Page 4 of 12
PE28.2-5 | Childhood Asthma — SDL Guide
Learning Objectives
- Explain the etio-pathogenesis of childhood asthma including Th2 immunopathogenesis, airway inflammation, and remodelling
- Describe the clinical types and presentations of asthma in children across different age groups
- Classify asthma severity (GINA grid) and control, and distinguish these from acute exacerbation severity
- Develop a stepwise treatment plan for childhood asthma appropriate to clinical presentation and severity (PE28.3)
- Enumerate the indications for pulmonary function testing (PFT) and interpret basic spirometric findings (PE28.4)
- Describe the principles and technique of nebulisation and age-appropriate inhaler device selection (PE28.5)
INSTRUCTIONS
Asthma is the most common chronic disease of childhood, affecting approximately 30 million children in India. It is characterised by variable airflow obstruction, bronchial hyperreactivity, and chronic airway inflammation — and it is both preventable and treatable. Despite effective therapies, asthma remains dramatically undertreated in India: most children receive only bronchodilator rescue therapy and never the inhaled corticosteroid controllers that prevent exacerbations and protect long-term lung function. As the doctor your patients will see, your understanding of severity classification, stepwise treatment, and crisis management will directly determine whether a child with asthma lives a normal, active life or suffers preventable disability.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 16 (Respiratory Disorders — Asthma) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 169 (Childhood Asthma) (textbook)
- GINA Report 2023 — Global Strategy for Asthma Management and Prevention (guideline)
- IAP Consensus Statement on Childhood Asthma Management 2020 (guideline)
- NAEPP Expert Panel Report 3 (EPR-3) — Guidelines for the Diagnosis and Management of Asthma (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Arjun, a 7-year-old boy from Mumbai, is brought to casualty at 11 PM by his terrified parents. For the past 4 hours he has had worsening difficulty breathing after playing cricket in a dusty field. He is sitting bolt upright, unable to speak more than 2–3 words between breaths, using his neck muscles to breathe, and his lips are faintly blue. His SpO₂ on room air reads 88%. His parents tell you that he has had 'chest problems' since age 3, wakes up coughing 2–3 nights a week, and has been using a 'blue inhaler' (salbutamol) almost every day for the past 6 weeks — but has never been prescribed a 'preventer'. His school nurse told the family last year that 'it's just allergies, he'll grow out of it.' You recognise the silent chest on auscultation as a medical emergency. As you call for the crash trolley and initiate oxygen, consider: How should this acute episode be classified and managed? And once Arjun is stabilised, what long-term plan would have prevented this admission?
WHY THIS MATTERS
Asthma is India's most prevalent chronic childhood disease, affecting an estimated 10–15% of school-age children — approximately 30 million children nationwide. Despite being largely controllable, asthma accounts for significant preventable mortality: over 1,000 children die from asthma annually in India, almost all from undertreated or inadequately managed disease. The economic burden — lost school days, caregiver income, emergency admissions — falls disproportionately on lower-income families who rely on salbutamol alone because 'the inhaler is expensive'. As a final-year student about to enter practice, you will encounter asthma in every clinical setting from the OP to the ICU. The skills in this module — severity classification, inhaled controller prescribing, exacerbation management, and nebulisation — are among the highest-value competencies you will carry into practice from paediatrics.
RECALL
Before proceeding, recall from your preclinical years:
- Bronchial smooth muscle contains beta-2 adrenergic receptors. Activation by catecholamines or beta-2 agonists (salbutamol) increases intracellular cAMP via adenylyl cyclase, causing smooth muscle relaxation and bronchodilation. Cholinergic (muscarinic) stimulation does the opposite — causes bronchoconstriction and increased mucus secretion.
- Mast cells in the bronchial mucosa bear surface IgE (via FcεRI). Cross-linking by allergen triggers degranulation releasing histamine, tryptase, and prostaglandins (early bronchoconstriction) and newly synthesised leukotrienes (prolonged bronchoconstriction and oedema).
- FEV₁ (forced expiratory volume in 1 second) and FVC (forced vital capacity) are the two primary spirometric indices. In obstructive disease (asthma, COPD) FEV₁ falls more than FVC, reducing the FEV₁/FVC ratio below 0.80 (or below the lower limit of normal, LLN). In restrictive disease both fall proportionately, ratio normal or elevated.
- You have seen allergic rhinitis in the previous module — recall that 40–50% of children with AR will develop asthma (the allergic march), and that the same IgE-Th2 inflammation drives both upper and lower airway disease ('one airway, one disease').
Clinical Presentation and Types of Childhood Asthma
Asthma in children does not present as a single uniform disease but as a heterogeneous group of phenotypes whose clinical expression varies with age, trigger exposure, and atopic status. The cardinal clinical features shared across all presentations are episodes of reversible bronchospasm: wheeze (a high-pitched expiratory sound caused by turbulent airflow through narrowed lower airways), breathlessness, chest tightness, and cough — particularly a dry, nocturnal or early-morning cough that is pathognomonic in the right clinical context. The defining characteristic that distinguishes asthma from other obstructive lung conditions is variability — symptoms wax and wane over time, are worse with triggers, and are at least partially reversible with bronchodilators.
Age-specific phenotypes are clinically important because the diagnosis and management differ:
Infants and toddlers (age <3 years) — 'preschool wheeze': Wheeze in this age group is common and heterogeneous. Episodic (viral) wheeze — discrete episodes triggered exclusively by viral upper respiratory infections, with complete resolution between episodes and no intercurrent symptoms — has a good prognosis and frequently resolves by age 6. Multiple-trigger wheeze — symptoms between viral episodes, triggered also by allergens, cold air, and exercise — is more likely to represent early persistent atopic asthma. Since spirometry is not feasible below age 5–6 years, the diagnosis of 'asthma' in this age group remains a clinical and probabilistic one. A positive Asthma Predictive Index (API): ≥3 episodes of wheeze in a year PLUS ≥1 major criterion (parental asthma OR physician-diagnosed atopic dermatitis in the child) OR ≥2 minor criteria (eosinophilia ≥4%, wheeze apart from colds, allergic rhinitis) — predicts persistent asthma with reasonable specificity.
School-age children (6–12 years): Classic atopic asthma — allergen-triggered, associated with AR and atopic dermatitis, spirometry-confirmable. This is the age group in which formal GINA severity and control classification applies most reliably. Exercise-induced bronchoconstriction (EIB) — wheeze, chest tightness, and cough during or after 5–10 minutes of sustained exercise — may be the sole presentation; a 15-minute free-run test or exercise-challenge spirometry can confirm it.
Adolescents: Symptoms often under-reported or attributed to 'being unfit'. Tobacco smoking (active or passive), allergen avoidance non-compliance, and poor inhaler technique are major management challenges. Vocal cord dysfunction (VCD) can mimic asthma — inspiratory stridor, throat tightness, flow-volume loop with variable extrathoracic obstruction, no response to SABA.
Common triggers in Indian children: house-dust mite (the single most important perennial trigger), cockroach allergen, mould spores, Bermuda grass pollen, tobacco smoke, biomass fuel combustion, cold air, exercise, viral respiratory infections (rhinovirus, RSV), strong odours, and non-steroidal anti-inflammatory drugs (aspirin-exacerbated respiratory disease — less common in children than adults).
Differential diagnoses to exclude before labelling asthma:
• Foreign body aspiration — sudden onset, unilateral wheeze or absent breath sounds, typically age 1–3 years; CXR (expiratory) or bronchoscopy
• Tracheomalacia / bronchomalacia — continuous wheeze from birth, worse with crying
• Cystic fibrosis — productive cough, failure to thrive, recurrent infections, sweat chloride test
• Congenital heart disease — cardiac wheeze, signs of heart failure
• GERD — cough-dominant, worse after feeds, responds to antireflux treatment
• Vascular ring — stridor + dysphagia, CXR shows tracheal deviation
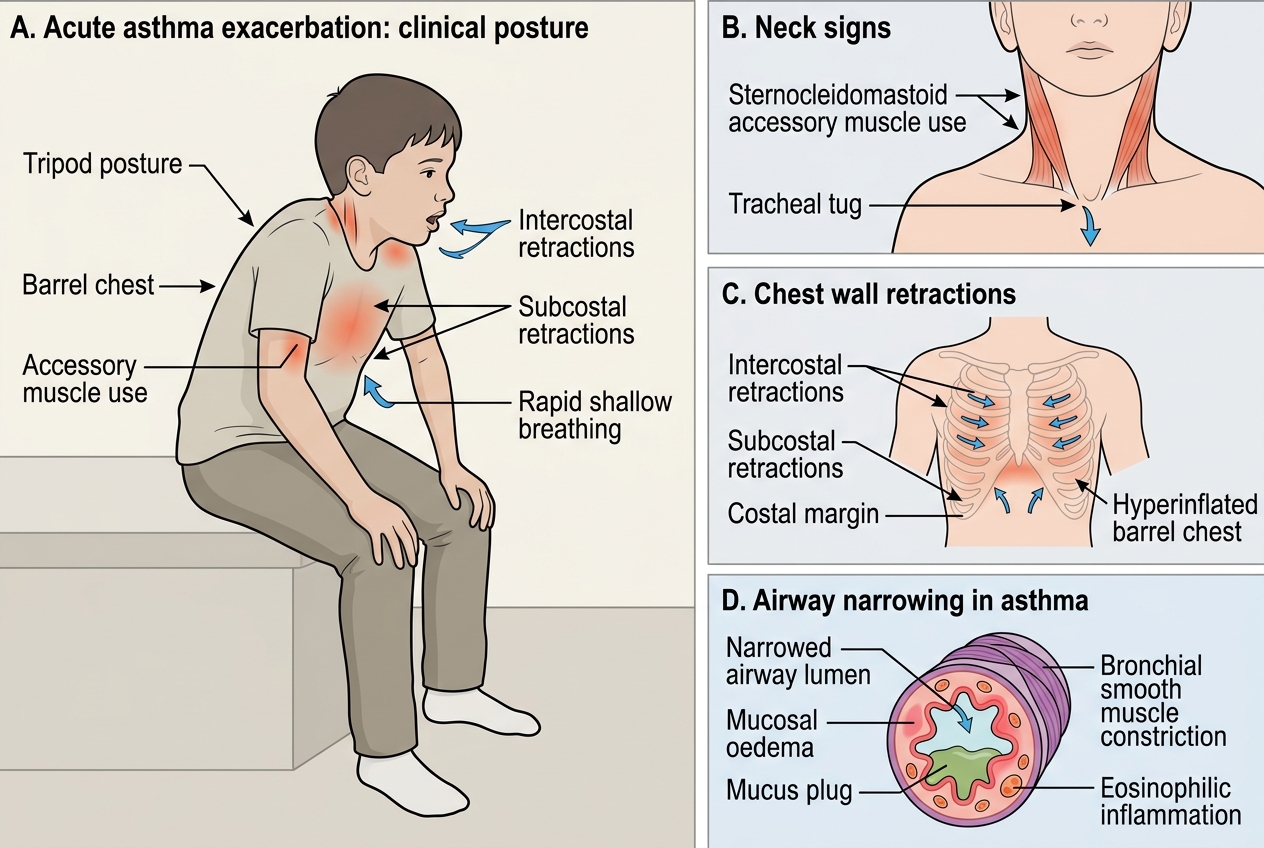
Clinical Signs of Acute Asthma Exacerbation
Pathophysiology and Aetiology of Asthma
The pathophysiology of asthma is fundamentally an interaction between genetic susceptibility, environmental allergen and irritant exposure, and a dysregulated Th2 immune response that produces three interlocking abnormalities: airway inflammation, bronchial hyperreactivity, and — in chronic disease — airway remodelling.
Immune and inflammatory mechanisms: In atopic asthma (the dominant paediatric phenotype), the initiating event is sensitisation to an inhaled allergen (typically HDM in India), mediated by the same Th2 polarisation, IgE class switching, mast cell priming, and FcεRI-mediated degranulation described in allergic rhinitis. The key distinction from rhinitis is the anatomical site and the effector cell population: in the bronchi, eosinophils are the dominant inflammatory cell (recruited by IL-5), and their granule products — major basic protein, eosinophil cationic protein, and eosinophil-derived neurotoxin — cause direct epithelial damage, increase bronchial hyperreactivity, and perpetuate the inflammatory cycle. Mast cell degranulation releases histamine (early bronchospasm), prostaglandin D₂, and leukotrienes C₄/D₄/E₄ (prolonged bronchospasm and mucosal oedema). The late-phase reaction 4–8 hours later involves eosinophil influx and Th2 cytokine amplification, causing persistent airways narrowing.
Airway structural abnormalities:
- Bronchospasm: smooth-muscle contraction (reversible with SABA)
- Mucosal oedema: vascular leakage driven by mediators (partially reversed by corticosteroids)
- Mucus hypersecretion and plugging: goblet-cell hyperplasia driven by IL-13; viscid mucus plugs cause areas of atelectasis
- Airway remodelling (in long-standing uncontrolled asthma): subepithelial fibrosis (TGF-β driven), smooth muscle hypertrophy and hyperplasia, goblet cell hyperplasia, angiogenesis — these structural changes are IRREVERSIBLE and explain the progressive fixed airflow obstruction seen in some adults with childhood-onset asthma. Early controller therapy with ICS can attenuate (not fully prevent) remodelling.
Risk factors and aetiology:
- Genetic: polygenic; first-degree relative with asthma 2–3× risk; chromosome 5q (IL-4/IL-5/IL-13 cluster), 11q (FcεRIβ), 17q (ORMDL3 — identified in GWAS as strong paediatric asthma susceptibility locus)
- Atopic sensitisation: strongest identifiable risk factor; 60–80% of childhood asthma is atopic
- Early-life respiratory infections: RSV bronchiolitis in infancy strongly associated with recurrent wheeze; rhinovirus wheezing illnesses in sensitised infants predict asthma
- Environmental: HDM, cockroach, indoor moulds, tobacco smoke, biomass fuel, outdoor air pollution (PM₂.₅, NO₂), traffic-related pollution
- Obesity: a non-atopic asthma phenotype; adipokines promote airway inflammation
- Prematurity and low birthweight: structurally smaller airways → higher airway resistance
- The hygiene hypothesis: reduced childhood microbial diversity (rural → urban migration, antibiotic use, Caesarean birth) shifts immune balance toward Th2 predominance
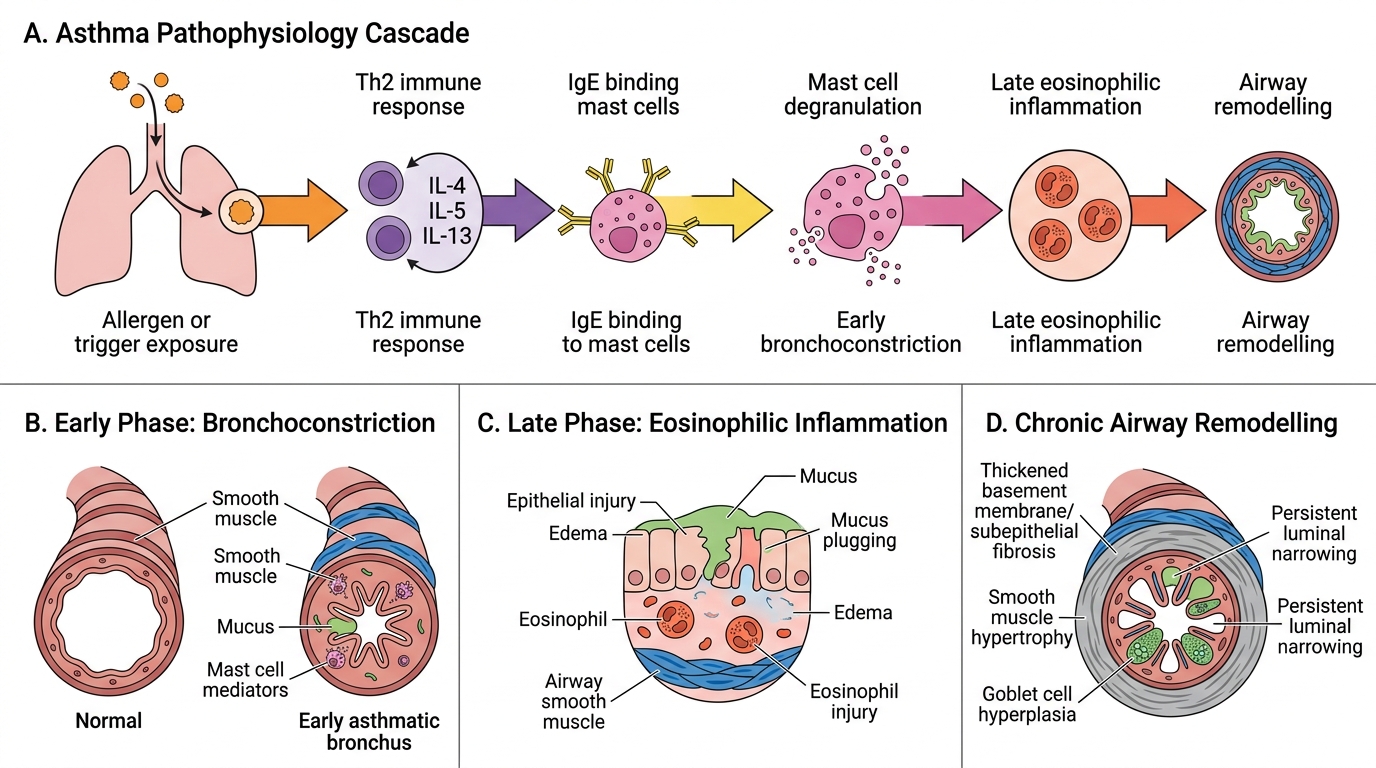
Asthma Pathophysiology: From Trigger Exposure to Airway Remodelling
SELF-CHECK
An 8-year-old with known asthma has daily daytime symptoms, wakes from sleep with coughing approximately twice per week, and requires salbutamol every day. Spirometry shows FEV₁ 65% predicted. Using GINA criteria, what is the severity classification?
A. Intermittent asthma
B. Mild persistent asthma
C. Moderate persistent asthma
D. Severe persistent asthma
Reveal Answer
Answer: C. Moderate persistent asthma
GINA moderate persistent asthma is characterised by ALL of: daily daytime symptoms, nocturnal awakenings ≥1 per week (not necessarily nightly), SABA needed daily, and FEV₁ 60–80% predicted. This child meets all four criteria. Intermittent asthma has symptoms ≤2 days/week and FEV₁ ≥80%. Mild persistent has symptoms >2 days/week but not daily and FEV₁ ≥80%. Severe persistent has continuous daytime symptoms, frequent nocturnal awakenings, and FEV₁ <60%. This child's FEV₁ of 65% places him in the moderate (60–80%) range.
Diagnosis, Severity Classification, and Pulmonary Function Testing
The diagnosis of asthma in children aged ≥5–6 years is established by combining a compatible clinical history (episodic wheeze, cough, breathlessness with the characteristic triggers and variability) with objective evidence of reversible variable airflow obstruction on pulmonary function testing. In children below 5 years, where reliable spirometry is not feasible, the diagnosis remains clinical and probabilistic (supported by the Asthma Predictive Index and response to empirical trial of SABA ± low-dose ICS). The integration of history with objective lung-function data is not merely a diagnostic formality — it enables you to classify severity accurately, monitor treatment response over time, and detect early decline in lung function before the child's symptoms change. Pulmonary function testing is therefore both a diagnostic and a monitoring tool, and every child confirmed to have asthma should have a baseline spirometry documented before starting treatment and re-checked at 3–6 monthly intervals. Understanding when and how to order PFT, and how to interpret the results, is a core clinical competency that directly informs treatment decisions.
Provided image
Pulmonary Function Testing (PFT) — Indications (PE28.4):
PFT (principally spirometry) is indicated in childhood asthma for the following:
- Diagnosis confirmation: to establish the presence and degree of airflow obstruction and confirm reversibility — when the clinical presentation alone is insufficient or the diagnosis is in doubt
- Severity assessment: FEV₁ is one of the four GINA severity criteria; objective lung function data supplement symptom history in initial classification
- Monitoring disease control and treatment response: serial spirometry detects deterioration or improvement in lung function with therapy; guides step-up or step-down decisions
- Pre-bronchodilator and post-bronchodilator assessment: mandatory in initial workup; reversibility confirms the diagnosis
- Exercise challenge: formal incremental exercise test on a treadmill or cycle ergometer with pre- and post-exercise spirometry; confirms exercise-induced bronchoconstriction (>12% fall in FEV₁ post-exercise)
- Assessment of exacerbation severity: PEFR (peak expiratory flow rate) is the bedside PFT modality for grading acute exacerbation severity and monitoring response to bronchodilator therapy
- Occupational or environmental exposure assessment: serial PEFRs at work/school vs at home to identify trigger-specific patterns
Spirometric findings and interpretation in asthma:
In symptomatic asthma, spirometry shows an obstructive pattern: FEV₁/FVC ratio reduced (<0.80 or below the lower limit of normal, LLN), with disproportionate reduction in FEV₁ relative to FVC. After administering a SABA (salbutamol 400 µg via spacer, or 2.5 mg nebulised), a post-bronchodilator FEV₁ increase of ≥12% confirms significant reversibility and strongly supports the diagnosis of asthma. In children, the absolute 200 mL criterion commonly used in adults may not apply to small children; the percentage criterion (≥12%) is the more reliable paediatric threshold. Between attacks, spirometry may be entirely normal — a normal result does not exclude asthma if the clinical history is compelling. In that situation, methacholine or histamine bronchoprovocation (specialist setting) can demonstrate bronchial hyperreactivity.
PEFR (Peak Expiratory Flow Rate): PEFR is practical in children ≥5–6 years using a portable peak flow meter. Normal PEFR values are referenced against predicted values for height and sex. PEFR % predicted: >80% = mild exacerbation; 40–69% = moderate; <40% = severe. PEFR variability (diurnal variation: [morning PEFR − evening PEFR] / evening PEFR × 100) >20% is diagnostic of variable airflow obstruction in asthma.
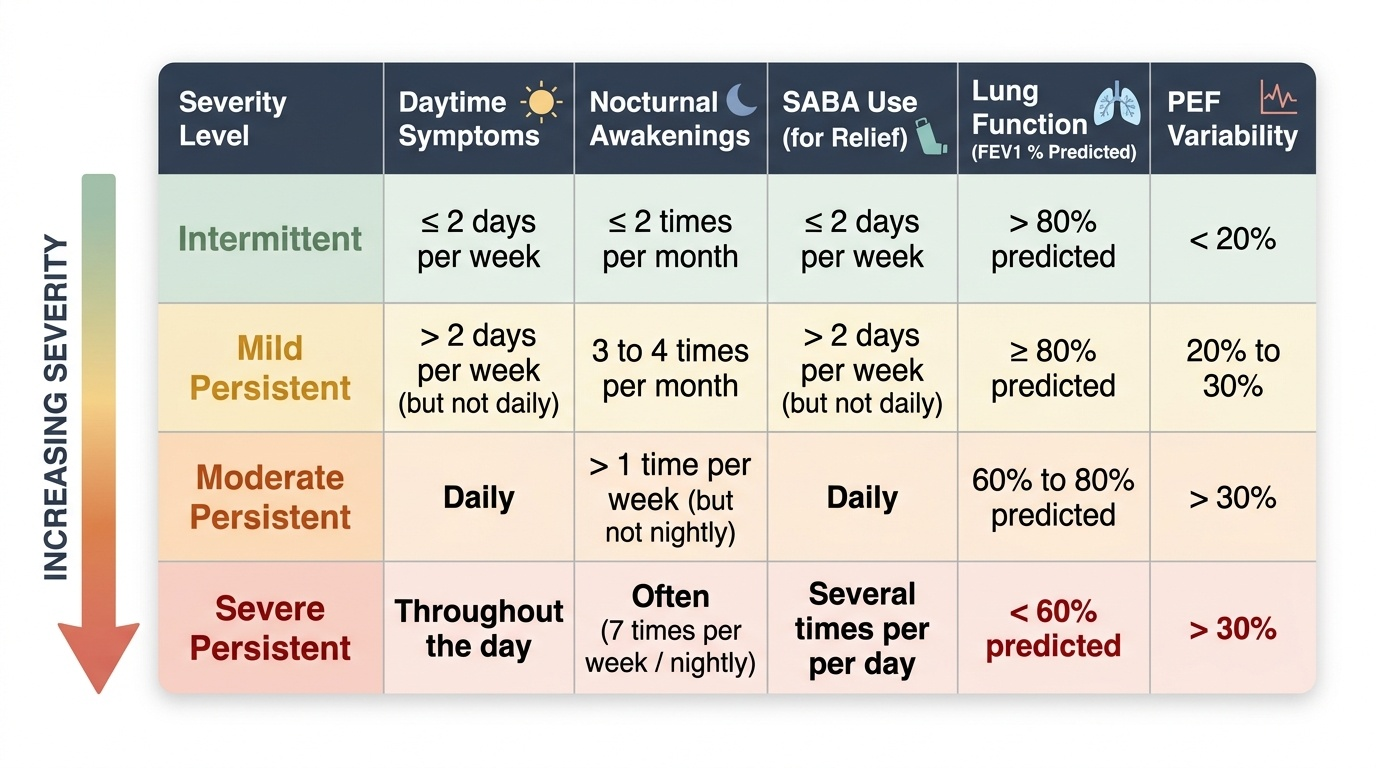
GINA Severity Classification (applied at initial assessment before starting treatment, or in a patient not on controller therapy):
| Severity | Daytime symptoms | Nocturnal awakenings | SABA use | FEV₁ (% predicted) | PEF variability |
|---|---|---|---|---|---|
| Intermittent | ≤2 days/week | ≤2/month | ≤2 days/week | ≥80% | <20% |
| Mild persistent | >2 days/week, not daily | >2/month, not weekly | >2 days/week, not daily | ≥80% | 20–30% |
| Moderate persistent | Daily | ≥1/week, not nightly | Daily | 60–80% | >30% |
| Severe persistent | Continuous | Nightly | Several times/day | <60% | >30% |
GINA Control Classification (applied during ongoing treatment to decide step-up or step-down): assesses the same four domains over the prior 4 weeks. Well-controlled = all four domains minimal/none; Partially controlled = 1–2 domains present; Uncontrolled = 3–4 domains present. Control and severity are distinct constructs — a child with initially severe asthma can achieve well-controlled status on appropriate therapy.
CLINICAL PEARL
The 'silent chest' paradox: Students commonly assume that the louder the wheeze, the more severe the attack. The inverse is often true in a near-fatal exacerbation: as the child exhausts their respiratory reserve and airflow becomes critically limited, wheeze may disappear — not because the airway has opened, but because there is too little air movement to generate turbulence. A child who presented with loud wheeze that has now become silent, combined with cyanosis, fatigue, or altered consciousness, is in imminent respiratory failure and needs immediate ICU-level intervention. Always correlate wheeze intensity with work of breathing, accessory muscle use, SpO₂, and ability to speak — never use wheeze alone as a severity marker.