Page 14 of 48
PE27.4 | Hydrocephalus — SDL Guide (Part 2)
Complications of Untreated Hydrocephalus
Untreated or inadequately treated hydrocephalus causes progressive neurological damage through two mechanisms acting simultaneously: the direct pressure effect of elevated ICP on surrounding brain parenchyma, and the ischaemic injury from compression of the cortical and periventricular blood supply. The white matter immediately surrounding the ventricles — which contains the corticospinal tracts for the lower limbs — is compressed first, explaining why gait and lower-limb spasticity are often early motor signs.
Cognitive and developmental delay:
The most common and most significant long-term consequence of inadequately treated hydrocephalus. Progressive ventricular dilation compresses the periventricular white matter, disrupting myelinated associative fibres. Intelligence is affected, attention and memory suffer, and school performance is impaired. The degree of damage is proportional to the severity and duration of ventricular pressure before treatment.
Visual impairment and blindness:
Optic atrophy results from prolonged pressure on the optic nerves (from raised ICP) or from compression of the optic chiasm by the dilated third ventricle. Papilloedema, if unrelieved, transitions to optic atrophy with permanent visual loss. The optic disc assessment on fundoscopy is therefore a critical monitoring parameter in all children with hydrocephalus.
Epilepsy:
Cortical irritation from periventricular gliosis and ischaemia generates epileptiform activity. Approximately 30% of children with hydrocephalus develop epilepsy, which requires anti-epileptic therapy independent of shunting.
Spastic diplegia (periventricular leukomalacia pattern):
Compression of the periventricular corticospinal tracts — particularly those serving the lower limbs — produces spastic diplegia: bilateral lower-limb spasticity with relatively preserved upper-limb function. This pattern is especially common in hydrocephalus secondary to prematurity and IVH.
Herniation and death:
Untreated progressive hydrocephalus leads to transtentorial or tonsillar herniation from uncontrolled ICP, producing progressive brainstem compression, Cheyne-Stokes breathing, and death. Herniation is the direct cause of death in untreated obstructive hydrocephalus.
CLINICAL PEARL
The sunset sign is a red flag, not a curiosity: When you see tonic downward deviation of the eyes in an infant — sclerae visible above the irises, eyes looking persistently downward — this is raised intracranial pressure from hydrocephalus until proven otherwise. Do not attribute it to a transient reflex in a drowsy infant. Measure the OFC immediately, assess the fontanelle, look for scalp vein distension, and arrange urgent cranial ultrasound or CT. The sunset sign means the ICP has risen enough to compress the midbrain; in an infant with open sutures, this usually means the hydrocephalus has been present and progressing for some time — but it has now reached a threshold requiring urgent intervention.
Management: Medical and Surgical
The definitive treatment of hydrocephalus is surgical, and this has been true since the development of the ventriculoperitoneal shunt in the 1950s transformed what was previously a near-uniformly fatal condition into a manageable chronic one. The two main surgical options today — VP shunting and endoscopic third ventriculostomy — represent fundamentally different strategies: shunting diverts CSF to another body compartment and manages hydrocephalus throughout the patient's lifetime, while ETV creates a new anatomical drainage pathway within the brain and, in appropriate cases, can produce a cure without an implanted device. Medical therapy with acetazolamide reduces CSF production and is used as a temporising measure while awaiting surgery or in selected neonatal cases where spontaneous arrest of hydrocephalus is possible. The choice between VP shunt and ETV is governed primarily by the type of hydrocephalus (communicating vs obstructive) and the age of the child — knowing this dichotomy is the core clinical decision framework for this section.
Medical management (temporary/adjunctive):
• Acetazolamide (carbonic anhydrase inhibitor) — reduces CSF production by approximately 50%; used as a temporising measure in infants awaiting shunt surgery or in post-haemorrhagic hydrocephalus of prematurity where spontaneous arrest is possible; dose 25 mg/kg/day divided; side effects: metabolic acidosis, hypokalaemia, nephrocalcinosis with prolonged use
• Repeated serial lumbar punctures (for communicating hydrocephalus): May temporarily reduce ICP; useful in post-haemorrhagic hydrocephalus of prematurity while awaiting haemolysis of blood products; not sustainable long-term
• Furosemide: Occasionally combined with acetazolamide; not first-line
Ventriculoperitoneal (VP) shunt:
The most common surgical treatment for paediatric hydrocephalus worldwide. A silastic tube diverts CSF from the lateral ventricle (via a burr hole), through a subcutaneous tunnel in the neck and chest wall, to the peritoneal cavity where it is absorbed.
Components: Ventricular catheter → reservoir/valve assembly (one-way pressure-regulated valve) → peritoneal catheter with coiled extra length (to allow for growth).
Complications of VP shunt (high-yield for examination):
• Shunt blockage/malfunction (most common) — obstruction of the ventricular catheter by choroid plexus or debris, or disconnection; presents as recurrence of raised ICP symptoms (headache, vomiting, sunset sign, bulging fontanelle); confirmed by CT (ventricles enlarging); requires shunt revision
• Shunt infection (second most common) — most commonly Staphylococcus epidermidis or S. aureus; risk highest in the first 6 months post-insertion; presents as fever, meningism, and CSF analysis via shunt tap showing pleocytosis; requires shunt removal + IV antibiotics + external ventricular drain, then re-shunting
• Over-drainage (slit ventricle syndrome) — excessive CSF drainage when upright → orthostatic headache (worse standing, better lying); ventricles collapse and intermittently obstruct the valve; managed by reprogramming adjustable valves or using anti-siphon devices
• Shunt erosion/migration — distal catheter migrates; rare
Endoscopic Third Ventriculostomy (ETV):
A neuroendoscopic procedure that creates a new passage in the floor of the third ventricle, bypassing the obstructed aqueduct and allowing CSF to flow directly into the interpeduncular cistern. ETV avoids the need for a shunt device and its associated complications.
Indications: Preferred for obstructive (non-communicating) hydrocephalus — particularly aqueductal stenosis in children >6 months of age. ETV is NOT effective for communicating hydrocephalus (the problem is not obstruction of flow within the ventricular system).
Success rate: Approximately 60–80% in children >6 months with aqueductal stenosis; lower in infants <6 months and in post-meningitis or post-haemorrhagic hydrocephalus.
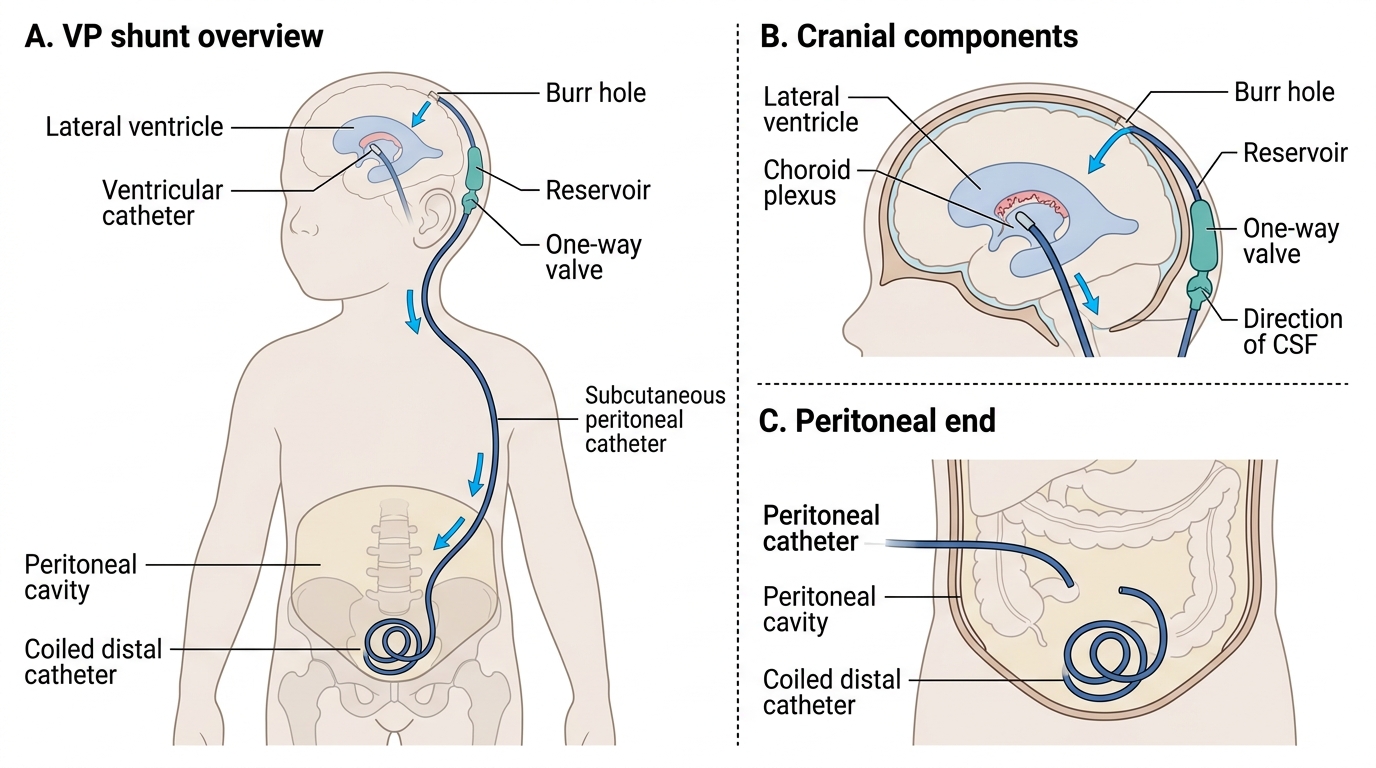
Ventriculoperitoneal Shunt Anatomy
SELF-CHECK
A child with VP shunt for hydrocephalus presents with fever, neck stiffness, and headache 3 months after shunt insertion. CSF via shunt tap shows WBC 450/mm³ (70% neutrophils). What is the most likely diagnosis and initial management?
A. Shunt blockage — immediate CT and shunt revision
B. Viral meningitis — supportive care and observation
C. Shunt infection — shunt removal, IV antibiotics, external drain, then re-shunting
D. Over-drainage syndrome — switch to anti-siphon valve
Reveal Answer
Answer: C. Shunt infection — shunt removal, IV antibiotics, external drain, then re-shunting
Fever, meningism, and CSF pleocytosis (especially neutrophilic) from a shunt tap within the first 6 months of insertion is shunt infection until proven otherwise. The commonest organism is coagulase-negative Staphylococcus (S. epidermidis), followed by S. aureus. Management requires: shunt removal (the infected hardware must come out), IV antibiotics (typically vancomycin ± gram-negative coverage), an external ventricular drain for CSF diversion, and re-shunting after CSF is sterile. Shunt blockage presents with raised ICP symptoms but without fever or CSF pleocytosis. Over-drainage is an orthostatic headache pattern without fever.
Self-Assessment
The following scenarios are designed to test your ability to classify, diagnose, and manage hydrocephalus using the frameworks from this module. Work through each question systematically before consulting the answers.
Scenario 1: A 6-week-old infant has a head circumference tracking on the 50th centile since birth but over 4 weeks has crossed to above the 98th centile. OFC today = 42 cm (>2 SD above mean). Anterior fontanelle tense. Sunset sign present. Cranial USG shows dilated lateral and third ventricles; the fourth ventricle is normal in size.
Q1: What type of hydrocephalus is this (communicating or obstructive)? What is the most likely level of obstruction?
Q2: What is the name of the specific sign observed in the eyes, and what is its mechanism?
Q3: What is the first surgical option, and when would ETV be preferred over VP shunt?
Answers:
1. Obstructive hydrocephalus — lateral and third ventricles dilated but fourth ventricle normal indicates obstruction at the level of the cerebral aqueduct (aqueductal stenosis).
2. Sunset sign (Parinaud's sign variant) — tonic downward deviation of both eyes from pressure on the midbrain pretectal area impairing upgaze centres.
3. VP shunt is the first-line treatment in a 6-week-old infant (ETV success rates are lower in infants <6 months). ETV is preferred over VP shunt in children >6 months with aqueductal stenosis because it avoids the lifelong shunt dependence and complications.
Scenario 2: A 7-year-old boy with known hydrocephalus and VP shunt (inserted 2 years ago) presents with morning headache and vomiting for 5 days. Temperature 37.2°C, neurologically intact. CT shows ventricles larger than the post-shunt baseline scan.
Q4: What is the most likely complication, and how is it confirmed and managed?
SELF-CHECK
A CT brain in a 4-year-old shows large ventricles with widened cerebral sulci. Head circumference is on the 50th centile. The child has cerebral atrophy from hypoxic-ischaemic encephalopathy. What is the correct diagnosis and management?
A. Communicating hydrocephalus — start acetazolamide
B. Obstructive hydrocephalus — refer for VP shunt
C. Hydrocephalus ex vacuo — treat the underlying cause; no shunting required
D. Post-meningitis hydrocephalus — serial LP and VP shunt if fails
Reveal Answer
Answer: C. Hydrocephalus ex vacuo — treat the underlying cause; no shunting required
Hydrocephalus ex vacuo is apparent ventricular enlargement caused by loss of brain parenchyma (atrophy), not by CSF overproduction or obstruction. The key distinguishing features are: widened cerebral sulci (brain shrinkage, not just ventricular expansion) and NO raised ICP (normal OFC, no symptoms of raised ICP, no bulging fontanelle). There is NO excess CSF to drain; shunting is not indicated and could cause over-drainage. Management is of the underlying cause (in this case, the sequelae of HIE). This is a commonly tested distinction.