Page 1 of 11
PE2.1-2 | Failure to Thrive — SDL Guide
Learning Objectives
- Define failure to thrive (FTT) using WHO/IAP growth chart criteria and identify children meeting SAM cut-offs
- Classify FTT into non-organic and organic aetiology and explain the pathophysiological mechanism for each
- Conduct a structured assessment including dietary history, anthropometry (weight-for-age, weight-for-height, MUAC), physical examination, and targeted investigations
- Outline the management of a child with FTT including nutritional rehabilitation (F-75, F-100, RUTF), treatment of the underlying cause, and CSAM protocols
- Counsel the parent of a child with FTT using clear, empathetic communication — explaining the diagnosis, providing practical feeding guidance, and identifying red flags
INSTRUCTIONS
Failure to thrive is among the most common growth problems encountered in paediatric and primary-care settings in India, where undernutrition remains a major public health challenge. Understanding how to identify, assess, and manage FTT — and how to counsel the family — is a core competency for every clinician. This module follows the clinical arc from presentation through assessment to management and parent counselling.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 7 (Growth and Development) and Ch. 8 (Nutrition) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 59 (Failure to Thrive) (textbook)
- WHO/UNICEF: Management of Severe Acute Malnutrition — A Manual for Physicians and Other Senior Health Workers (2013) (guideline)
- IAP Recommended Age-Appropriate Foods for Indian Infants and Young Children (2018) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A mother brings her 18-month-old son to the outpatient department. She says he 'doesn't eat well' and several relatives have commented that he is much smaller than other children his age. On examination the child is quiet and apathetic. His weight is 7.2 kg and his length is 73 cm. When you plot these on the WHO growth chart, you find his weight-for-age falls below −3 SD and his weight-for-height is also below −3 SD. His mid-upper arm circumference (MUAC) is 10.8 cm. A detailed dietary history reveals the child receives only one substantial meal a day; the mother, who has been visibly withdrawn, says she struggles to prepare food regularly. What is happening in this child, and where do you begin?
WHY THIS MATTERS
India carries one of the world's largest burdens of child undernutrition — approximately 35% of children under five are stunted and 19% are wasted (NFHS-5, 2019–21). Failure to thrive (FTT) is not simply a weight problem; it signals a breakdown somewhere in the chain of adequate nutrition, caregiver capacity, or child health. If unaddressed, FTT leads to irreversible cognitive deficits, impaired immune function, increased mortality, and — through the Barker hypothesis — increased risk of non-communicable disease in adulthood. For a practising clinician, recognising FTT early, finding the cause, and empowering the family to act are among the highest-impact interventions in paediatric primary care.
RECALL
Before proceeding, recall these foundational concepts:
• WHO 2006 growth standards are the reference for Indian children aged 0–5 years (adopted by IAP 2015); the IAP 2015 chart extends to 18 years. Growth is plotted as standard deviation scores (z-scores) from the reference median.
• Macronutrients: carbohydrates provide ~50–55% of daily energy, proteins ~15% (essential for cell growth and enzyme synthesis), and fats ~30–35% (essential for neuronal myelination in the first 2 years).
• Holliday-Segar maintenance fluids: 100 mL/kg/day for the first 10 kg, 50 mL/kg/day for the next 10 kg, and 20 mL/kg/day for each additional kilogram above 20 kg.
• Normal weight gain: ~25–30 g/day in the first 3 months, ~20 g/day from 3–6 months, ~10–15 g/day from 6–12 months. Birth weight doubles by 5 months and triples by 1 year.
Understanding Failure to Thrive: Definition and Magnitude
Failure to thrive is defined as a pattern of inadequate physical growth in a young child, typically identified when weight-for-age falls below −2 SD on the WHO growth chart, or when a child crosses two or more major centile lines downward over a period of observation. It is a clinical sign rather than a diagnosis — the task of the clinician is to determine WHY the child is failing to grow. Although height is also affected in chronic undernutrition, weight gain is the earliest and most sensitive indicator of acute nutritional inadequacy; linear growth (height) falters later and signals more prolonged nutritional or hormonal disruption.
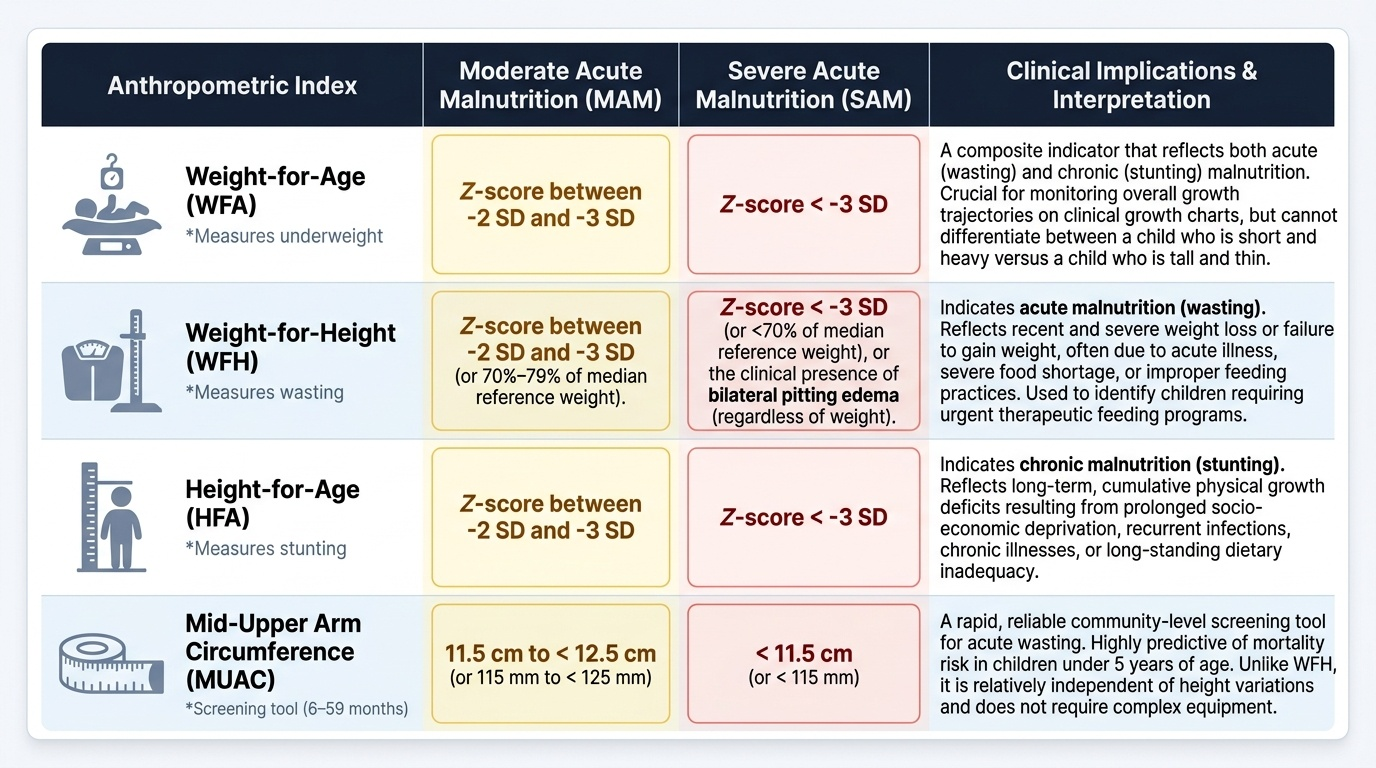
The most severe end of the spectrum is severe acute malnutrition (SAM), defined by ANY of three criteria: (1) weight-for-height below −3 SD on the WHO chart, (2) mid-upper arm circumference (MUAC) less than 11.5 cm in children aged 6–59 months, or (3) the presence of bilateral pitting pedal oedema (kwashiorkor). Moderate acute malnutrition (MAM) is defined as weight-for-height between −2 and −3 SD, or MUAC 11.5–12.5 cm. These thresholds are operationally critical because they govern referral to facility-based care, eligibility for therapeutic food (RUTF), and mortality risk stratification.
In the Indian context, FTT is most prevalent in children aged 6–24 months — the window of complementary feeding — when growth faltering is most dangerous. NFHS-5 (2019–21) data show that wasting affects approximately 19% of under-5 children nationally, with higher rates in states such as Jharkhand (22%) and Bihar (22.9%). Children with SAM face a case fatality rate of 30–50% without treatment.
IMPORTANT NOTE on anthropometric indices: weight-for-age alone is insufficient to classify the type of malnutrition. It must be combined with height-for-age (to detect stunting = chronic undernutrition) and weight-for-height (to detect wasting = acute undernutrition). MUAC is the single most efficient field tool for identifying SAM in children 6–59 months.
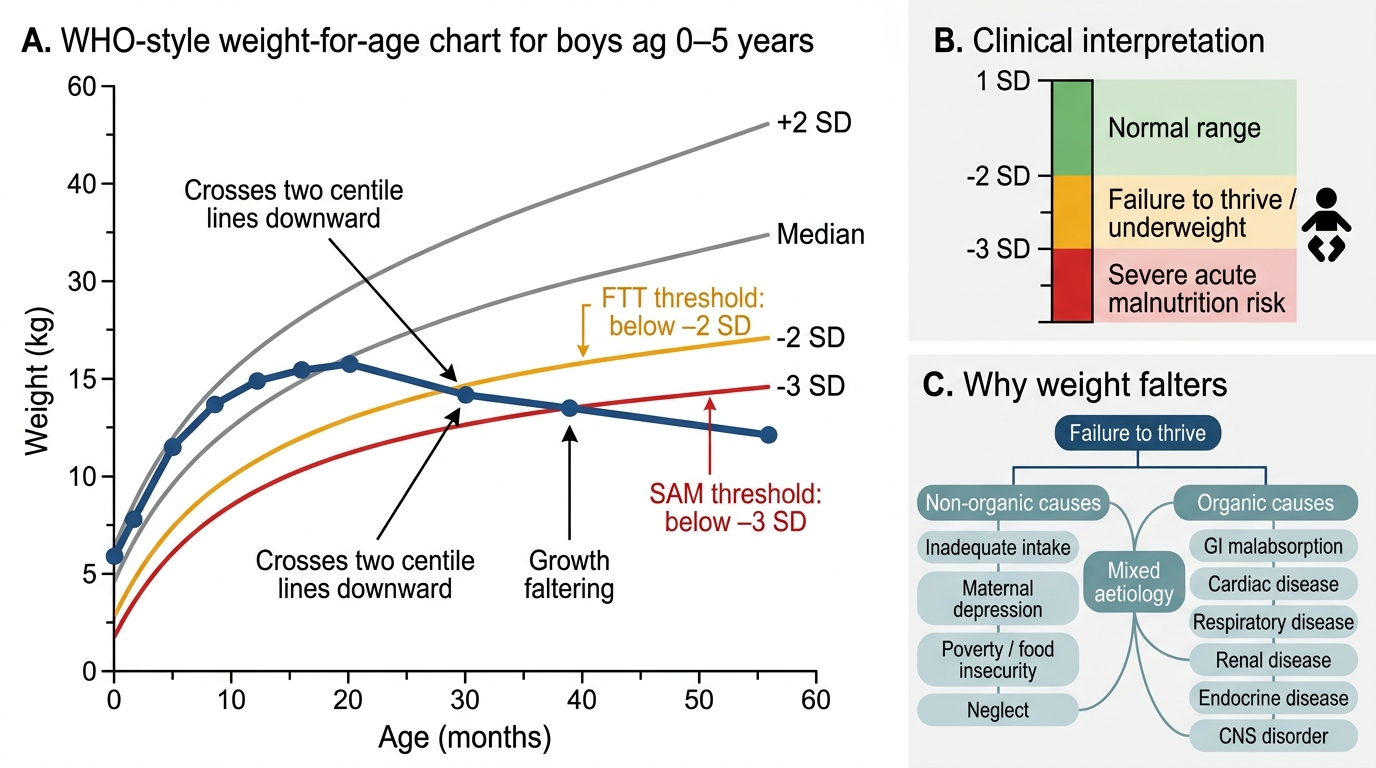
Growth Faltering on WHO Weight-for-Age Chart
Aetiology and Pathophysiology: Why Children Fail to Thrive
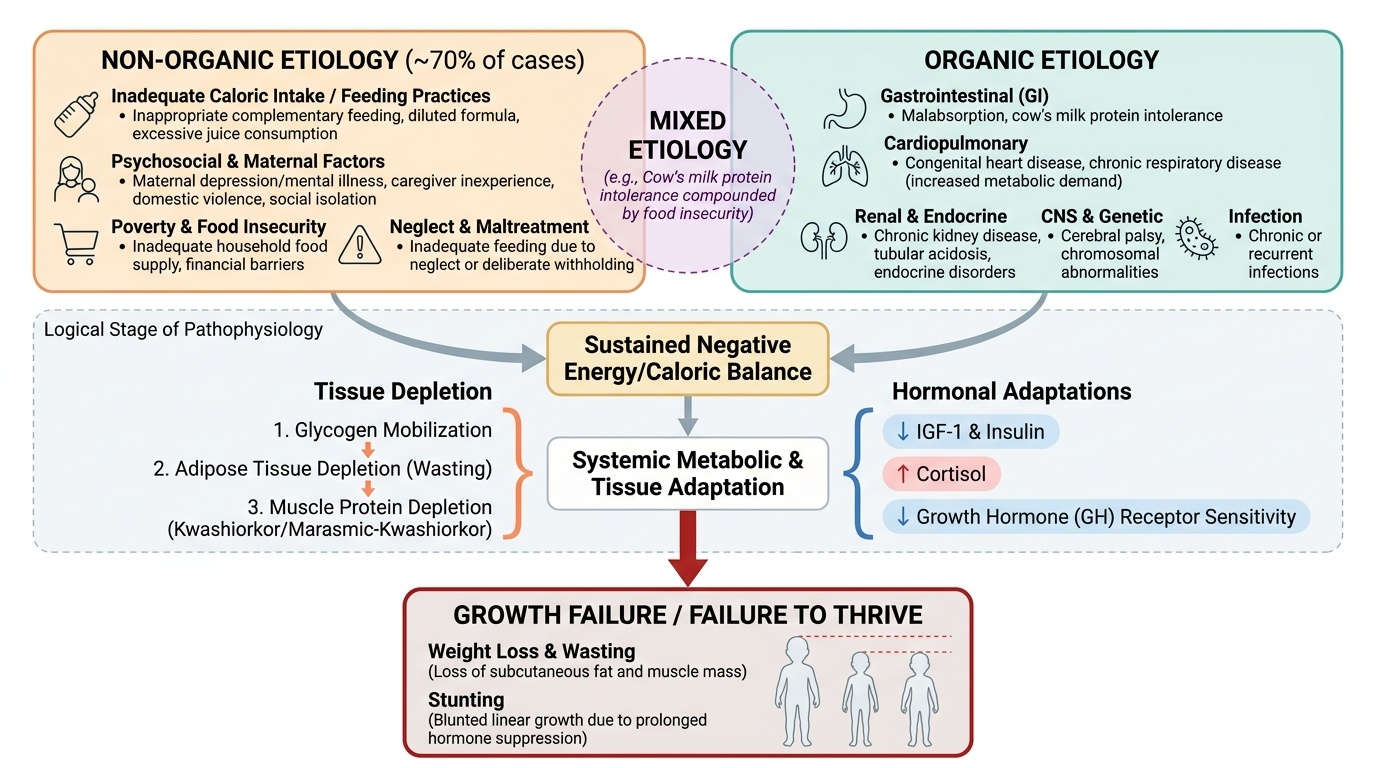
The causes of FTT are broadly divided into non-organic and organic categories. Non-organic causes — where no primary medical disease explains the growth failure — account for the majority of cases, estimated at more than 70% in most paediatric series from both high-income and low-and-middle-income countries. Organic causes include medical conditions that directly impair nutrient intake, absorption, or utilisation. In practice, a third category of mixed aetiology is common: for example, a child with untreated cow's milk protein intolerance may also come from a food-insecure household, compounding the nutritional deficit. The clinical importance of this classification lies in management: non-organic FTT requires behavioural and psychosocial intervention in addition to nutritional rehabilitation, while organic FTT requires specific treatment of the underlying medical condition alongside nutritional support. Missing the non-organic aetiology — particularly maternal depression or neglect — is one of the most common and costly diagnostic errors in paediatric practice.
Provided image
Non-organic FTT arises from an inadequate caloric intake that is not explained by organic disease. Key contributors include:
• Feeding practices: inappropriate complementary feeding (too little, too late, wrong consistency), diluted formula, excessive juice consumption displacing nutrient-dense foods.
• Psychosocial factors: maternal depression or mental illness (one of the strongest predictors), domestic violence, parental substance misuse, caregiver inexperience, or social isolation.
• Poverty and food insecurity: inadequate household food supply, inability to afford appropriate foods.
• Neglect or maltreatment: in a subset of children, inadequate feeding reflects neglect or deliberate withholding of food.
Pathophysiologically, non-organic FTT results in a sustained negative caloric balance. The body initially mobilises glycogen, then adipose tissue (causing weight loss and wasting), and eventually depletes muscle protein (kwashiorkor/marasmic-kwashiorkor). Hormonal adaptation includes suppression of IGF-1 and insulin, elevation of cortisol, and down-regulation of growth hormone receptor sensitivity — collectively blunting linear growth if the deficiency is prolonged.
Organic FTT is caused by a medical condition that may impair intake, absorption, or increased metabolic demand:
| System | Examples | Mechanism |
|---|---|---|
| Gastrointestinal | Coeliac disease, Giardia, cow's milk protein allergy, GERD, pyloric stenosis | Malabsorption or vomiting → reduced net absorption |
| Cardiac | Cyanotic CHD, large VSD/ASD | Increased metabolic demand + early satiety |
| Respiratory | Cystic fibrosis, asthma, BPD | Increased work of breathing → increased caloric need; pancreatic exocrine insufficiency (CF) |
| Renal | CKD, renal tubular acidosis | Metabolic acidosis suppresses growth; anorexia |
| Endocrine | Hypothyroidism, GH deficiency, DM type 1 | Hormone deficiency blunts linear growth and anabolism |
| CNS | Cerebral palsy, hydrocephalus | Feeding difficulties; increased energy expenditure |
| Infections | HIV, TB, recurrent ARI/diarrhoea | Increased catabolic demand; anorexia; intestinal inflammation |
| Chromosomal | Trisomy 21, Turner syndrome | Intrinsic growth limitation |
A unifying pathophysiological consequence across all causes is the cycle of undernutrition: reduced caloric intake → reduced energy for activity and organ maturation → reduced appetite signalling → further reduced intake. Intestinal mucosal atrophy from undernutrition itself impairs absorptive capacity, creating a vicious cycle.
SELF-CHECK
A 9-month-old child has weight-for-height of −3.5 SD on the WHO chart and MUAC of 11.2 cm. There is no pedal oedema. Which of the following best classifies this child?
A. Moderate acute malnutrition (MAM)
B. Severe acute malnutrition (SAM)
C. Stunting without wasting
D. Normal nutritional status for age
Reveal Answer
Answer: B. Severe acute malnutrition (SAM)
SAM is defined by ANY of: weight-for-height < −3 SD, MUAC <11.5 cm (in 6–59 months), or bilateral pedal oedema. This child meets TWO criteria (weight-for-height −3.5 SD AND MUAC 11.2 cm <11.5 cm), confirming SAM. MAM requires weight-for-height −2 to −3 SD and MUAC 11.5–12.5 cm. The presence of bilateral pedal oedema is not required — any single criterion suffices.
Clinical Assessment of the Child with FTT
Assessment of FTT requires a systematic approach integrating history, anthropometry, physical examination, and targeted investigations. The purpose is two-fold: to determine the SEVERITY of growth failure (SAM vs MAM vs at-risk) and to identify the CAUSE (non-organic vs organic, and if organic, which system). A structured, unhurried history is almost always more diagnostically productive than a battery of investigations, particularly for identifying the non-organic causes that account for the majority of FTT cases. Every assessment should begin with a clinical growth chart review — plotting the child's current and any prior measurements to determine whether this is an acute, chronic, or mixed pattern of faltering. The sequence presented below mirrors standard paediatric assessment practice: history first, then physical examination with anthropometry, then targeted investigations guided by clinical findings rather than a fixed panel.
Provided image
History should cover:
• Dietary history: a detailed 24-hour dietary recall and feeding history — breast vs formula feeding, age and adequacy of complementary foods, food preparation, feeding duration and frequency, who feeds the child, and any recent change in feeding. Ask specifically about diluted formula, excessive juice, late introduction of solids, or an abrupt switch from breast to formula.
• Birth and neonatal history: gestational age, birth weight (small for gestational age?), NICU admission, early feeding difficulties, jaundice.
• Past medical history: recurrent diarrhoea, vomiting, respiratory infections, hospitalizations, chronic illness. Specific inquiry for symptoms of organic causes: loose greasy stools (CF/malabsorption), persistent vomiting (GERD/pyloric stenosis), cyanosis (CHD), polyuria/polydipsia (DM).
• Developmental history: meeting milestones? Developmental delay may indicate a CNS cause or severe prolonged undernutrition.
• Family and social history: maternal mental health, caregiver stress, domestic violence, food insecurity, educational level, household composition. These are often the most important determinants in non-organic FTT and are the most commonly missed by time-pressured clinicians.
Anthropometry (must be plotted and interpreted on WHO/IAP growth charts):
• Weight-for-age: identifies overall growth failure
• Height/length-for-age: identifies stunting (chronic)
• Weight-for-height: identifies wasting (acute); use for SAM/MAM classification
• MUAC: measure with a standard MUAC tape at the mid-point of the left upper arm; <11.5 cm = SAM, 11.5–12.5 cm = MAM, >12.5 cm = normal (6–59 months)
• Head circumference: assess for microcephaly (indicates prolonged prenatal/early malnutrition or CNS pathology)
• Growth velocity: if prior measurements exist, plot the trajectory. Crossing ≥2 centile lines downward is clinically significant.
Physical examination: assess for oedema (kwashiorkor), dermatitis, hair changes (flag sign of hair, easy pluckability), angular stomatitis, conjunctival pallor. Look for signs of organic disease: cardiac murmur, hepatosplenomegaly, clubbing, eczema (CMPA), abdominal distension (malabsorption), neurological findings.
Investigations are targeted by clinical suspicion:
• All children: haemoglobin, blood glucose, serum electrolytes, urine routine and culture
• Malabsorption suspected: stool for fat globules, anti-tTG IgA (coeliac), stool microscopy (Giardia)
• Cardiac: echocardiogram
• Renal: renal function tests, urine pH (for RTA)
• Thyroid dysfunction: TSH, free T4
• HIV: as clinically indicated per local exposure profile
• Sweat chloride test: if CF suspected (rare in India but not absent)
• Bone age X-ray (wrist): if short stature co-exists — see SDL pe2-short-stature
CLINICAL PEARL
Maternal depression is the single most under-recognised cause of non-organic FTT. Studies from Indian outpatient clinics show that maternal depressive symptoms are present in 25–40% of mothers of FTT children — yet clinicians rarely ask about it. A brief two-question screen ('Over the past two weeks, have you felt down, depressed, or hopeless?' and 'Have you had little interest or pleasure in doing things?') takes under a minute and, if positive, changes your management plan entirely: the child's nutrition cannot be improved without addressing the caregiver first.