Page 13 of 48
PE27.4 | Hydrocephalus — SDL Guide
Learning Objectives
- Identify the clinical features of hydrocephalus in infants and older children, including the sunset sign
- Classify hydrocephalus as communicating or obstructive and explain the pathophysiological basis of each
- List the major causes of hydrocephalus in the paediatric age group
- Interpret OFC measurement, head CT/MRI findings, and cranial ultrasound in the diagnosis of hydrocephalus
- Outline the management options including VP shunt and endoscopic third ventriculostomy, and their complications
INSTRUCTIONS
Hydrocephalus — literally 'water on the brain' — is an abnormal accumulation of CSF within the ventricular system, leading to raised intracranial pressure and, if untreated, progressive brain damage. In India, it remains one of the most common paediatric neurosurgical conditions, occurring as a complication of meningitis, prematurity with intraventricular haemorrhage, congenital malformations, and neural tube defects. The clinical picture in infants is distinct from older children because of the open fontanelle and unfused sutures — knowing these age-specific presentations allows you to recognise hydrocephalus before irreversible neurological damage occurs.
References
- Ghai Essential Pediatrics, 9th ed., Ch 18 (Neurological Conditions) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 610 (Hydrocephalus) (textbook)
- IAP Guidelines on Paediatric Neurosurgical Conditions (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-month-old infant is brought to the paediatric OPD because the mother noticed his head has been growing very fast over the past 6 weeks. On examination: head circumference 44 cm (>97th centile for age), bulging anterior fontanelle, prominent scalp veins, and when you shine a light in his eyes, he shows tonic downward deviation of both eyes with the sclerae visible above the iris. The infant was delivered at 30 weeks' gestational age and had a documented grade III intraventricular haemorrhage (IVH) in the NICU. What type of hydrocephalus does this infant most likely have, and what is the most likely cause?
WHY THIS MATTERS
Hydrocephalus is not a rare or specialised condition limited to neurosurgical units — it is a common outcome of several paediatric conditions you will encounter across all levels of care: meningitis (bacterial and tuberculous), prematurity with intraventricular haemorrhage, congenital neural tube defects, and central nervous system tumours. As an intern, you will be the first to measure the head circumference of a child brought for a developmental check or a febrile illness — a rapidly enlarging head circumference in an infant is an emergency requiring urgent CT and neurosurgical referral. Missing hydrocephalus on a routine developmental check because the head circumference was not plotted on a centile chart is a preventable diagnostic failure. Understanding the pathophysiology tells you which children are at risk, what to look for, and when to act.
RECALL
Before proceeding, recall the following:
• CSF physiology (from PY): CSF produced by the choroid plexus at approximately 0.35 mL/min (~500 mL/day); total CSF volume is ~150 mL; circulates from lateral ventricles → third ventricle → cerebral aqueduct (of Sylvius) → fourth ventricle → subarachnoid space → absorbed at arachnoid granulations (Pacchioni's granulations).
• Anterior fontanelle (from AN): diamond-shaped, closes by 12–18 months; NORMALLY slightly depressed or level; bulging = raised ICP; sunken = dehydration.
• Cranial sutures (from AN): in infants, sutures allow the skull to expand under raised ICP — this is why infants can tolerate gradually rising ICP for longer than older children whose sutures are fused.
• Meningitis complications (from PE27.1/27.2): communicating hydrocephalus is a recognised complication of both bacterial meningitis and TBM — from arachnoid fibrosis impairing CSF resorption.
Clinical Presentation of Hydrocephalus
The clinical presentation of hydrocephalus is dramatically age-dependent, and understanding this age-dependence is the key to not missing the diagnosis in clinical practice. The fundamental variable is the degree of fontanelle and cranial suture patency — a property that changes continuously through the first two years of life. In young infants, the fontanelle is open and the cranial sutures are unfused, so the expanding skull can accommodate slowly rising CSF pressure by growing outward. The result is that raised ICP in infants is signalled primarily by an enlarging head circumference and bulging fontanelle rather than by the headache and vomiting that dominate the picture in older children. In older children beyond 18–24 months, the sutures are fused and the skull is rigid; raised ICP cannot be absorbed by calvarial expansion and instead produces the classic acute-onset raised-ICP syndrome of headache, vomiting, and papilloedema. This age-based difference in skull compliance means that the same degree of ventricular dilation will produce very different clinical pictures depending on the child's age — a principle that fundamentally organises your approach to examination and interpretation.
In infants (fontanelle open, sutures unfused):
• Macrocephaly: The most consistent and measurable sign. Occipito-frontal circumference (OFC) exceeds the 98th centile (>2 SD above the mean) for age and sex, OR is crossing centile lines on serial measurements at an abnormal velocity. A single above-normal measurement may reflect familial macrocephaly; an accelerating OFC that crosses two or more centile lines is a red flag requiring investigation.
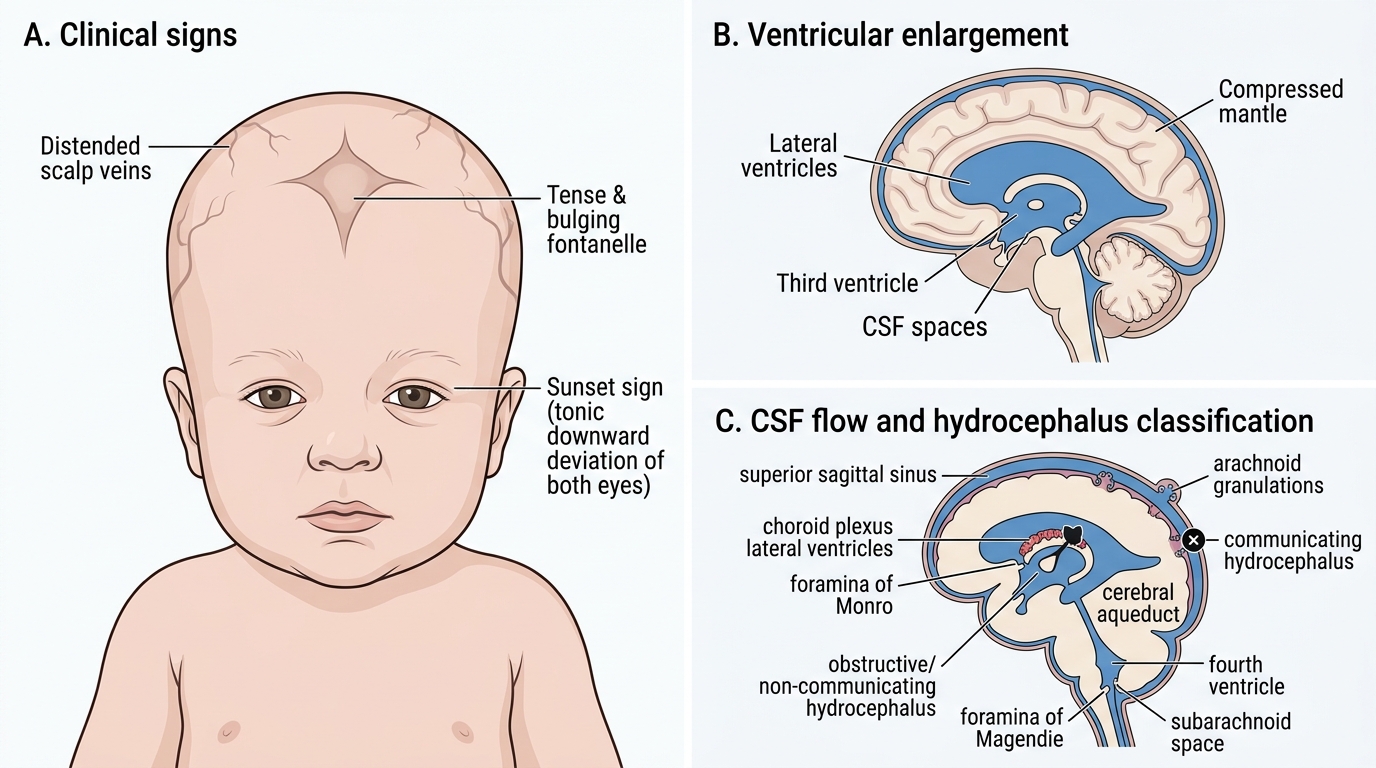
• Bulging anterior fontanelle: Tense or bulging even when the infant is upright and not crying — indicates raised ICP transmitted through the patent fontanelle.
• Dilated scalp veins: CSF pressure impairs venous drainage from the scalp, distending the visible scalp veins in a characteristic fan-like pattern.
• Sunset sign (Parinaud's sign variant): Tonic downward deviation of both eyes, with the sclerae visible above the iris — the classic 'setting sun' appearance. Caused by pressure on the midbrain pretectal area (Edinger-Westphal nucleus-region) impairing upgaze. This is a specific and important sign of raised ICP in infants. Note: it is NOT a physiological sign in healthy infants beyond the neonatal period.
• Prominent forehead (frontal bossing): Result of the disproportionate anterior expansion of the calvarium.
• Craniotabes: Eggshell-like cracking of the thinned skull on pressure over the parieto-occipital region (Macewen's sign).
• Developmental delay (motor milestones first, as periventricular motor tracts are compressed), poor feeding, irritability.
In older children (sutures fused):
The skull cannot expand, so raised ICP manifests acutely:
• Headache: Typically worst in the morning (recumbent position increases ICP at night), improved by sitting up. Morning vomiting without nausea (projectile) is characteristic.
• Papilloedema on fundoscopy: venous pulsations absent, blurred disc margin, disc elevation — indicates chronic raised ICP; rarely present in acute hydrocephalus.
• Cushing's triad: Bradycardia, systolic hypertension, and irregular respirations — indicates imminent herniation; a late and ominous sign.
• Sixth nerve palsy (CN VI) — a false localising sign from raised ICP stretching the nerve over the petrous bone.
Infant Hydrocephalus: Clinical Signs and CSF Pathophysiology
Pathophysiology and Classification of Hydrocephalus
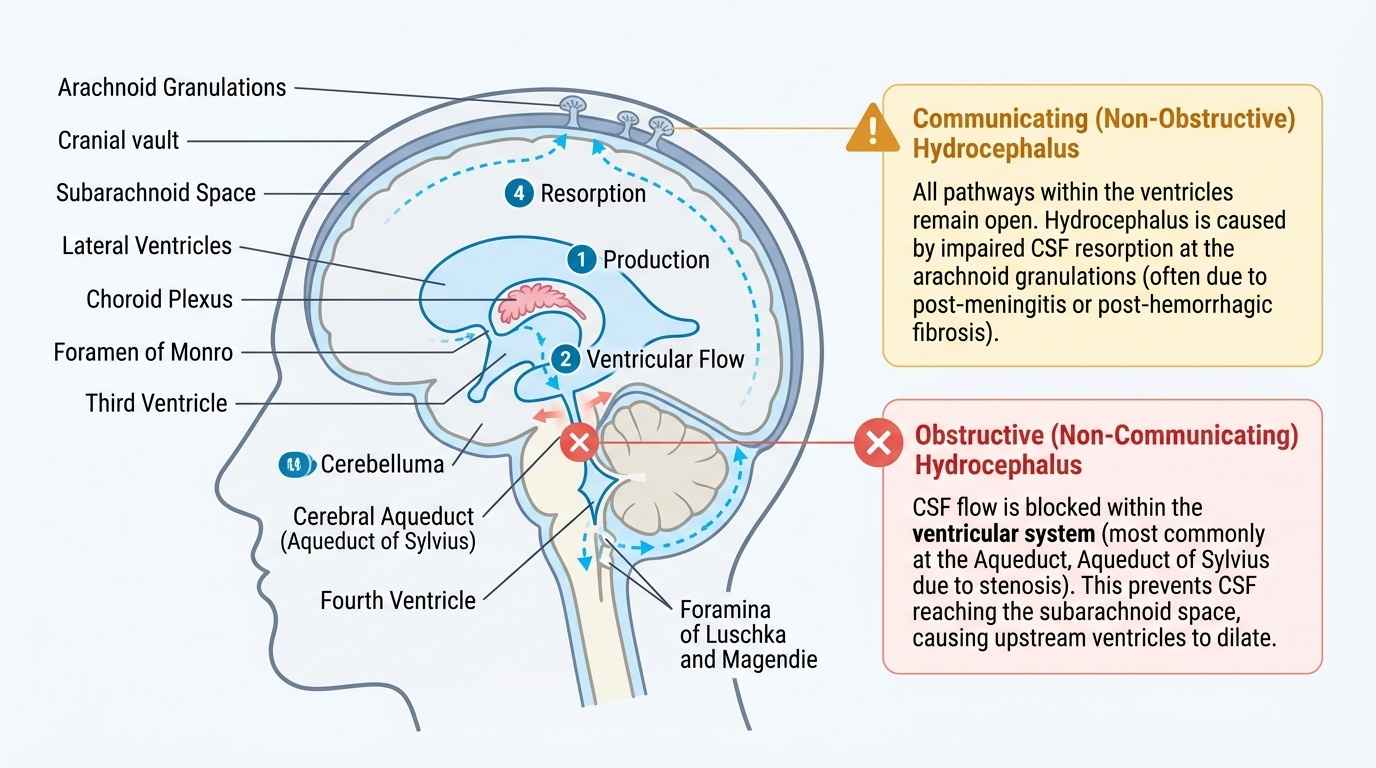
The normal CSF cycle is a continuous loop: production at the choroid plexus (primarily in the lateral ventricles) → flow through the foramina of Monro into the third ventricle → through the cerebral aqueduct (aqueduct of Sylvius) into the fourth ventricle → out through the foramina of Magendie and Luschka into the subarachnoid space → absorption at the arachnoid granulations along the sagittal sinus. Hydrocephalus results whenever this loop is disrupted: either by obstruction of CSF flow within the ventricular system, or by failure of CSF resorption at the arachnoid granulations, or rarely by excess CSF production (choroid plexus papilloma).
Provided image
The clinical classification that matters most for management is the distinction between communicating (non-obstructive) and obstructive (non-communicating) hydrocephalus, because it determines the surgical approach.
Communicating hydrocephalus:
All CSF pathways remain open (communication between ventricles and subarachnoid space is intact), but resorption at the arachnoid granulations is impaired. The commonest paediatric cause is post-meningitis fibrosis — both bacterial and tuberculous meningitis cause a fibrotic reaction in the basal cisterns and over the arachnoid granulations, permanently impairing their resorptive capacity. Other causes include post-haemorrhagic (post-IVH in premature infants), subarachnoid haemorrhage, and choroid plexus papilloma (excess production).
Obstructive (non-communicating) hydrocephalus:
CSF flow is blocked at some point within the ventricular system, before reaching the subarachnoid space. The blocked segment determines which ventricles dilate:
• Aqueductal stenosis — most common cause of congenital obstructive hydrocephalus; narrowing or obstruction of the aqueduct of Sylvius → dilation of lateral and third ventricles but normal fourth ventricle; may be isolated or associated with X-linked inheritance (L1CAM gene mutation)
• Dandy-Walker malformation — cystic dilation of the fourth ventricle with hypoplasia of the cerebellar vermis; all four ventricles can dilate
• Posterior fossa tumour or cyst — compresses the fourth ventricle or aqueduct
• Intraventricular haemorrhage (preterm neonates) — blood clot obstructs the aqueduct or foramina
• Neural tube defects (meningomyelocele with Arnold-Chiari II malformation) — hindbrain herniation into the cervical canal obstructs CSF outflow
Hydrocephalus ex vacuo (IMPORTANT misnomer):
Ventricular enlargement caused by loss of brain parenchyma (atrophy) — NOT true hydrocephalus. There is no raised ICP. Seen in severe cerebral atrophy (hypoxic-ischaemic encephalopathy, advanced metabolic disease). CT shows large ventricles and widened sulci. Management: treat the underlying cause; NO shunting required.
SELF-CHECK
A 3-month-old premature infant had a grade III intraventricular haemorrhage at birth. Now presents with progressive macrocephaly. CSF analysis shows blood-stained fluid from all LP tubes equally. CT shows all four ventricles dilated, communicating with the subarachnoid space. What is the mechanism of hydrocephalus?
A. Obstructive hydrocephalus from blood clot in the aqueduct
B. Communicating hydrocephalus from fibrosis at arachnoid granulations
C. Hydrocephalus ex vacuo from periventricular white matter loss
D. Choroid plexus papilloma causing excess CSF production
Reveal Answer
Answer: B. Communicating hydrocephalus from fibrosis at arachnoid granulations
Post-haemorrhagic hydrocephalus in premature infants typically causes communicating hydrocephalus — blood breakdown products cause fibrosis and scarring of the arachnoid granulations, impairing CSF resorption. All CSF pathways remain open (all four ventricles dilate, CSF communicates with the subarachnoid space). If the blood clot directly obstructs the aqueduct it would be obstructive, but the CT description showing all four ventricles dilated with subarachnoid communication points to communicating type. Hydrocephalus ex vacuo has NO raised ICP.
Diagnosis and Investigation
The diagnosis of hydrocephalus begins with a simple clinical measurement — the occipito-frontal circumference (OFC) — and is confirmed by neuroimaging. In infants, this is a primarily clinical-radiological diagnosis; in older children, the presentation with raised ICP symptoms makes neuroimaging urgent.
Occipito-frontal circumference (OFC) measurement:
Measure with a non-stretchable tape around the largest circumference of the head (over the most prominent part of the occiput and the most prominent part of the forehead). Plot on a gender-specific WHO/IAP growth chart. A single measurement above the 98th centile (>2 SD) requires plotting to assess trajectory; serial measurements crossing 2+ centile lines upward within weeks are abnormal and indicate rapidly progressive hydrocephalus. Familial macrocephaly (measure parental OFC — typically large in both parents) must be distinguished from pathological expansion.
Cranial ultrasonography (neonates and infants):
Through the open anterior fontanelle, cranial USG provides a radiation-free, bedside assessment of ventricular size and architecture. Measurements: the ventricular index (Levene's chart) and the anterior horn width are compared against gestational-age-specific norms. USG is the first-line investigation for suspected hydrocephalus in neonates and infants due to its safety and availability in NICUs and peripheral hospitals. It allows serial monitoring without radiation exposure.
CT brain (with contrast for suspected mass lesion):
CT provides rapid cross-sectional imaging of ventricular size, identifies the likely site of obstruction (aqueduct stenosis vs fourth ventricular outlet), and detects associated pathology (posterior fossa tumour, haemorrhage, tuberculomata). Ventriculomegaly — dilatation of the ventricular system on CT — is graded by the ratio of the frontal horn width to the internal skull diameter (FHW/ISD > 0.33 is abnormal). Periventricular lucency (transependymal CSF seepage) on CT indicates active raised ICP.
MRI brain:
MRI provides superior soft-tissue detail: aqueduct flow studies (phase-contrast MRI demonstrates CSF flow through the aqueduct — absent in aqueductal stenosis), posterior fossa anatomy (Dandy-Walker, Chiari malformations), and detection of white matter changes. MRI is the preferred imaging modality for planning surgical intervention, particularly endoscopic third ventriculostomy.