Page 26 of 48
PE27.8 | Status Epilepticus — SDL Guide (Part 2)
Emergency Management
The management of status epilepticus follows a structured, time-based protocol. Every clinician must be able to execute this protocol from memory, because SE management is a medical emergency where hesitation costs neurons. The protocol is divided into four phases based on time from onset — each phase has a clear therapeutic goal, specific drug choices, and a defined escalation trigger. Understanding the rationale for this phased approach is as important as knowing the drug names and doses: the first phase focuses on stabilising the child's physiology (airway, oxygen, glucose) while simultaneously obtaining access; the second phase uses benzodiazepines, which are most effective when given early before GABA-A receptors internalise; the third phase uses IV AEDs when benzodiazepines have failed; and the fourth phase uses anaesthetic agents in the ICU. Moving through phases without unnecessary delay, and not repeating a class of drug that has already failed, are the two discipline rules of SE management.
Provided image
Phase 1 — Pre-treatment / Stabilisation (0–5 minutes):
Goal: Protect the child and prepare for drug therapy; treat hypoglycaemia if present.
• Recovery position (lateral decubitus); protect airway
• 100% oxygen via non-rebreather mask
• Establish IV access (or IO if IV fails after 2 attempts)
• Bedside glucose — give dextrose 2–4 mL/kg of 10% dextrose IV if hypoglycaemic
• Start monitoring: SpO₂, ECG, temperature
• Identify the child's weight (for weight-based dosing) — ask parents; if unknown, estimate by age (weight in kg ≈ 2 × age + 8, or use a Broselow tape)
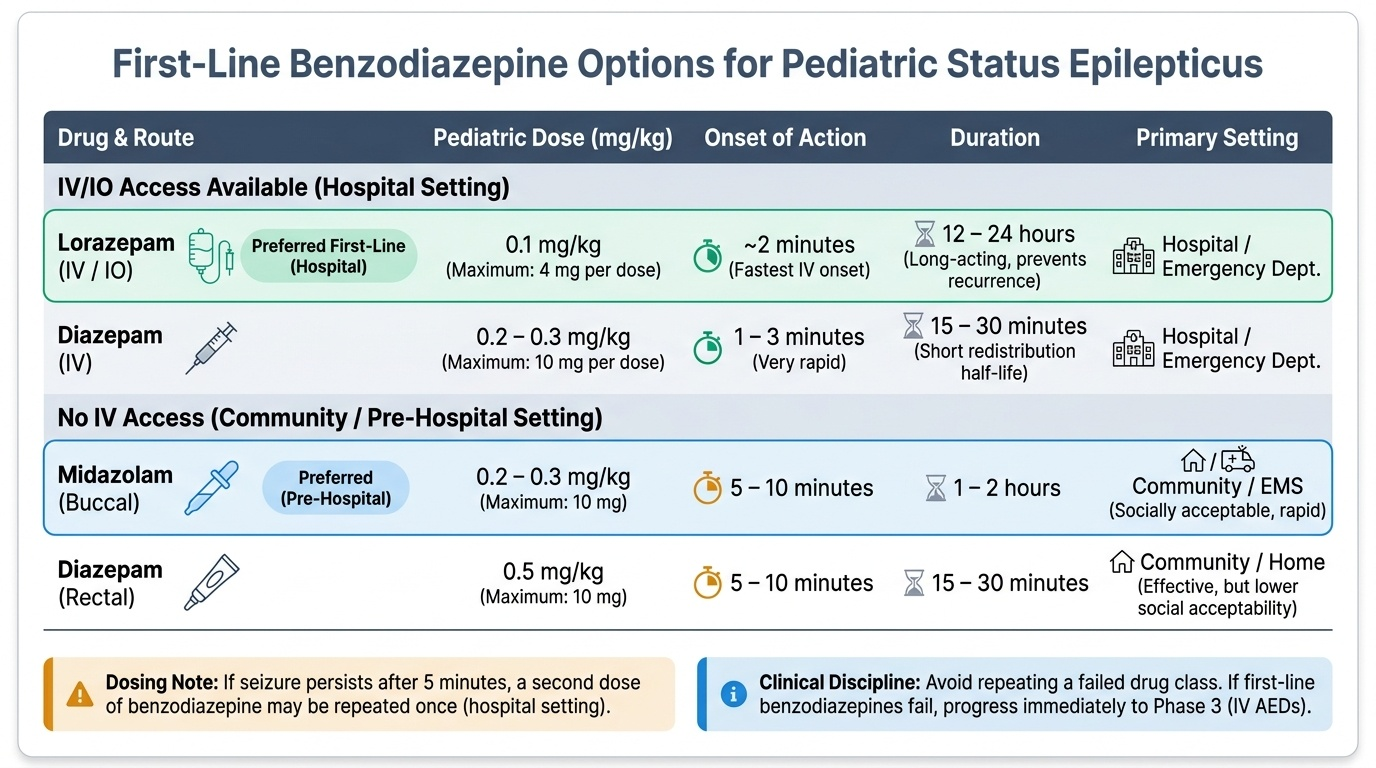
Phase 2 — First-line benzodiazepine (5–20 minutes from seizure onset):
Goal: Terminate the seizure with the fastest available benzodiazepine route.
IV/IO access AVAILABLE:
• Lorazepam IV/IO: 0.1 mg/kg (maximum 4 mg per dose); onset ~2 min; duration 12–24 h. Preferred first-line.
• Can repeat once after 5 minutes if seizure persists.
No IV access (community/pre-hospital):
• Buccal midazolam: 0.2–0.3 mg/kg (maximum 10 mg); apply to buccal mucosa; onset 5–10 min; increasingly preferred over rectal diazepam due to ease and social acceptability
• Rectal diazepam: 0.5 mg/kg (maximum 10 mg); onset 5–10 min; effective but less convenient
• Intranasal midazolam: 0.2 mg/kg — used in some settings; absorption variable
Phase 3 — Second-line AED (20–40 minutes from onset, if benzodiazepine has failed):
Goal: Terminate SE after benzodiazepine failure with an IV AED.
Option A — Levetiracetam IV: 20–60 mg/kg (max 3000 mg) over 10–15 minutes
• Rapidly becoming the preferred second-line agent in many paediatric centres
• Advantages: no cardiac monitoring required, no respiratory depression, minimal drug interactions
• Supported by ECLIPSE trial (equivalent to phenytoin and valproate for second-line SE in children)
Option B — Phenytoin IV: 15–20 mg/kg at ≤1 mg/kg/min (do NOT exceed this rate)
• Must be diluted in normal saline (not dextrose — precipitates); must NOT be given IM
• Monitor ECG and BP during infusion (arrhythmia and hypotension risk)
• Fosphenytoin IV/IM: 15–20 mg phenytoin equivalents (PE)/kg — water-soluble prodrug; can be given IM; safer cardiac profile; preferred over phenytoin in most guidelines
Option C — Sodium valproate IV: 20–40 mg/kg over 10 minutes
• Broad-spectrum; good for generalised SE
• Avoid in liver disease, mitochondrial disorders, or if hepatic metabolic cause suspected
Only ONE second-line agent should be given; if it fails → proceed to Phase 4.
Phase 4 — Refractory SE (>40 minutes from onset, failed benzodiazepine + second-line AED):
Goal: ICU management with anaesthetic agents to achieve burst-suppression on EEG.
Refractory SE = SE that has not responded to an adequate benzodiazepine and one second-line AED. This requires:
• Intubation and mechanical ventilation (to protect airway from anaesthetic agents)
• Continuous EEG monitoring to guide therapy and detect burst-suppression
• Midazolam infusion (0.1–0.4 mg/kg/h) — first-line anaesthetic agent for refractory SE in many guidelines
• Thiopentone (sodium thiopental) infusion (loading 2–4 mg/kg, then 2–8 mg/kg/h) — barbiturate, potent GABA-A agonist; most evidence for refractory SE
• Propofol infusion — NOT recommended in children <15 years (propofol infusion syndrome risk — fatal metabolic acidosis with prolonged high-dose use)
• Identify and treat the underlying cause — antivirals for HSV (aciclovir), antibiotics for meningitis, pyridoxine for pyridoxine-dependent epilepsy, calcium/glucose correction
SELF-CHECK
A 5-year-old (weight 18 kg) with known epilepsy presents to the emergency department in active convulsive SE for 25 minutes. IV lorazepam was given at 15 minutes (dose: 0.1 mg/kg = 1.8 mg) but the seizure continues. Glucose is normal. Which of the following is the MOST APPROPRIATE next step?
A. Repeat IV lorazepam 0.1 mg/kg (1.8 mg)
B. Levetiracetam IV 20 mg/kg (360 mg) over 10 minutes
C. Phenobarbitone IM 15 mg/kg
D. Oral valproate via nasogastric tube
Reveal Answer
Answer: B. Levetiracetam IV 20 mg/kg (360 mg) over 10 minutes
The seizure has not responded to a benzodiazepine (lorazepam 25 minutes ago, no response) — this now meets the criterion for Phase 3 (second-line IV AED). Levetiracetam IV 20–60 mg/kg over 10–15 minutes is the appropriate second-line choice. Another benzodiazepine dose is not indicated at this stage (the Phase 2 window has passed, the seizure is 25 minutes long, and benzodiazepine GABA-A receptor internalisation makes it less likely to work). Phenobarbitone IM has slower absorption; it is not first-choice second-line in most current guidelines. Oral valproate via NG tube has inadequate/unpredictable absorption in a seizing child and is inappropriate in an emergency.
Self-Assessment
Test your management knowledge with these case-based questions:
Case: A 2-year-old girl (weight 12 kg) is brought to the emergency department by her parents. She started convulsing at home 18 minutes ago. The tonic-clonic movements are ongoing. No IV access has been established. Bedside glucose is 3.8 mmol/L (normal). Temperature is 39.8°C.
Q1. No IV access is available. What is the IMMEDIATE drug treatment and dose?
Answer: Buccal midazolam 0.2–0.3 mg/kg = 2.4–3.6 mg (maximum 10 mg) applied to the buccal mucosa, OR rectal diazepam 0.5 mg/kg = 6 mg (maximum 10 mg). Simultaneously, continue attempts to establish IV access (or IO access after 2 failed IV attempts). These are equivalent first-line agents when no IV access is available.
Q2. IV access is established while giving buccal midazolam. The seizure continues for another 10 minutes despite the benzodiazepine (now at 28 minutes total). What is the next step and dose?
Answer: Second-line IV AED: Levetiracetam IV 20–60 mg/kg (= 240–720 mg for 12 kg child) over 10–15 minutes; OR fosphenytoin IV/IM 15–20 mg PE/kg (= 180–240 mg PE) given slowly with ECG monitoring; OR sodium valproate IV 20–40 mg/kg (= 240–480 mg) over 10 minutes.
Q3. The seizure continues for another 20 minutes despite second-line AED (now at 48 minutes). What has this become, and what is the management?
Answer: This is refractory status epilepticus (failed benzodiazepine + failed second-line AED, >40 minutes). Management: transfer to ICU; intubate and ventilate; continuous EEG monitoring; midazolam or thiopentone infusion (not propofol in children <15 years); urgent investigation for underlying cause (LP, viral PCR, autoimmune screen); neurology consult.
Key summary points:
• SE = ≥5 min seizure (T1 = treat) OR ≥2 seizures without recovery; T2 = 30 min (neurological consequences).
• Phase 1 (0–5 min): ABC + O₂ + glucose (dextrose 2–4 mL/kg of 10%).
• Phase 2 (5–20 min): Lorazepam IV 0.1 mg/kg (IV available) or buccal midazolam 0.2–0.3 mg/kg / rectal diazepam 0.5 mg/kg (no IV).
• Phase 3 (20–40 min, benzodiazepine failed): Levetiracetam IV 20–60 mg/kg or phenytoin/fosphenytoin IV or valproate IV.
• Phase 4 (>40 min, refractory): ICU — midazolam or thiopentone infusion; intubate.
• Phenytoin MUST NOT be given IM — crystallises. Give IV slowly (≤1 mg/kg/min with ECG).
• Propofol is CONTRAINDICATED in children <15 years for SE (propofol infusion syndrome).