Page 2 of 11
PE2.1-2 | Failure to Thrive — SDL Guide (Part 2)
Management of Failure to Thrive
Management of FTT is always cause-directed, but nutritional rehabilitation is required in all cases regardless of aetiology. The approach depends on severity (SAM vs MAM vs mild FTT without SAM) and the setting (facility vs community).
SAM Management — WHO/UNICEF Protocol:
Children with SAM who have any of the following danger signs require facility-based care: poor appetite (failed appetite test), bilateral pedal oedema, medical complications (hypoglycaemia, hypothermia, severe anaemia, respiratory distress, dehydration signs, altered consciousness).
Phase 1 — Stabilisation (Days 1–7): The F-75 therapeutic milk formula provides 75 kcal/100 mL and 0.9 g protein/100 mL. It is deliberately low in protein and energy to avoid refeeding syndrome (sudden shift in electrolytes — particularly phosphate — when a starved child begins to eat). F-75 is fed at approximately 100 mL/kg/day in 8–12 feeds. During this phase: treat hypoglycaemia (10% dextrose 5 mL/kg IV/NG if glucose <3 mmol/L), prevent hypothermia (clothe, kangaroo care), begin empirical broad-spectrum antibiotics, and give micronutrients (without iron in stabilisation phase — iron can worsen infection in the acutely ill). Do NOT use standard WHO-ORS in SAM; use ReSoMal (reduced osmolarity oral rehydration solution for malnourished children) at 5–10 mL/kg/hr if dehydrated.
Phase 2 — Rehabilitation (Weeks 2–6): When the child's appetite returns and complications resolve, transition to F-100 (100 kcal/100 mL, 2.9 g protein/100 mL) fed at 150–220 mL/kg/day. Encourage gradual return to home foods. Iron supplementation is introduced in this phase. Psychosocial stimulation (play, mother-child interaction activities) is integral.
Community-based SAM without complications: Ready-to-Use Therapeutic Food (RUTF) — Plumpy'Nut (peanut-based, 500 kcal/92 g sachet) — is provided at home. Dose is approximately 200 kcal/kg/day until weight-for-height reaches −2 SD. The child is followed weekly. India's SAM management integrates NRC (Nutrition Rehabilitation Centre) for inpatient and CSAM (Community-based SAM) for outpatient management under NHM.
MAM and mild FTT: Counsel on optimal complementary feeding, micronutrient supplementation (vitamin A, zinc, iron-folic acid), and caloric enrichment of home foods (adding oil, cereals). Fortified blended foods (e.g., Bal Ahar, Poshan Maah programmes) through the ICDS.
Treating the underlying cause: In organic FTT, addressing the cause is essential for sustained improvement — correcting hypothyroidism with levothyroxine, managing GERD with positioning and feeds, referral for cardiac surgery, gluten-free diet in coeliac disease.
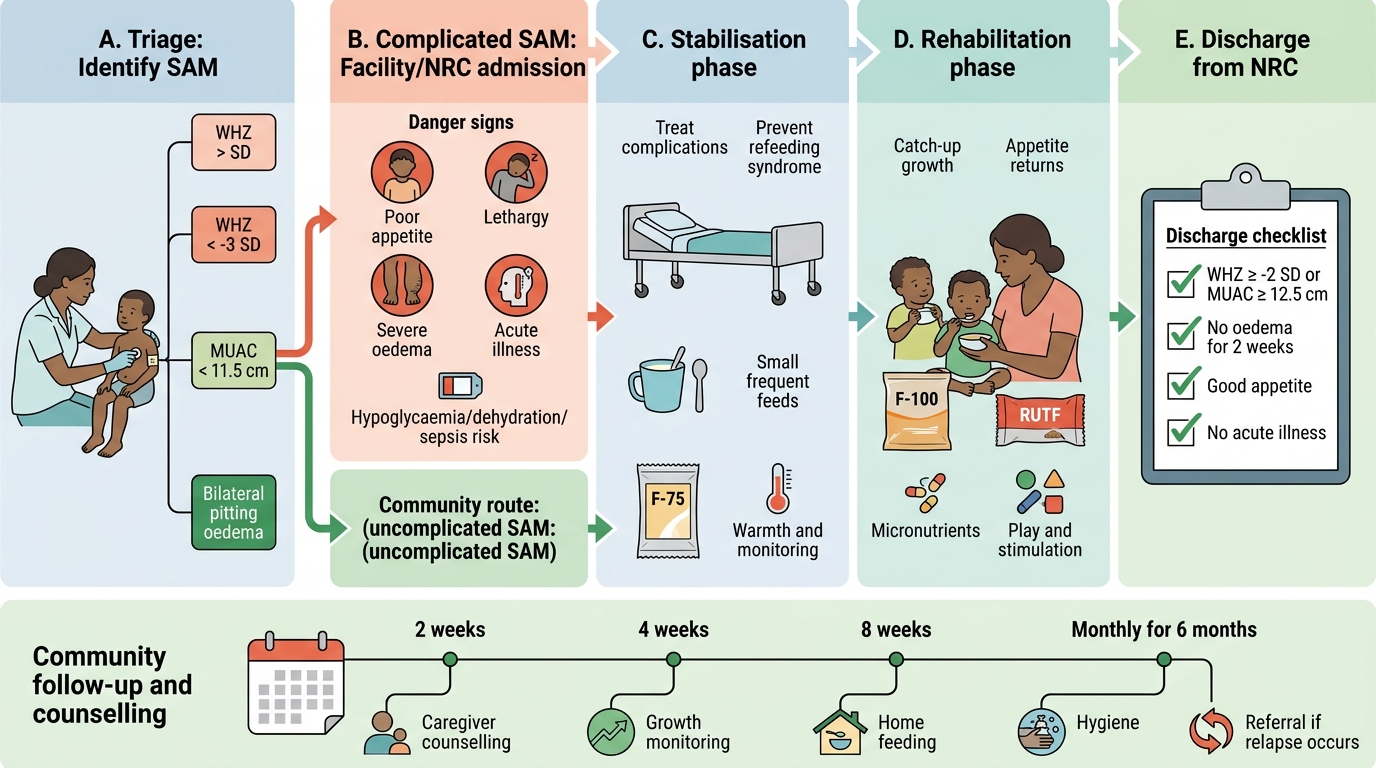
CSAM Pathway for Severe Acute Malnutrition Management
Discharge criteria from NRC: weight-for-height ≥−2 SD (or MUAC ≥12.5 cm), no oedema for 2 weeks, good appetite, no acute illness. Follow-up at 2, 4, and 8 weeks post-discharge, then monthly for 6 months.
Counselling Parents of a Child with Failure to Thrive
Counselling the parent of a child with FTT is a core clinical skill (PE2.2, domain A). The communication approach must be non-blaming, empathetic, and practically actionable — because the goal is to change real-world feeding behaviour and strengthen the caregiver-child relationship, not to assign fault.
Framework for counselling:
1. Build rapport and assess understanding first. Start by acknowledging the parent's concern ('I can see you are worried about your child's growth, and you are right to be concerned — it is important that we address this together'). Explore what the parent already knows or believes about why the child is not growing. Avoid opening with a lecture.
2. Explain the diagnosis clearly and honestly. Use simple language without jargon: 'Your child's weight is lower than we expect for his age, which means he is not getting enough nutrition to grow well. This is something we can work on together.' Avoid value-laden language ('neglect', 'malnourished child' as an accusation). If SAM is diagnosed, explain the seriousness calmly: 'This level of low weight can be dangerous and needs more attention than usual.'
3. Address feeding practices practically. For children 6–24 months: emphasise continued breastfeeding (on demand up to 2 years), complementary food from 6 months (starting with energy-dense semi-solids — soft khichdi with ghee, mashed dal-rice with oil, mashed banana), feeding frequency (3 meals + 2 snacks), and responsive feeding (sit with the child, make feeding a positive, interactive experience, avoid distractions and force-feeding). For older children: advise on food variety, adequate portion size, and limiting dilute fluids before meals.
4. Address psychosocial and structural barriers. If maternal depression is suspected, provide validation and referral: 'It can be very hard to care for a child when you are feeling low yourself — that is not your fault, and there is help available.' Address food insecurity by linking the family to ICDS (Integrated Child Development Services), Anganwadi centre, PM-POSHAN (midday meals for older children), and the NRC where applicable. Educate about hand hygiene and safe food preparation to reduce infection-driven catabolism.
5. Red flags to return immediately. Counsel the caregiver to bring the child back at once if: the child becomes very weak or unresponsive, develops fast breathing (possible pneumonia), has convulsions, refuses all feeds for more than a few hours (failed appetite test), develops swollen feet or face (oedema = SAM), or has profuse watery diarrhoea.
6. Agree on a follow-up plan. Establish a specific date and simple, measurable goals (e.g., 'By the time you come back in two weeks, I expect your child to have gained at least 100 grams'). Written or pictorial instructions for illiterate caregivers improve adherence significantly.
Communication pitfalls to avoid:
• Do NOT use blame language ('You are not feeding your child properly').
• Do NOT overwhelm with too many instructions in one visit (focus on 1–2 actionable changes).
• Do NOT ignore the father or other caregivers — include them where present.
• Do NOT dismiss maternal concerns about the child's appetite or preferences; validate, then redirect.
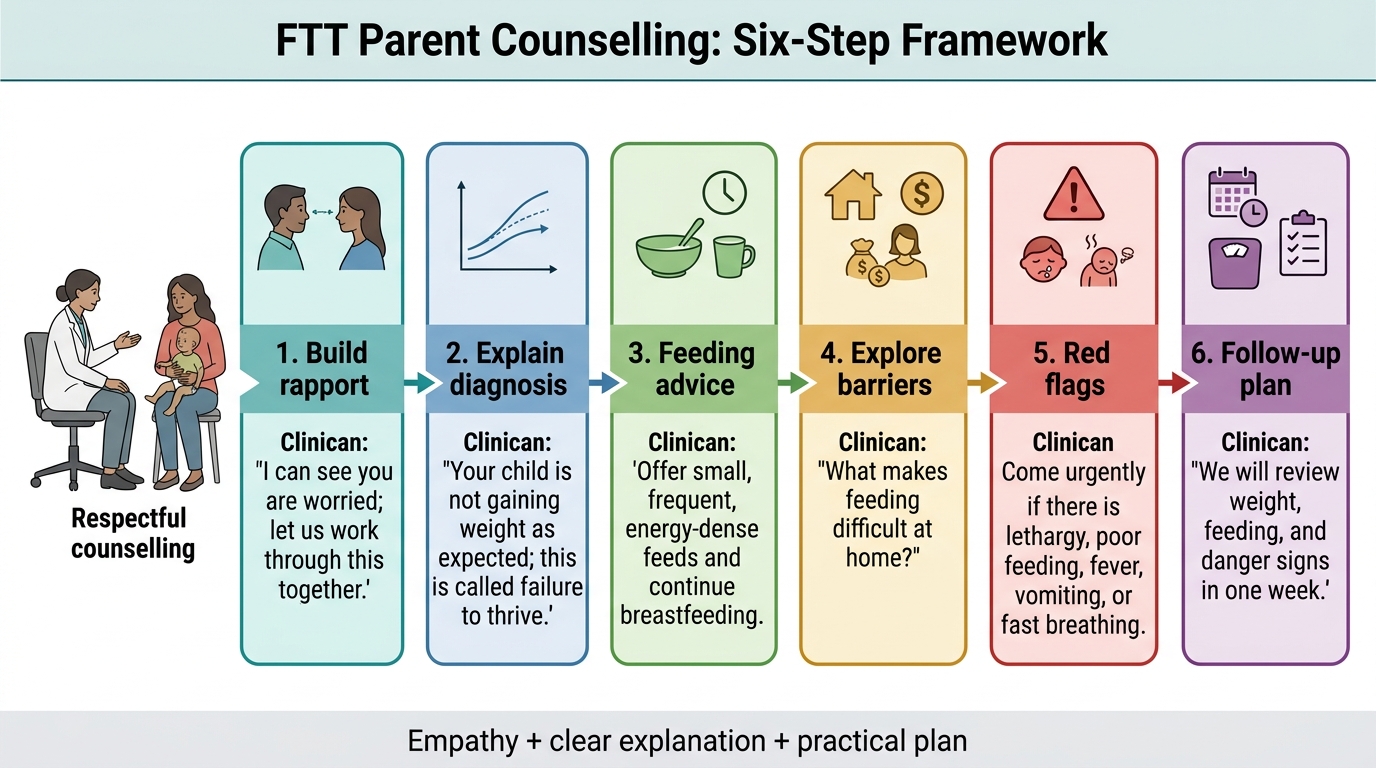
FTT Parent Counselling: Six-Step Framework
SELF-CHECK
A 14-month-old girl with SAM (weight-for-height −3.8 SD, MUAC 10.9 cm) is started on F-75 at the NRC. On day 3, her blood glucose is 2.4 mmol/L and she appears lethargic. What is the immediate first step?
A. Switch immediately to F-100 to increase caloric delivery
B. Give 10% dextrose 5 mL/kg orally or via nasogastric tube and increase feeding frequency
C. Administer IV 50% dextrose 2 mL/kg stat
D. Continue F-75 and recheck blood glucose in 4 hours
Reveal Answer
Answer: B. Give 10% dextrose 5 mL/kg orally or via nasogastric tube and increase feeding frequency
Hypoglycaemia in SAM (blood glucose <3 mmol/L or 54 mg/dL) is treated with 10% dextrose at 5 mL/kg, given orally or by nasogastric tube (preferred over IV to avoid fluid overload and because IV access may be difficult). If IV access is required, 10% dextrose IV is used — NOT 50% dextrose, which is hyperosmolar and dangerous in a malnourished child. Switching to F-100 is done only when the child stabilises and appetite returns (Phase 2). Waiting 4 hours is dangerous — hypoglycaemia in SAM carries high mortality if untreated.
Self-Assessment: Growth Problems and Counselling
This section consolidates the key learning points from the module and offers structured self-assessment prompts. Having worked through the clinical arc — from the definition and epidemiology of FTT, through the non-organic and organic aetiologies, to the structured assessment framework, management protocol, and counselling approach — you are now ready to test your grasp of the integrated picture. Self-assessment at this stage is not about memorising isolated facts but about being able to reason through a clinical problem: given a child's anthropometry, can you classify the severity correctly? Given a history, can you distinguish the most likely aetiology? Given a management question, can you apply the correct protocol? Review the checklist below before attempting the quiz items, and use the reflection prompts to identify any gaps.
Provided image
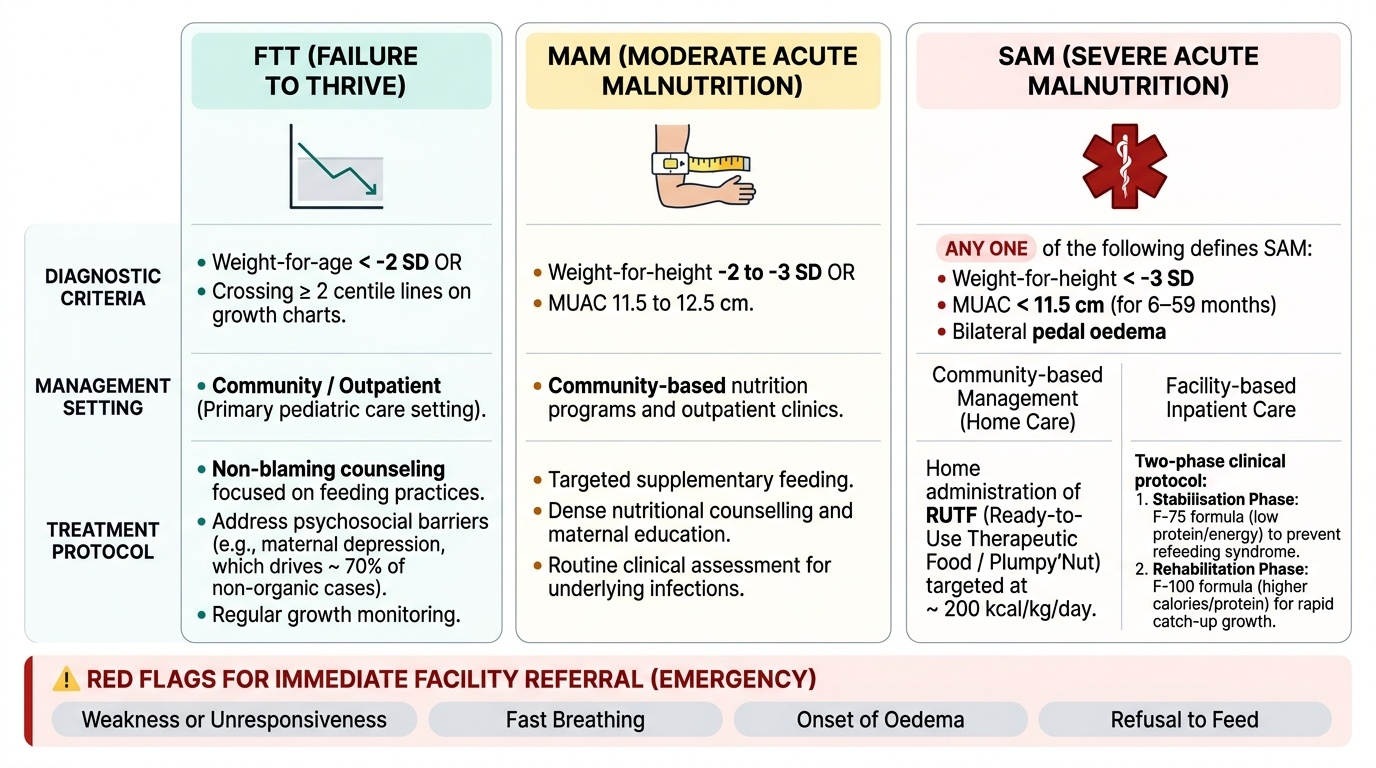
Checklist of must-know facts:
• SAM criteria: weight-for-height < −3 SD, OR MUAC <11.5 cm (6–59 months), OR bilateral pedal oedema — ANY ONE criterion defines SAM.
• MAM: weight-for-height −2 to −3 SD, or MUAC 11.5–12.5 cm.
• FTT = weight-for-age < −2 SD or crossing ≥2 centile lines.
• Non-organic FTT accounts for >70% of cases; maternal depression is a key driver.
• F-75 is used in stabilisation (low protein/energy to prevent refeeding syndrome); F-100 in rehabilitation (higher calories/protein).
• RUTF (Plumpy'Nut) is for uncomplicated community SAM management at ~200 kcal/kg/day.
• Holliday-Segar: 100/50/20 mL/kg/day (10/next 10/each additional kg).
• Counselling must be non-blaming, practically actionable, and address both feeding practices and psychosocial barriers.
• Red flags for immediate return: weakness/unresponsiveness, fast breathing, oedema onset, refusal to feed.
Self-assessment prompts (think through before reading the answers):
1. How does the pathophysiology of non-organic FTT differ from organic FTT in terms of the initial trigger?
2. What is the specific reason iron is withheld during the stabilisation phase of SAM management?
3. Why is standard WHO-ORS replaced by ReSoMal in SAM with dehydration?
4. What does a 'failed appetite test' indicate, and what is the clinical significance?
5. You are about to counsel a mother who is visibly distressed. How does your approach differ from counselling a confident, engaged caregiver?
SELF-CHECK
Which of the following is the MOST appropriate first step in counselling a parent whose 18-month-old child has just been diagnosed with non-organic FTT?
A. Explain the detailed pathophysiology of malnutrition so the parent understands the severity
B. Immediately refer to a social worker without explaining the diagnosis to avoid distressing the parent
C. Acknowledge the parent's concern, explore their understanding, and explain the diagnosis in plain language without blame
D. Prescribe a multivitamin supplement and schedule a follow-up in six months
Reveal Answer
Answer: C. Acknowledge the parent's concern, explore their understanding, and explain the diagnosis in plain language without blame
Effective counselling begins with building rapport and assessing what the parent already understands, then delivering the diagnosis clearly and without blame. Starting with a detailed pathophysiology lecture overwhelms the parent. Withholding the diagnosis is unethical and undermines trust. A six-month follow-up is inappropriate for an active nutritional emergency. The non-blaming, empathetic, practically-oriented approach is the foundation of behaviour change in caregiver counselling.