose.
Parenteral iron (iron sucrose or ferric carboxymaltose) is reserved for: documented malabsorption, intolerance to all oral preparations, non-compliance despite counselling, or inflammatory bowel disease.
Transfusion: reserved for Hb <7 g/dL with haemodynamic compromise or signs of cardiac failure; not indicated for straightforward IDA with Hb ≥7 g/dL.
Dietary counselling (PE26.16 — counsel and educate):
Effective counselling addresses both what to add and what to reduce. It must be practical and culturally feasible — generic advice to 'eat more meat' is not useful in a vegetarian family.
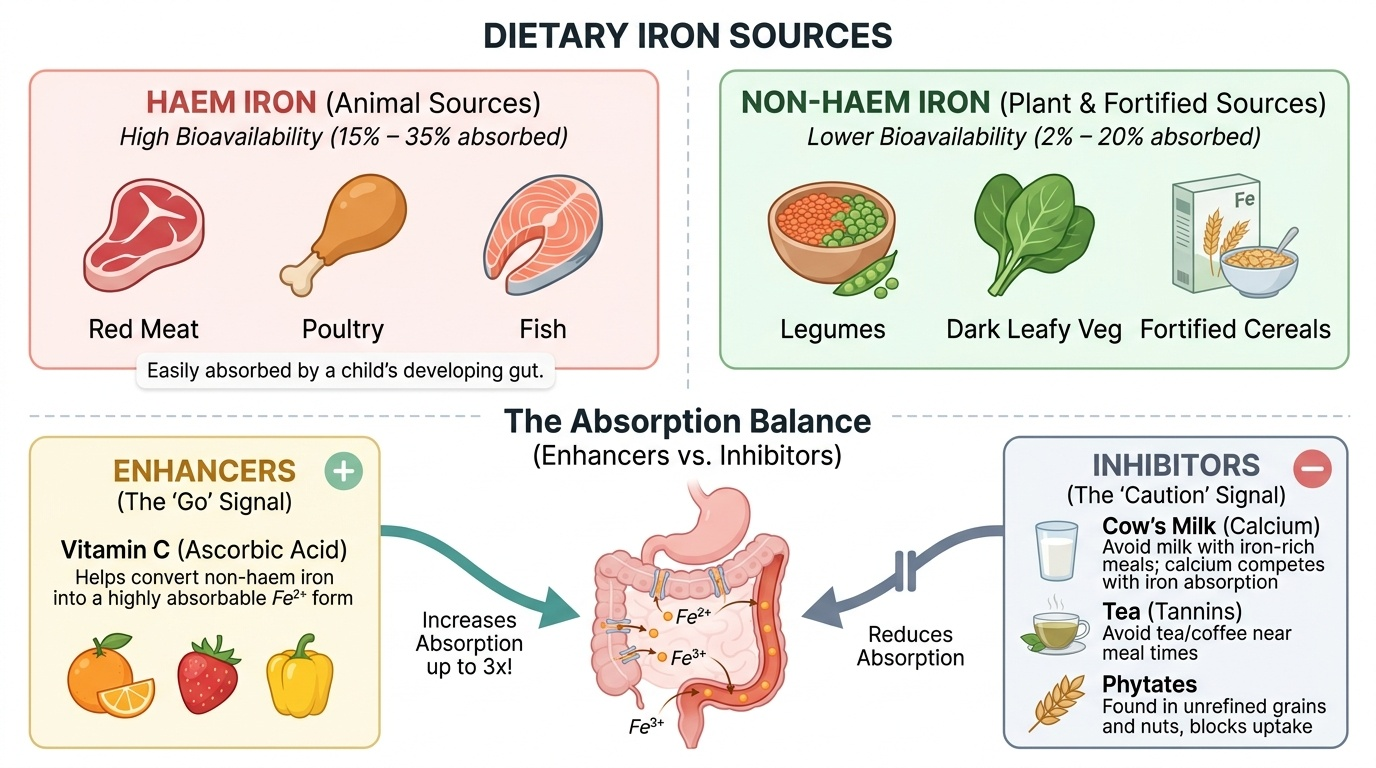
- Haem iron sources (high bioavailability ~25%): red meat, poultry, fish — if culturally acceptable, aim for 3–4 portions/week
- Non-haem iron sources (lower bioavailability ~5–10%): dark leafy vegetables (amaranth/moringa leaves, spinach), legumes (dal, rajma, chana), garden cress seeds (aliv/halim — 100 mg iron/100g in traditional use), iron-fortified cereals
- Vitamin C enhancers: amla, guava, citrus, tomato — taken alongside iron-rich meals increases non-haem absorption 3-fold by reducing ferric to ferrous iron; practical advice: a small cup of amla juice with the dal meal
- Absorption inhibitors to reduce: cow's milk (>200 mL/day in children <2 years competes with iron absorption and causes occult bleeding); tea and coffee (polyphenols chelate iron — avoid within 1 hour of iron-rich meals); excess calcium supplements; phytate-rich unleavened bread (reduce by soaking legumes before cooking and fermenting cereals)
- Complementary feeding timing: introduce iron-rich complementary foods by 6 months — iron-fortified rice cereal or meat puree; do not delay beyond this with breast milk alone
National Anaemia Control Programme
The National Anaemia Control Programme (NACP) is a component of the National Health Mission (NHM) and the POSHAN Abhiyaan (National Nutrition Mission) that aims to reduce the prevalence of anaemia in India's most vulnerable groups through universal supplementation with iron and folic acid (IFA). Understanding this programme is essential for community paediatric postings because it is the primary mechanism through which the majority of India's children receive prophylactic iron — not through hospital prescriptions but through anganwadis, schools, and ASHA workers.
Provided image
The programme has evolved over time and currently operates under the Anaemia Mukt Bharat (AMB — Anaemia-Free India) strategy launched in 2018, which targets six beneficiary groups with a 6×6×6 intervention matrix (6 beneficiaries, 6 interventions, 6 institutional mechanisms). The six beneficiary groups include: children 6–59 months, children 5–10 years, adolescents 10–19 years, pregnant women, lactating mothers, and women of reproductive age (15–49 years).
IFA supplementation schedule under NACP (IAP/MoHFW):
| Target Group | Elemental Iron | Folic Acid | Frequency | Delivery Platform |
|---|---|---|---|---|
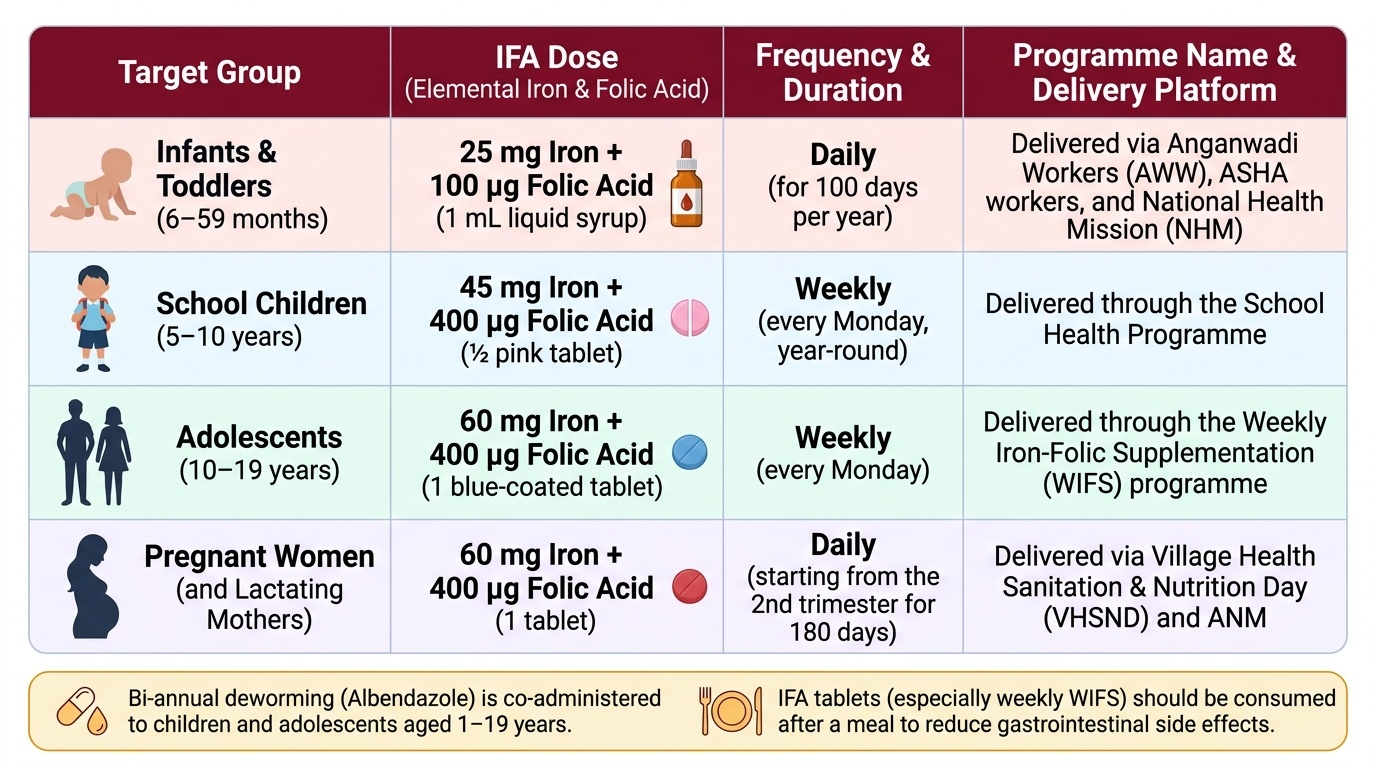
| Infants 6–59 months | 25 mg (1 mL syrup) | 100 µg | Daily for 100 days/year | AWW/ASHA, NHM |
| Children 5–10 years | 45 mg (½ tablet) | 400 µg | Weekly | School health programme |
| Adolescents 10–19 years | 60 mg (1 tablet) | 400 µg | Weekly | WIFS (Weekly Iron-Folic Supplementation) |
| Pregnant women | 60 mg | 400 µg | Daily (180 tablets) | VHSND, ANM |
| Lactating mothers | 60 mg | 400 µg | Daily (180 tablets) | VHSND, ANM |
Note: WIFS (Weekly Iron-Folic Acid Supplementation) is the programme for school-age children and adolescents; it runs every Monday (or the first school day of the week) to maximise visibility and compliance. Side effects (GI upset) are managed by giving the tablet after a meal.
Other interventions under AMB beyond supplementation include: deworming (albendazole biannually for children 1–19 years), point-of-care Hb testing (HemoCue at AWW level), dietary counselling, and behaviour-change communication.
SELF-CHECK
Under the National Anaemia Control Programme (Anaemia Mukt Bharat), a 7-year-old school child in India should receive iron supplementation at which dose and frequency?
A. 25 mg elemental iron daily
B. 60 mg elemental iron daily
C. 45 mg elemental iron weekly
D. 60 mg elemental iron weekly
Reveal Answer
Answer: C. 45 mg elemental iron weekly
Under WIFS (Weekly Iron-Folic Acid Supplementation) for school-age children (5–10 years), the dose is 45 mg elemental iron + 400 µg folic acid, given WEEKLY (not daily). Daily supplementation is for infants 6–59 months (25 mg) and pregnant/lactating women (60 mg). Adolescents 10–19 years receive 60 mg weekly. The 7-year-old falls in the 5–10 year school-child category — 45 mg weekly.
Self-Assessment
Self-assessment in IDA integrates three competencies: diagnosis using iron studies, prescribing iron at the correct dose and duration, and providing counselling that addresses the family's specific dietary practices. Work through the case below independently before reading the analysis — attempt each question without looking ahead, as the diagnostic reasoning and dosing calculation are the skills being tested, not recall of the answers. Pay particular attention to the transferrin saturation calculation and the distinction between correcting haemoglobin and replenishing stores.
Case: Priya, an 18-month-old girl, is brought by her mother to the PHC. She has been on cow's milk and rice gruel diet since 6 months. The mother reports she eats mud occasionally. Examination: moderate conjunctival pallor, HR 128/min, no hepatosplenomegaly. CBC: Hb 8.3 g/dL, MCV 64 fL, RDW 19.5%, platelets 480 × 10⁹/L. Iron studies: ferritin 5 µg/L, serum iron 28 µg/dL, TIBC 450 µg/dL.
Questions:
1. Calculate transferrin saturation. Is this consistent with IDA?
2. What stage of iron deficiency is this?
3. Prescribe iron therapy: specify the exact elemental iron dose (mg/kg) for Priya if she weighs 10 kg, the formulation, timing relative to meals, and total duration of treatment.
4. What three pieces of dietary counselling would you provide to the mother that are specific to this family's diet?
5. Under NACP, which programme should Priya be enrolled in, and what will she receive?
Analysis:
1. Transferrin saturation = (28 ÷ 450) × 100 = 6.2% — markedly low (<15%), consistent with iron-deficient erythropoiesis. Combined with low ferritin (5 µg/L), low serum iron, elevated TIBC, microcytic CBC, and elevated RDW, this is a classic IDA picture.
2. Stage 3 (frank IDA): all three compartments are affected — storage (ferritin ↓), transport (transferrin saturation ↓), and erythropoiesis (Hb <11 g/dL, MCV microcytic).
3. Dose: 3–6 mg/kg/day elemental iron → for 10 kg: 30–60 mg/day. Prescribe ferrous sulphate paediatric syrup (30 mg elemental iron per 5 mL in most Indian formulations) — 5 mL twice daily between meals for the lower end of the dose range. Timing: 1 hour before or 2 hours after meals (not with food). Duration: 3 months minimum (first month corrects Hb; next 2 months replenish ferritin to >30 µg/L). Review Hb at 4 weeks — expect ≥1 g/dL rise.
4. Dietary counselling specific to this family: (a) Reduce cow's milk to maximum 300–400 mL/day — it inhibits iron absorption and causes occult intestinal bleeding; replace calories with khichdi (rice + dal) which provides non-haem iron; (b) Add a small quantity of amla or tomato to the dal meal daily — vitamin C triples non-haem iron absorption; (c) Begin iron-rich complementary foods: cooked green leafy vegetables (amaranth/moringa/spinach) mashed with rice, small portions of egg if acceptable.
5. Priya is 18 months — she falls in the 6–59 months NACP/Anaemia Mukt Bharat category. She should receive IFA syrup: 25 mg elemental iron + 100 µg folic acid daily for 100 days per year through the anganwadi worker or ASHA. She should also receive albendazole for deworming at the next VHND.
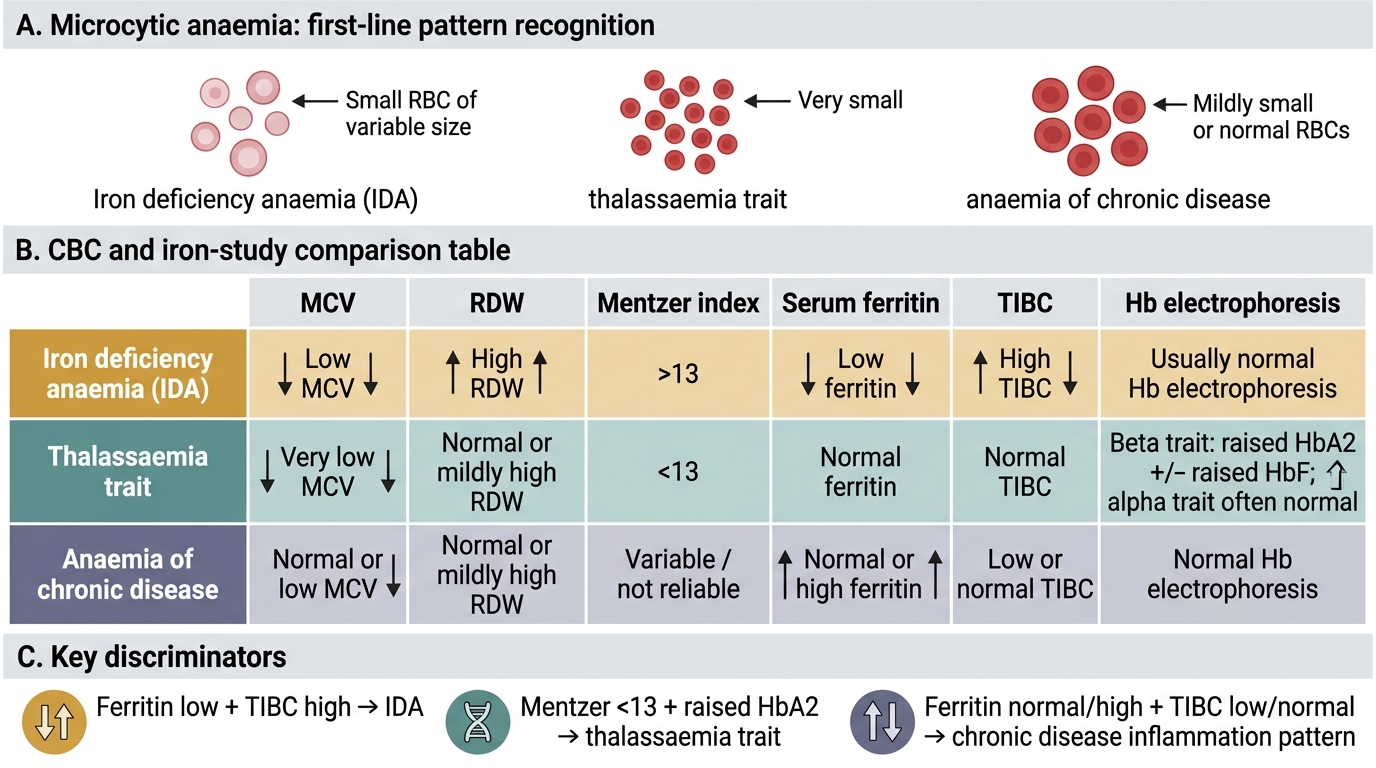
CBC and Iron-Study Patterns in Microcytic Anaemia