Page 23 of 34
PE26.9 | Lymphoma in Children — SDL Guide (Part 2)
Management of Lymphoma
The management of lymphoma in children is risk-stratified by subtype, stage, and disease extent — and the goal in both HL and most NHL is cure. Modern paediatric lymphoma treatment achieves cure rates that are among the best in oncology, and minimising late treatment toxicity (particularly from radiotherapy) is an increasingly important part of therapy planning.
Provided image
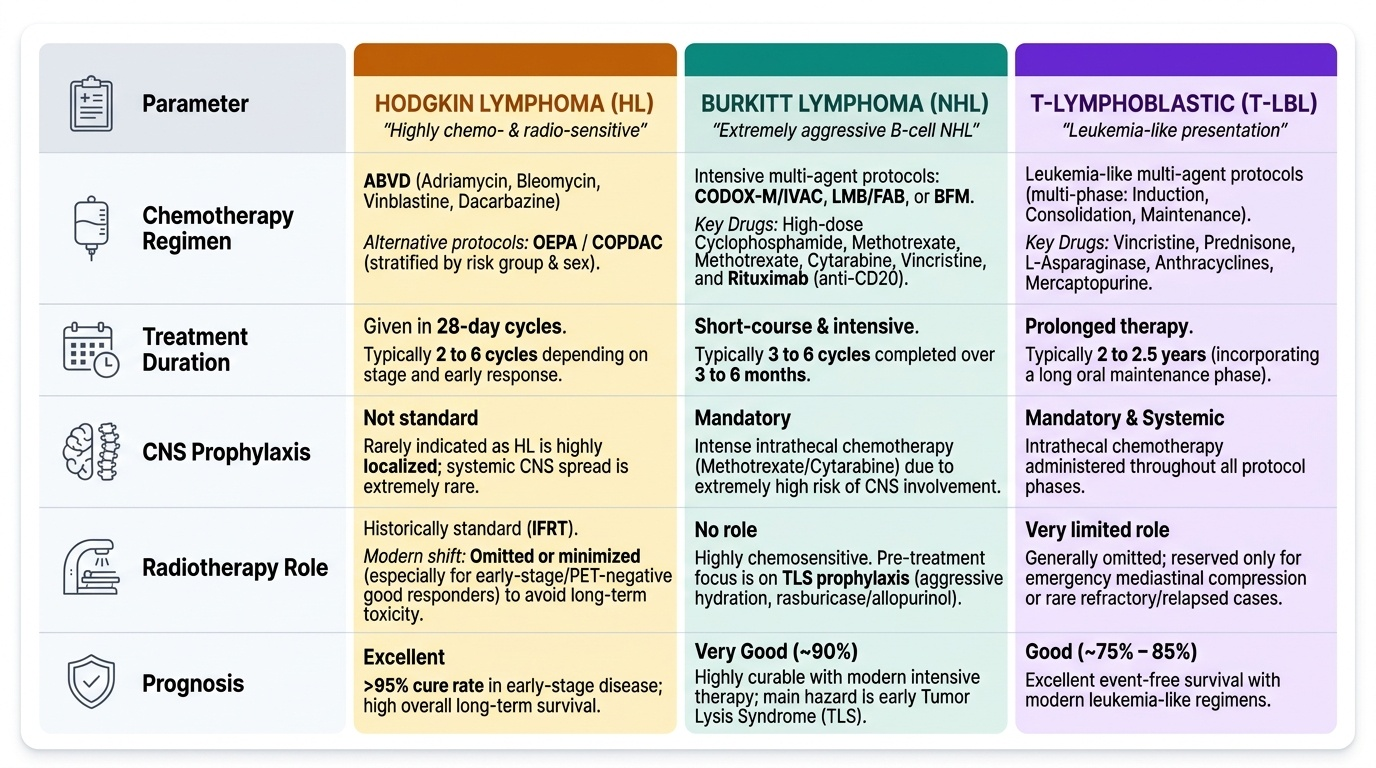
Hodgkin lymphoma:
HL is one of the most chemotherapy-sensitive and radiotherapy-sensitive malignancies. The cornerstone chemotherapy regimen for paediatric HL is ABVD — Adriamycin (doxorubicin), Bleomycin, Vinblastine, Dacarbazine — given in 28-day cycles. Alternative regimens used in paediatric/adolescent protocols include OEPA (vincristine, etoposide, prednisolone, doxorubicin) and COPDAC (cyclophosphamide, vincristine, prednisolone, dacarbazine) based on risk group and sex. Involved-field radiotherapy (IFRT) was historically standard after chemotherapy; in modern paediatric protocols, the aim is to omit or minimise radiotherapy (especially in early-stage/good responders assessed by interim PET) to reduce long-term risks (secondary malignancy, cardiopulmonary toxicity, growth plate effects). Early-stage HL (Stage IA/IIA, no bulky disease, good early response) may achieve >95% cure without radiotherapy in current protocols.
Burkitt lymphoma:
Burkitt is highly chemosensitive but also extremely aggressive — the combination of rapid growth and high TLS risk at initiation of therapy makes it a haematological emergency. Treatment consists of intensive, short-course multi-agent chemotherapy (typically 3–6 cycles over 3–6 months, far shorter than HL) using protocols such as CODOX-M/IVAC, LMB/FAB, or BFM. Key drugs include high-dose cyclophosphamide, high-dose methotrexate, cytarabine, vincristine, and rituximab (anti-CD20, for mature B-cell NHL). CNS prophylaxis with intrathecal methotrexate is mandatory. Tumour lysis syndrome prophylaxis (aggressive IV hydration, allopurinol or rasburicase) must be started BEFORE chemotherapy, particularly in patients with high-bulk disease — large abdominal Burkitt carries one of the highest TLS risks of any tumour.
T-lymphoblastic lymphoma:
When bone marrow blasts are <25%, the entity is staged and treated as NHL (T-lymphoblastic lymphoma) using ALL-type intensive multi-drug protocols (similar to high-risk T-ALL induction/consolidation/maintenance). When marrow blasts ≥25%, it is reclassified as T-ALL and treated on ALL protocols. CNS prophylaxis (intrathecal chemotherapy) is essential given the high CNS tropism.
ALCL:
ALK-positive ALCL is treated with CHOP-based chemotherapy (cyclophosphamide, doxorubicin, vincristine, prednisolone) with good outcomes; targeted therapies (ALK inhibitors) are in clinical trials.
SELF-CHECK
A 14-year-old boy with Stage IIB Hodgkin lymphoma (bilateral cervical nodes + mediastinal mass, with B symptoms) is about to start chemotherapy. Which chemotherapy regimen is the standard backbone for paediatric HL?
A. CODOX-M/IVAC (cyclophosphamide, doxorubicin, vincristine, methotrexate)
B. ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine)
C. CHOP (cyclophosphamide, doxorubicin, vincristine, prednisolone)
D. BFM protocol (methotrexate, cytarabine, thioguanine)
Reveal Answer
Answer: B. ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine)
ABVD (Adriamycin/doxorubicin, Bleomycin, Vinblastine, Dacarbazine) is the classical standard chemotherapy backbone for Hodgkin lymphoma. It was established in clinical trials and remains the cornerstone regimen, often combined with involved-field radiotherapy in advanced stages. CODOX-M/IVAC and BFM protocols are used for aggressive NHL (particularly Burkitt lymphoma). CHOP is used for NHL including DLBCL and ALCL.
Self-Assessment
Apply your knowledge to the following case.
Case: A 14-year-old boy presents with a 3-month history of painless, progressive bilateral cervical and right axillary lymphadenopathy. He has had fever for 6 weeks (temperature 38.5–39°C, coming and going), drenching night sweats, and has lost 9 kg over the past 3 months. Chest X-ray shows a mediastinal mass. CBC: Hb 9.8 g/dL (mild normocytic anaemia), WBC 10,400/µL (normal), platelets 280,000/µL. LDH is elevated. CT chest/abdomen shows bilateral cervical, mediastinal, and right axillary nodes; no abdominal nodal enlargement; no hepatosplenomegaly. PET-CT confirms FDG-avid bilateral cervical, mediastinal, and axillary disease only.
Q1: What is the Ann Arbor stage?
Answer: Stage IIB — disease in two or more lymph node regions (cervical, mediastinal, axillary) on one side of the diaphragm (above); suffix B because fever, night sweats, and >10% weight loss (B symptoms) are all present. (All disease is above the diaphragm = Stage II, not Stage III.)
Q2: Why is a bone marrow biopsy indicated before starting treatment?
Answer: To exclude Stage IV disease (bone marrow involvement), which would change treatment intensity. Marrow infiltration in HL changes Ann Arbor staging to IV and requires more intensive therapy.
Q3: Before scheduling a biopsy under general anaesthesia, what is the most important safety step?
Answer: Quantify tracheal compression from the mediastinal mass with CT/MRI, involve a senior anaesthetist, and be prepared for airway collapse. If peripheral nodes are accessible, peripheral node biopsy under local anaesthesia is safer. General anaesthesia with a large mediastinal mass carries risk of complete airway obstruction.
Q4: What chemotherapy backbone is used for this patient's diagnosis, and what determines whether radiotherapy is added?
Answer: ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) is the standard HL chemotherapy. Whether radiotherapy is added depends on interim PET response after 2–4 cycles (PET-guided adaptive therapy) and the stage/risk group — early complete metabolic responders may omit RT to reduce late toxicity.
SELF-CHECK
A 7-year-old child presents with a massive abdominal mass, ascites, and LDH five times the upper limit of normal. Biopsy shows the 'starry-sky' pattern with Ki-67 >95%. Which of the following must be initiated BEFORE starting chemotherapy?
A. Cranial irradiation to prevent CNS relapse
B. Splenectomy for staging
C. Aggressive IV hydration and allopurinol for tumour lysis syndrome prophylaxis
D. Bone marrow transplant referral
Reveal Answer
Answer: C. Aggressive IV hydration and allopurinol for tumour lysis syndrome prophylaxis
This is Burkitt lymphoma — the fastest-growing human tumour, with massive tumour burden (elevated LDH) and high TLS risk. Before initiating chemotherapy, aggressive IV hydration (2–3× maintenance) and allopurinol (or rasburicase for high-risk) must be started to prevent the metabolic cascade of tumour lysis syndrome (hyperkalaemia, hyperphosphataemia, hyperuricaemia, hypocalcaemia) that can cause acute kidney injury, cardiac arrhythmia, and death. CNS prophylaxis is intrathecal chemotherapy (not cranial radiation); splenectomy is not part of NHL staging; BMT is not the first step.