Page 22 of 34
PE26.9 | Lymphoma in Children — SDL Guide
Learning Objectives
- Describe the clinical presentation of Hodgkin lymphoma (HL) and common childhood non-Hodgkin lymphomas (NHL), including painless lymphadenopathy, B symptoms, mediastinal mass, and extranodal disease
- Explain the pathophysiology and classification of lymphoma: HL (Reed-Sternberg cells, EBV association, contiguous spread) versus NHL subtypes (Burkitt, T-lymphoblastic, ALCL) and their distinctive epidemiology in children
- Outline the diagnostic approach including excisional lymph node biopsy, histopathology, immunophenotyping, staging with Ann Arbor (HL) and Murphy/St Jude systems (NHL), and investigations for extramedullary disease
- Describe the treatment principles for HL (ABVD-based chemotherapy ± radiotherapy) and aggressive NHL (intensive short-course chemotherapy for Burkitt; ALL-type protocols for T-lymphoblastic lymphoma), including TLS prophylaxis
INSTRUCTIONS
Lymphoma is the third most common childhood malignancy after leukaemia and brain tumours, and it spans two quite different biological entities — Hodgkin lymphoma, with its characteristic Reed-Sternberg cells and predictable nodal spread, and non-Hodgkin lymphoma, a diverse group of aggressive but potentially curable disorders. Understanding how to classify, stage, and initiate treatment for lymphoma is directly examinable and directly applicable in emergency settings where a child with a mediastinal mass or jaw swelling requires urgent safe assessment.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 16 (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Chs. 524–525 (textbook)
- Indian Pediatric Oncology Group (InPOG) Lymphoma Protocols (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 14-year-old boy has noticed a painless lump in his right neck for the past three months. Initially it was the size of a marble; it is now 4 cm and he says more lumps have appeared on the left side. For the past six weeks he has had drenching night sweats that soak his pillow, a fever that comes and goes, and has lost 9 kg despite eating normally. His mother adds that she can feel something 'hard' in his armpit. Chest X-ray shows mediastinal widening. Examination: multiple cervical and axillary nodes up to 4 cm, rubbery and non-tender; no hepatosplenomegaly; no ascites. Could this be infection? Or is this a lymphoma — and which one?
WHY THIS MATTERS
Lymphoma — cancer arising from lymphocytes within lymphoid tissue — is the third most common malignancy of childhood, after leukaemia and brain tumours. It is clinically important for several reasons: first, painless lymphadenopathy is an extremely common presenting complaint in any clinical setting, and distinguishing malignant from reactive nodes requires a structured approach; second, the two broad categories of lymphoma (Hodgkin vs Non-Hodgkin) require fundamentally different staging, treatment, and counselling approaches; third, certain NHL subtypes (particularly T-lymphoblastic lymphoma with mediastinal mass) present as airway emergencies that must be recognised and managed urgently. Early, accurate diagnosis directly translates into curative outcomes — overall 5-year survival for childhood HL exceeds 95% with modern treatment.
RECALL
Activate the following foundations before proceeding:
- Lymph node anatomy and drainage: Cervical nodes drain head and neck; axillary nodes drain upper limb and breast; inguinal nodes drain lower limb; mediastinal nodes drain intrathoracic structures; mesenteric nodes drain the gut. Pattern of involvement guides the clinician to the likely primary site.
- Lymphocyte biology: B lymphocytes undergo affinity maturation and somatic hypermutation in germinal centres of lymph nodes — this is where Reed-Sternberg cells (HL) originate. T lymphocytes mature in the thymus — this is the origin of T-lymphoblastic lymphoma and T-ALL.
- B symptoms in oncology: In the context of lymphoma, the term 'B symptoms' refers to a specific triad — unexplained fever >38°C, drenching night sweats, and unexplained weight loss >10% body weight in 6 months. Their presence is prognostically significant and part of the Ann Arbor staging suffix (A = absent, B = present).
- Contrast with ALL: Lymphoma (particularly NHL at early stages) may present with disease predominantly in lymph nodes and extranodal sites with <25% bone marrow blasts; when marrow blasts exceed 25%, the entity is reclassified as leukaemia (T-ALL or B-ALL). This is a continuum, not a fixed border.
Clinical Presentation of Lymphoma
Lymphoma in children presents across a wide spectrum of clinical pictures depending on the subtype, stage, and primary site of disease. The unifying clinical entry point is persistent lymphadenopathy — nodes that are enlarged for more than 4–6 weeks, firm or rubbery in consistency, non-tender, and failing to respond to a course of antibiotics. In contrast to reactive lymphadenopathy, malignant nodes are typically non-tender (pain is often absent even in bulky disease), do not shrink with time, may be fixed to surrounding tissue in advanced cases, and are accompanied by systemic symptoms that do not fit a simple infective picture. The clinician must assess every enlarged node for these features and resist the temptation to attribute all lymphadenopathy to infection.
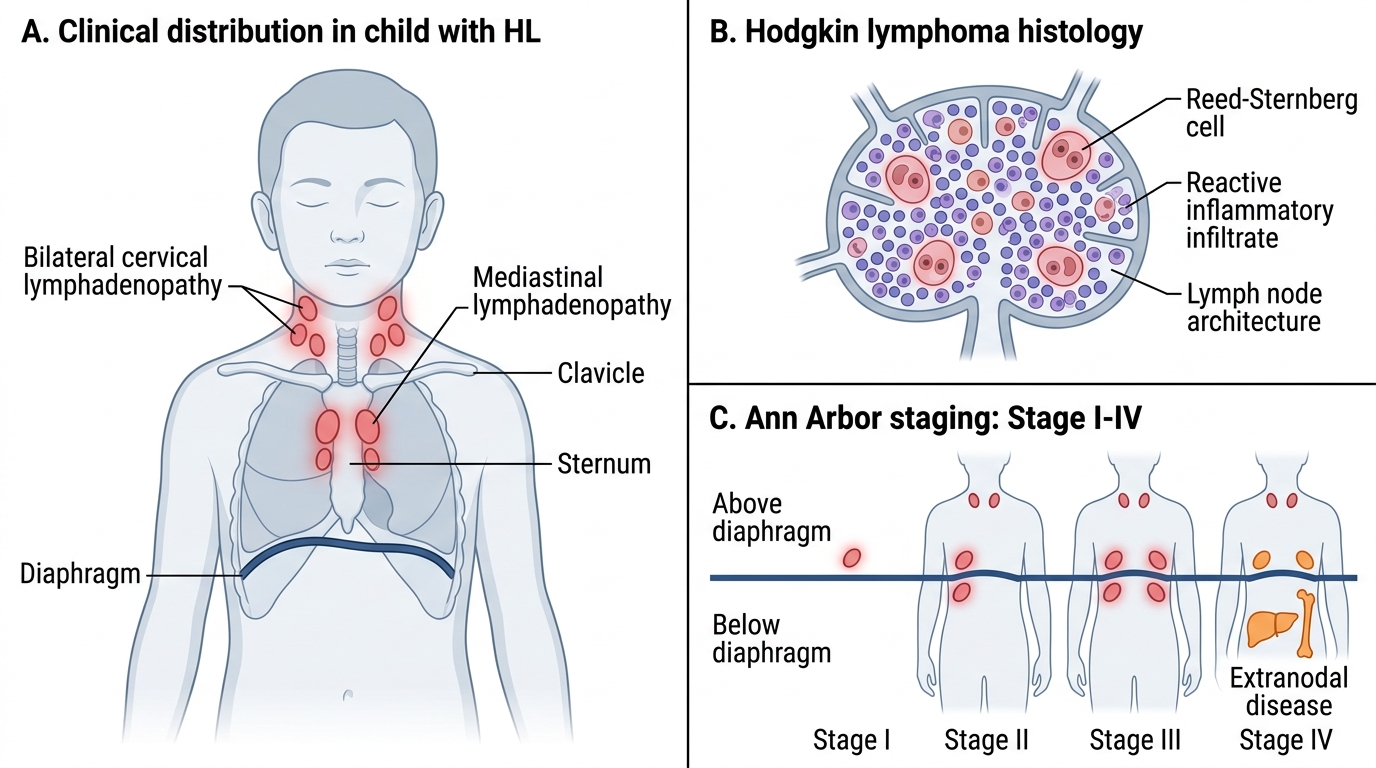
Hodgkin lymphoma (HL) most commonly presents in adolescents and young adults. The cardinal feature is painless, progressive cervical or supraclavicular lymphadenopathy — bilateral in many cases. The nodes are typically described as rubbery in consistency (as opposed to the stony-hard quality of metastatic carcinoma). Mediastinal involvement is common in HL, and a large mediastinal mass may cause cough, dyspnoea, or superior vena cava (SVC) syndrome (facial swelling, arm oedema, distended neck veins). B symptoms — fever (often Pel-Ebstein pattern: cyclical fevers alternating with afebrile periods), drenching night sweats, and unexplained weight loss >10% over 6 months — occur in a significant proportion of HL patients and indicate more advanced or aggressive disease.
Non-Hodgkin lymphoma (NHL) in children presents very differently from HL and from adult NHL. Childhood NHL is almost exclusively high-grade and aggressive, and it has a propensity for extranodal sites:
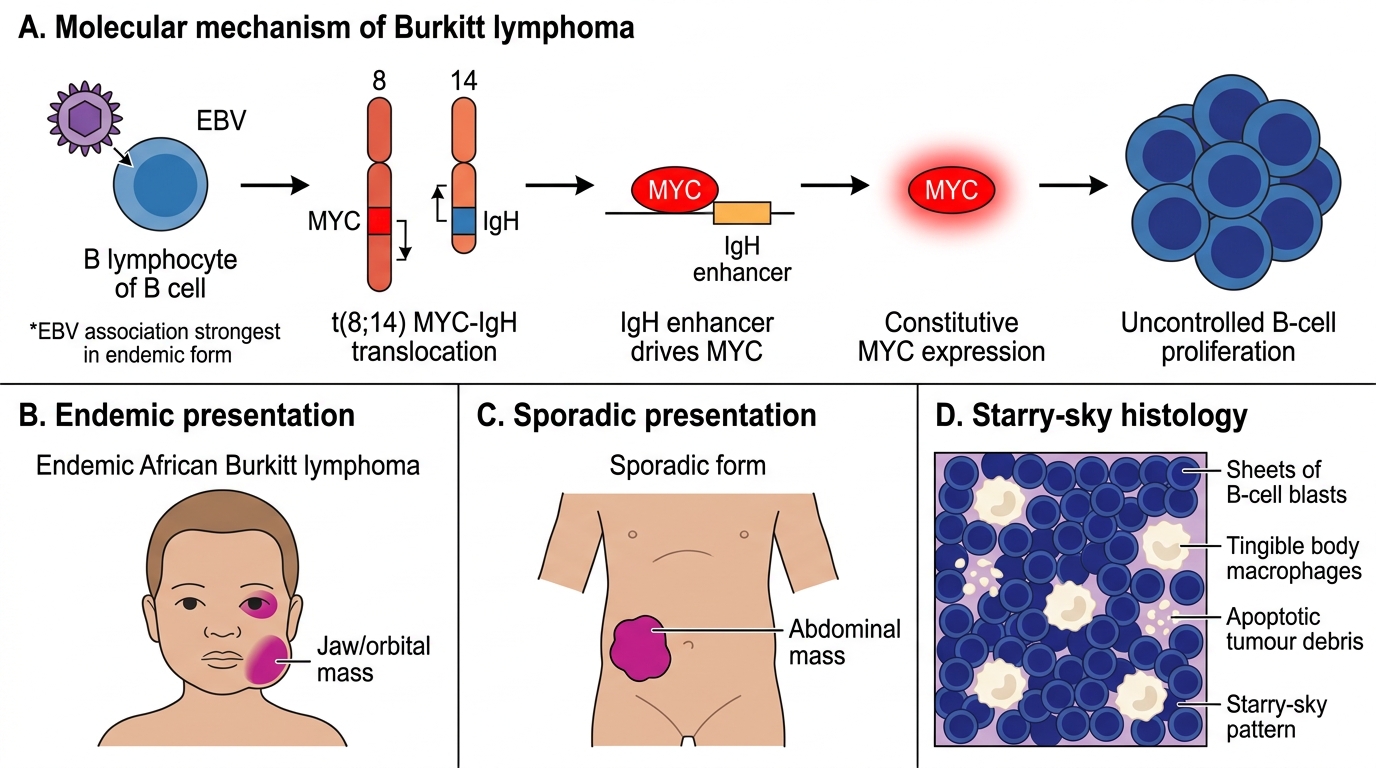
• Burkitt lymphoma (most common childhood NHL): presents as a rapidly growing jaw or orbital mass (endemic African form) or a massive abdominal mass with ascites and bowel obstruction (sporadic form, predominant in India). Abdominal Burkitt can be mistaken for appendicitis or intussusception. The tumour doubles in size every 24–48 hours — the fastest-growing human tumour.
• T-lymphoblastic lymphoma: presents with a mediastinal mass (superior vena cava syndrome, stridor, orthopnoea); bone marrow involvement is common; CNS involvement may occur. When bone marrow blasts exceed 25%, the entity is reclassified as T-ALL.
• Anaplastic large cell lymphoma (ALCL): may present with peripheral lymphadenopathy, skin lesions, and systemic symptoms; often ALK-positive in children with favourable prognosis.
Hodgkin Lymphoma: Clinical Distribution and Ann Arbor Staging
Pathophysiology, Aetiology and Classification
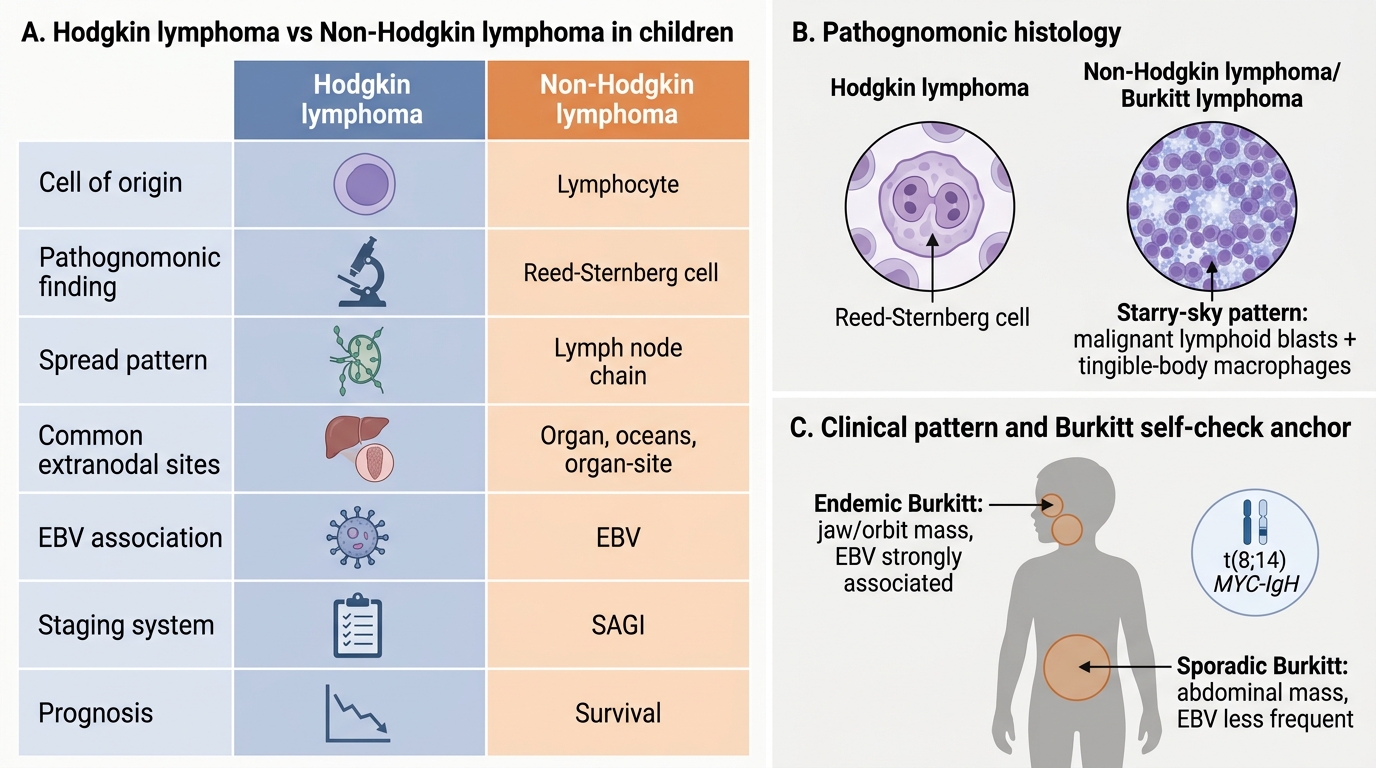
The fundamental biological distinction between Hodgkin lymphoma and non-Hodgkin lymphoma lies in their cell of origin and the mechanism by which the malignant clone evades normal immune control and tissue organisation. Understanding these mechanisms explains the striking differences in clinical behaviour — particularly why HL spreads in an orderly, contiguous pattern while NHL spreads unpredictably and invades extranodal sites early.
Hodgkin lymphoma arises from a B lymphocyte that has undergone somatic hypermutation in the germinal centre of a lymph node but has escaped the normal apoptotic fate of B cells that fail to produce high-affinity antibody. The transformed cell becomes the Reed-Sternberg (RS) cell — a large, binucleate or multinucleate cell with prominent 'owl-eye' nucleoli, which is the pathognomonic histological hallmark of HL. RS cells are few in number but release cytokines that recruit a reactive inflammatory infiltrate of T cells, plasma cells, eosinophils, and macrophages — this reactive infiltrate makes up the bulk of the tumour mass. The histological subtypes of HL (nodular sclerosis, mixed cellularity, lymphocyte predominant, lymphocyte depleted) are defined by the proportion and type of reactive infiltrate around the RS cells. Epstein-Barr virus (EBV) is found in RS cells in approximately 40% of HL cases and is thought to contribute to the oncogenic transformation by driving B-cell survival signalling. HL spreads contiguously — from one lymph node region to the adjacent anatomical station along lymphatic channels — which makes its Ann Arbor staging particularly predictive of treatment requirements.
Non-Hodgkin lymphoma in children is a diverse group of high-grade malignancies, each arising from a different lymphoid precursor at a different stage of differentiation. The most important paediatric NHL subtypes are:
• Burkitt lymphoma: A mature B-cell NHL characterised by the t(8;14) translocation in ~80% of cases (alternatively t(8;2) or t(8;22)), which juxtaposes the MYC proto-oncogene to the immunoglobulin heavy chain (IgH) locus, causing constitutive MYC overexpression and uncontrolled B-cell proliferation. Histologically shows a 'starry-sky' pattern — sheets of blasts with interspersed macrophages that have phagocytosed apoptotic tumour cells. EBV is associated with essentially 100% of endemic (African) Burkitt but only 20–30% of sporadic cases.
• T-lymphoblastic lymphoma: T-cell origin, closely related to T-ALL; mediastinal mass from thymic involvement; managed like T-ALL when marrow blasts ≥25%.
• Diffuse large B-cell lymphoma (DLBCL): Less common in children than adults; CD20+; treated with rituximab-containing regimens.
• Anaplastic large cell lymphoma (ALCL): CD30+, ALK+ in the majority of paediatric cases; the ALK positivity identifies a subtype with better prognosis and targeted therapy options.
HL spreads in an orderly, contiguous manner — from cervical to mediastinal to para-aortic nodes. NHL spreads non-contiguously and commonly involves extranodal sites from the outset. This explains why different staging systems are used: Ann Arbor (designed for HL's contiguous pattern) versus Murphy/St Jude (designed to capture the extranodal and bone marrow involvement common in NHL).
Burkitt Lymphoma: MYC Translocation, Clinical Forms, and Starry-Sky Histology
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
Hodgkin vs Non-Hodgkin Lymphoma in Children
SELF-CHECK
A 10-year-old boy presents with a rapidly growing jaw mass that has doubled in size over 3 days. Biopsy shows sheets of blasts with a 'starry-sky' pattern. FISH confirms t(8;14) translocation. Which diagnosis does this establish, and what is the primary endemic presentation site versus the sporadic form?
A. Hodgkin lymphoma; endemic form presents with mediastinal mass; sporadic form with jaw mass
B. Burkitt lymphoma; endemic (African) form presents with jaw/orbital mass; sporadic form (India/West) presents with abdominal mass
C. T-lymphoblastic lymphoma; endemic form presents with jaw mass; sporadic form with mediastinal mass
D. DLBCL; endemic form presents with jaw mass; sporadic form with lymph node disease only
Reveal Answer
Answer: B. Burkitt lymphoma; endemic (African) form presents with jaw/orbital mass; sporadic form (India/West) presents with abdominal mass
Burkitt lymphoma is confirmed by the 'starry-sky' histology (blasts + macrophages ingesting apoptotic tumour cells) and the t(8;14) MYC-IgH translocation. The endemic (African) form is strongly EBV-associated (~100%) and presents characteristically with jaw/orbital masses. The sporadic form (predominant in India and Western countries, EBV ~20–30%) presents with abdominal mass (often massive, with ascites and bowel obstruction), the commonest presentation in Indian children. Burkitt is the fastest-growing human tumour (doubling time ~24–48 h).
Diagnosis, Staging and Investigation
The diagnosis of lymphoma requires tissue confirmation — imaging and clinical features can suggest the diagnosis but never replace histopathology. The gold standard is an excisional lymph node biopsy, which preserves the nodal architecture and allows definitive classification. In accessible nodes, image-guided core-needle biopsy may provide sufficient tissue in experienced centres, but surgical excision is preferred for initial diagnosis to avoid sampling error. Fine-needle aspiration cytology (FNAC) alone is inadequate for lymphoma diagnosis — it cannot assess nodal architecture, which is essential for distinguishing HL subtypes and many NHL subtypes. This principle must be firmly embedded: a clinical diagnosis of lymphoma, however strongly suspected, is not a basis for initiating chemotherapy or radiotherapy; histological subtyping by immunohistochemistry and molecular studies is required before any treatment decision, because the same presenting lymphadenopathy can be HL, Burkitt, T-lymphoblastic lymphoma, or reactive — each requiring a completely different treatment strategy.
Histopathological findings by subtype:
• HL: Reed-Sternberg cells (large binucleate, 'owl-eye' nucleoli) in a background reactive infiltrate; CD15+, CD30+ by immunohistochemistry; TdT negative (distinguishing from lymphoblastic lymphoma).
• Burkitt NHL: Uniform medium-sized blasts, 'starry-sky' pattern, >95% Ki-67 proliferation index (the highest of any tumour), MYC translocation by FISH.
• T-lymphoblastic lymphoma: TdT+, CD3+, CD7+; mediastinal mass; if marrow blasts ≥25% → reclassify as T-ALL.
• ALCL: CD30+, ALK+ (paediatric form); large anaplastic cells.
Staging systems:
For Hodgkin lymphoma — Ann Arbor staging (suffix A = no B symptoms, B = B symptoms present):
| Stage | Definition |
|---|---|
| I | Single lymph node region |
| II | ≥2 regions, same side of diaphragm |
| III | Both sides of diaphragm |
| IV | Extranodal: bone marrow, liver, lung |
For NHL in children — Murphy (St Jude) staging:
• Stage I: single tumour (extranodal) or single nodal area (excluding mediastinum/abdomen).
• Stage II: single tumour + regional nodes; two or more nodal areas same side of diaphragm; primary GI tumour (completely resected).
• Stage III: two or more nodal areas both sides of diaphragm; mediastinal involvement; unresected abdominal disease; paraspinal/epidural.
• Stage IV: bone marrow (<25% blasts) or CNS involvement (plus any of above).
Investigations:
• CBC (anaemia, thrombocytopenia if marrow involved; eosinophilia in HL); LDH (tumour burden marker — high in aggressive NHL); uric acid (TLS risk); serum albumin, ESR, calcium.
• Chest X-ray and CT chest/abdomen/pelvis for staging.
• PET-CT: now the gold standard for staging and response assessment in HL; particularly valuable for detecting subclinical nodal involvement and assessing remission.
• Bone marrow aspiration and biopsy (bilateral iliac crests) for staging.
• CSF examination for lymphoma subtypes with CNS tropism (Burkitt, T-lymphoblastic).
• EBV serology (relevant for HL and Burkitt epidemiology).
CLINICAL PEARL
The mediastinal mass emergency: When a child with lymphoma (HL or T-NHL) has a large mediastinal mass, the trachea and great vessels may be severely compressed. General anaesthesia relaxes airway musculature and can precipitate complete airway collapse — causing intraoperative respiratory arrest. Never sedate or administer general anaesthesia to a child with an uncharacterised mediastinal mass without first quantifying the tracheal compression (CT or MRI), involving a senior anaesthetist, and having a thoracic surgical team available. In such patients, a diagnostic biopsy under local anaesthesia from a peripheral node (if available) is safer than proceeding to a mediastinoscopy or mediastinal biopsy under general anaesthesia.