Page 25 of 48
PE27.8 | Status Epilepticus — SDL Guide
Learning Objectives
- Define status epilepticus using the ILAE 2015 operational thresholds (T1 and T2)
- Identify the causes of status epilepticus in children
- Apply the phased emergency management protocol with correct weight-based drug doses
- Recognise refractory status epilepticus and escalate to ICU management
INSTRUCTIONS
Status epilepticus is the most common paediatric neurological emergency and carries significant morbidity and mortality if not treated promptly with a phased, time-based protocol. Time is brain — every minute of continuous seizure activity increases the risk of neuronal injury and makes the seizure progressively harder to abort. This module will teach you the precise treatment sequence — from the first five minutes to refractory status — so you can act decisively without hesitation when confronted with a convulsing child.
References
- Ghai Essential Pediatrics, 9th ed., Ch 18 (Neurology — Status Epilepticus) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 610 (Status Epilepticus) (textbook)
- ILAE 2015 Definition of Status Epilepticus (Trinka et al., Epilepsia) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 3-year-old boy is brought to the emergency department by ambulance, actively convulsing. His parents say the seizure started at home 12 minutes ago. He is stiff with rhythmic jerking of all four limbs, eyes deviated upward, oxygen saturation 91% on room air. He had a temperature of 40°C before the seizure. The ambulance crew placed him in recovery position but could not establish IV access. There is no intravenous access. You look at the clock. The seizure is now at 14 minutes. You know that status epilepticus is defined as a seizure lasting ≥5 minutes — and that the window for first-line treatment has already passed. Your systematic, time-based response in the next 10–15 minutes will determine whether this child emerges with minimal neurological damage or with permanent injury.
WHY THIS MATTERS
Status epilepticus is the most common paediatric neurological emergency, accounting for 3–8% of all paediatric emergency admissions. It has a case fatality rate of approximately 3–5% in children and significant neurological sequelae in a further 10–30%, depending on aetiology and duration. As a final-year medical student and future doctor — whether you work in a primary health centre, a district hospital, or a paediatric emergency unit — you will encounter this emergency. The phased management protocol is a required competency, and knowing the weight-based doses of lorazepam, diazepam, and second-line AEDs from memory is as essential as knowing how to manage airway and breathing. Delay in treatment is the single most modifiable determinant of outcome.
RECALL
Before proceeding, recall from the Epilepsy SDL (PE27.7): seizures normally self-terminate because inhibitory mechanisms (GABAergic interneurons, adenosine release, potassium channel opening) become activated after a brief discharge and suppress further firing. Recall from Febrile Seizures (PE27.6): a prolonged febrile seizure (≥15–30 minutes) IS febrile status epilepticus. Recall from Basic Pharmacology (PY/PH): benzodiazepines potentiate GABA-A receptor-mediated chloride influx, hyperpolarising neurons; their efficacy in status epilepticus is highest early when GABA-A receptors are still functional, and decreases with seizure duration as receptors internalise.
Clinical Presentation and Definition of Status Epilepticus
Status epilepticus (SE) is defined by the International League Against Epilepsy (ILAE 2015) using two operational time thresholds that reflect distinct biological states:
T1 (operational threshold to treat: ≥5 minutes): At 5 minutes, a generalised convulsive seizure is unlikely to self-terminate and benzodiazepine must be administered. The classic arbitrary '30-minute' definition is outdated and dangerous — waiting 30 minutes before treating means 25 minutes of preventable neuronal injury. The ILAE T1 threshold of 5 minutes is the clinical action point.
T2 (threshold for long-term consequences: ≥30 minutes): At 30 minutes of continuous seizure activity, irreversible neuronal injury begins — hippocampal neuron loss, excitotoxicity, cerebral oedema, and systemic complications (hyperthermia, hypoglycaemia, lactic acidosis, rhabdomyolysis) compound the injury. Prevention of reaching T2 is the primary goal of treatment.
Types of status epilepticus:
Convulsive SE (CSE): The most common and clinically obvious type. Presents as continuous or rapidly recurrent generalised tonic-clonic activity. A child in convulsive SE is: (1) actively convulsing with tonic-clonic movements; (2) unconscious; (3) may be cyanotic during the tonic phase; (4) unable to protect the airway; (5) hypoxaemic.
Non-convulsive SE (NCSE): SE without prominent motor manifestations — presents as: prolonged absence (absence SE — staring, fluctuating consciousness, rare automatisms); or subtle SE (minimal motor movements in a post-convulsive or encephalopathic patient). NCSE must be suspected in any child who remains encephalopathic or confused after a convulsive seizure — only EEG can diagnose it. Subtle SE is a particular danger: the motor activity stops, the physicians assume the seizure has ended, but electrographic seizure activity continues causing ongoing neuronal injury.
Febrile SE: Prolonged febrile seizure ≥15–30 minutes meeting the SE definition; clinically managed identically to other convulsive SE.
Recognition at the bedside:
A child in convulsive SE is unmistakable — continuous tonic-clonic jerking for >5 minutes, unconscious, with airway at risk. The critical additional recognition challenge is:
1. Timing — ask witnesses precisely when the seizure started; if no witness, note time of presentation and assume seizure has been ongoing
2. Identify any prior seizure activity and inter-ictal recovery — if there is none, it is SE
3. After initial treatment, if the child does not regain consciousness within 30–60 minutes of cessation of motor activity, suspect NCSE and request urgent EEG
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
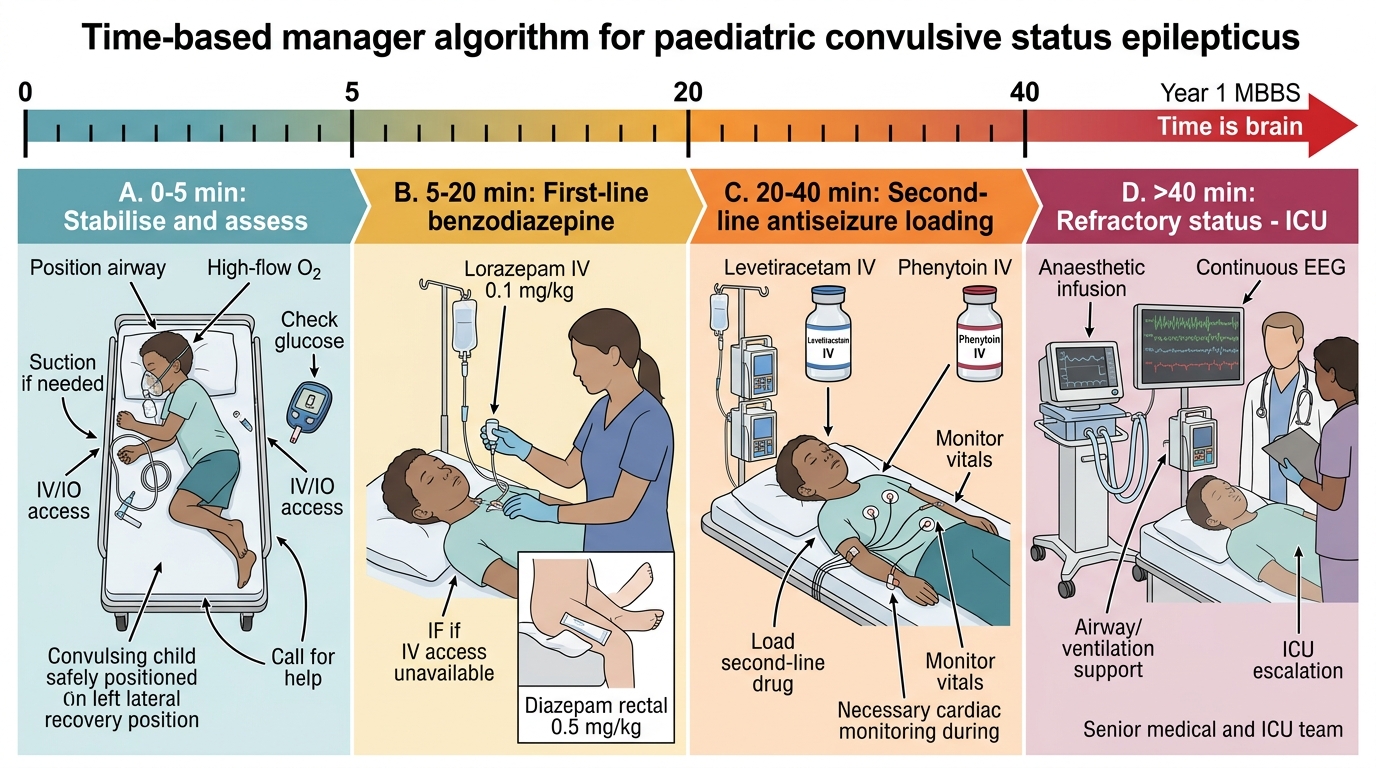
Time-Based Management of Paediatric Status Epilepticus
Pathophysiology and Aetiology
Understanding WHY status epilepticus perpetuates — why it does not self-terminate like most seizures — is essential for understanding why benzodiazepines are the first-line and why their efficacy decreases with seizure duration. Two complementary mechanisms explain SE self-perpetuation:
Mechanism 1 — Failure of inhibitory termination:
Normally, a seizure self-terminates because GABA-A receptors on inhibitory interneurons amplify inhibition and quench the discharge. During prolonged SE, GABA-A receptors are internalised (removed from the synaptic membrane by clathrin-mediated endocytosis) within minutes of sustained seizure activity. The loss of surface GABA-A receptors means less chloride influx → less hyperpolarisation → less inhibition → seizure cannot stop. This is the molecular basis for why benzodiazepines, which act through GABA-A receptors, become progressively less effective as SE continues — they have fewer receptors to act on.
Mechanism 2 — Sustained excitatory drive:
Concurrently, NMDA receptors (the principal excitatory glutamate receptors) are inserted into the synapse during SE, amplifying excitation. The result is a vicious cycle: more excitation, less inhibition, sustained discharge, more receptor trafficking, even more SE-maintenance. This provides the rationale for NMDA-targeting rescue agents in refractory SE.
Systemic consequences of prolonged SE (why T2 matters):
As SE continues beyond 30 minutes, systemic consequences compound the neurological injury:
• Hypoxia and hypercapnia — impaired ventilation during convulsions → cerebral ischaemia
• Hyperthermia — muscle activity generates heat; core temperature may reach 40–41°C → exacerbates neuronal injury
• Hypoglycaemia — sustained seizure activity depletes cerebral glucose; treat empirically early
• Metabolic acidosis (lactic acid from intense muscle activity)
• Rhabdomyolysis → myoglobinuria → acute kidney injury in prolonged SE
• Autonomic instability — hypertension, tachycardia, then hypotension in late SE
Causes of status epilepticus in children by age and context:
• Febrile illness — the most common cause in young children (febrile SE); HHV-6, influenza, bacterial infections
• Known epilepsy — missed AED doses, AED toxicity, fever as SE precipitant in Dravet syndrome
• Acute CNS insult — meningitis, encephalitis (HSV encephalitis — highly epileptogenic), traumatic brain injury
• Metabolic/electrolyte disturbance — hypoglycaemia (always check!), hyponatraemia, hypocalcaemia, hypomagnesaemia
• Toxins/drugs — accidental ingestion (tricyclic antidepressants, theophylline, organophosphates, isoniazid), drug withdrawal
• Structural — acute cortical stroke, intracranial haemorrhage, cortical venous thrombosis
• Unknown / cryptogenic — no cause identified despite workup (common in children, especially first-time SE)
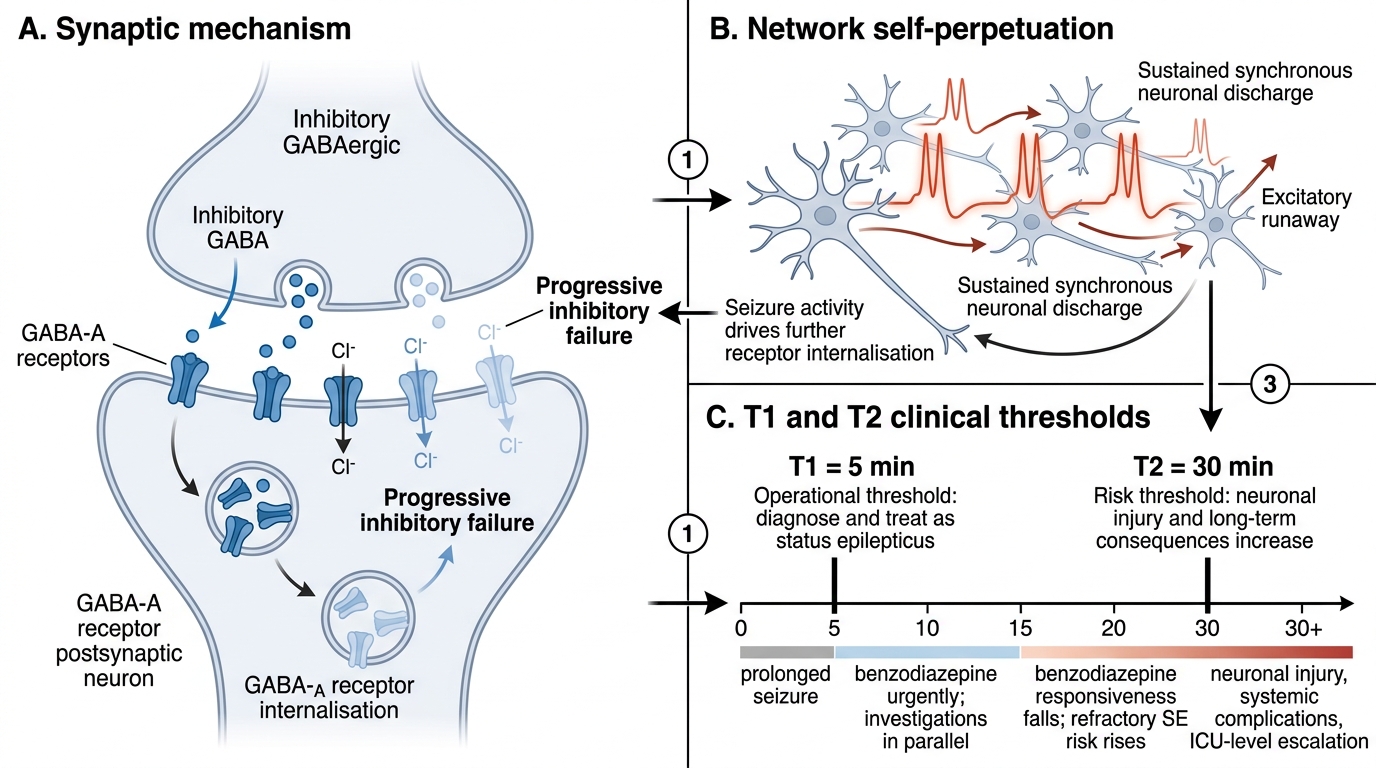
Self-Perpetuation of Convulsive Status Epilepticus
Diagnosis and Initial Assessment
The diagnosis of convulsive status epilepticus is clinical and bedside — a child with continuous tonic-clonic activity lasting more than 5 minutes has SE until proven otherwise. The critical principle is that investigations must run in parallel with treatment, not before it. Delaying the first benzodiazepine dose while waiting for a blood glucose result is a medical error; the glucose should be measured by bedside glucometer while the benzodiazepine is being drawn up, and IV access established during the assessment phase. The initial bedside assessment follows the ABCDE structure and takes no more than 2–3 minutes before first drug dose:
A — Airway: Is the airway clear? Clear secretions, position the child on their side; jaw thrust if needed. Avoid forcible airway insertion during active convulsion (bite risk, injury).
B — Breathing: Respiratory rate, work of breathing, oxygen saturation. Provide 100% O₂ via non-rebreather mask. Bag-valve-mask (BVM) if not breathing adequately.
C — Circulation: Heart rate, BP, skin perfusion. Establish IV access if not already present. If IV access cannot be established in 2 attempts, use intraosseous (IO) access immediately — IO delivers all resuscitation drugs including AEDs as rapidly as IV.
D — Disability: AVPU, pupil size and reaction. Look for evidence of focal neurological deficit (suggests structural cause or focal SE). Note the time.
E — Exposure: Temperature (to identify febrile SE), check for signs of trauma (non-accidental injury), rash (meningococcal disease, HSV), pharmacological ingestion (pill bottles, unusual odour).
Bedside glucose — FIRST investigation: A bedside glucometer test takes 30 seconds. Hypoglycaemia (glucose <2.5 mmol/L or <45 mg/dL in a seizing child) is rapidly fatal and easily treatable. Give dextrose 2–4 mL/kg of 10% dextrose IV empirically in any infant/young child with SE while awaiting confirmatory glucose.
Parallel investigations (to be sent but NOT to delay treatment):
• Blood glucose, sodium, calcium, magnesium (electrolyte disturbances)
• Full blood count, CRP (infection screen)
• Blood cultures before antibiotics if bacterial meningitis/encephalitis suspected
• AED drug levels if child is on AEDs (measure compliance)
• Toxicology screen (blood and urine) if drug ingestion suspected
• LP (only AFTER seizure control + haemodynamic stability + brain imaging if focal features are present — never during active convulsion)
• EEG — urgent if child remains encephalopathic after convulsions stop (to detect NCSE)
SELF-CHECK
A 4-year-old (weight 16 kg) arrives with continuous generalised tonic-clonic seizure for 8 minutes. IV access is secured. The bedside glucose is normal. What is the FIRST drug treatment and the CORRECT dose?
A. Rectal diazepam 8 mg (0.5 mg/kg)
B. Intravenous lorazepam 1.6 mg (0.1 mg/kg)
C. Intravenous phenytoin 300 mg (18 mg/kg)
D. Buccal midazolam 3 mg (0.2 mg/kg)
Reveal Answer
Answer: B. Intravenous lorazepam 1.6 mg (0.1 mg/kg)
IV access is available, so the first-line drug is intravenous lorazepam at 0.1 mg/kg = 1.6 mg (weight 16 kg). Lorazepam IV has a rapid onset (~2 min), prolonged antiseizure duration (12–24 h), and is the hospital first-line benzodiazepine for established SE. Rectal diazepam 0.5 mg/kg and buccal midazolam 0.2 mg/kg are pre-hospital/no-IV-access alternatives — when IV access is available, IV lorazepam is preferred. Phenytoin is a second-line drug given only after benzodiazepine failure — never as first-line.
CLINICAL PEARL
Two critical rules for status epilepticus management: (1) Benzodiazepines work best early — every minute of SE that passes before the first benzodiazepine dose reduces its efficacy, because GABA-A receptors are progressively internalised. The T1 = 5 minutes threshold is the trigger to act, not to wait and see. (2) Phenytoin MUST NOT be given intramuscularly — it crystallises in muscle and is not absorbed. Phenytoin IV must be given slowly (≤1 mg/kg/min with cardiac monitoring) to avoid arrhythmia and hypotension. Fosphenytoin (water-soluble prodrug) is safer and can be given IM. In many modern paediatric units, levetiracetam IV has largely replaced phenytoin as second-line SE treatment due to its favourable safety profile and ease of administration.