Page 5 of 12
PE28.2-5 | Childhood Asthma — SDL Guide (Part 2)
Long-term Management: Stepwise Controller Therapy
The goal of long-term asthma management is control — achieving minimal or no symptoms, no exacerbations, normal lung function, and normal activity — at the lowest medication burden. The GINA stepwise framework (Steps 1–5) achieves this by escalating (step-up) or reducing (step-down) treatment based on the control classification reassessed at every visit. Two non-negotiable principles underpin the entire framework: inhaled corticosteroids (ICS) are the cornerstone of controller therapy and should be initiated in any child with persistent asthma; and SABAs are relievers, not controllers — a child using SABA more than 2 days a week for symptom relief needs a step-up in controller therapy, not more SABA.
GINA Step-care for children ≥6 years:
Step 1 — Intermittent asthma (as-needed SABA only):
Children with infrequent, brief symptoms (≤2 days/week) and no risk factors for exacerbation can be managed with SABA (salbutamol MDI + spacer, or nebulisation for young children) on an as-needed basis. No controller is needed at Step 1. GINA 2023 notes that low-dose ICS-formoterol (as-needed) is an alternative Step 1 option in adolescents/adults but this is not yet widely applied in young children.
Step 2 — Mild persistent asthma (low-dose ICS):
Low-dose ICS (budesonide 100–200 µg/day, or beclomethasone 100–200 µg/day, or fluticasone propionate 100–200 µg/day) is the preferred controller. ICS suppresses eosinophilic airway inflammation, reduces bronchial hyperreactivity, prevents exacerbations, and improves lung function. Montelukast (LTRA) is an alternative for children with AR + asthma or those who cannot use inhalers. Regular follow-up at 2–4 weeks after starting, then 2–3 months.
Step 3 — Moderate persistent asthma:
Escalate to medium-dose ICS (budesonide 200–400 µg/day) OR low-dose ICS + LABA (ICS/formoterol or ICS/salmeterol combination inhaler). LABA is NEVER used as monotherapy in asthma — it must always be combined with ICS because LABA alone can paradoxically increase asthma mortality risk. In children <5 years, medium-dose ICS rather than ICS/LABA combination is preferred. Adding montelukast to low-dose ICS is an alternative at Step 3 for children with comorbid AR.
Step 4 — Severe persistent asthma:
Medium-to-high dose ICS/LABA combination. Consideration of adding tiotropium (long-acting muscarinic antagonist, LAMA) — soft-mist inhaler approved as add-on for severe asthma ≥6 years. Sustained-release theophylline is a third-line add-on but has a narrow therapeutic index and CNS side-effects; not preferred in children.
Step 5 — Refractory asthma:
High-dose ICS/LABA ± add-on agents (LAMA, theophylline). Refer to a paediatric pulmonologist. Consider biologic agents: omalizumab (anti-IgE monoclonal antibody — approved ≥6 years for severe allergic asthma with confirmed sensitisation and inadequate control on high-dose ICS/LABA) given as subcutaneous injections every 2–4 weeks; dose is weight- and IgE-level-based. Mepolizumab (anti-IL-5) for severe eosinophilic asthma (approved ≥12 years; used off-label in younger children under specialist guidance).
Step-up and step-down protocol: Step up if control is partial or uncontrolled for ≥3 months; step down if well-controlled for ≥3 months at the current step. Before stepping up, always check: inhaler technique, adherence, allergen exposure, and absence of comorbidities (AR, GERD, obesity) that could be driving symptoms.
Prevention: Trigger avoidance (HDM encasements, tobacco smoke-free home, pet dander), allergen immunotherapy for confirmed sensitised moderate-severe atopic asthma, influenza vaccination annually (reduces asthma exacerbations), pneumococcal vaccination per NIS (PCV given at 6, 10, 14 weeks and 9 months under recent IAP expansion recommendations).
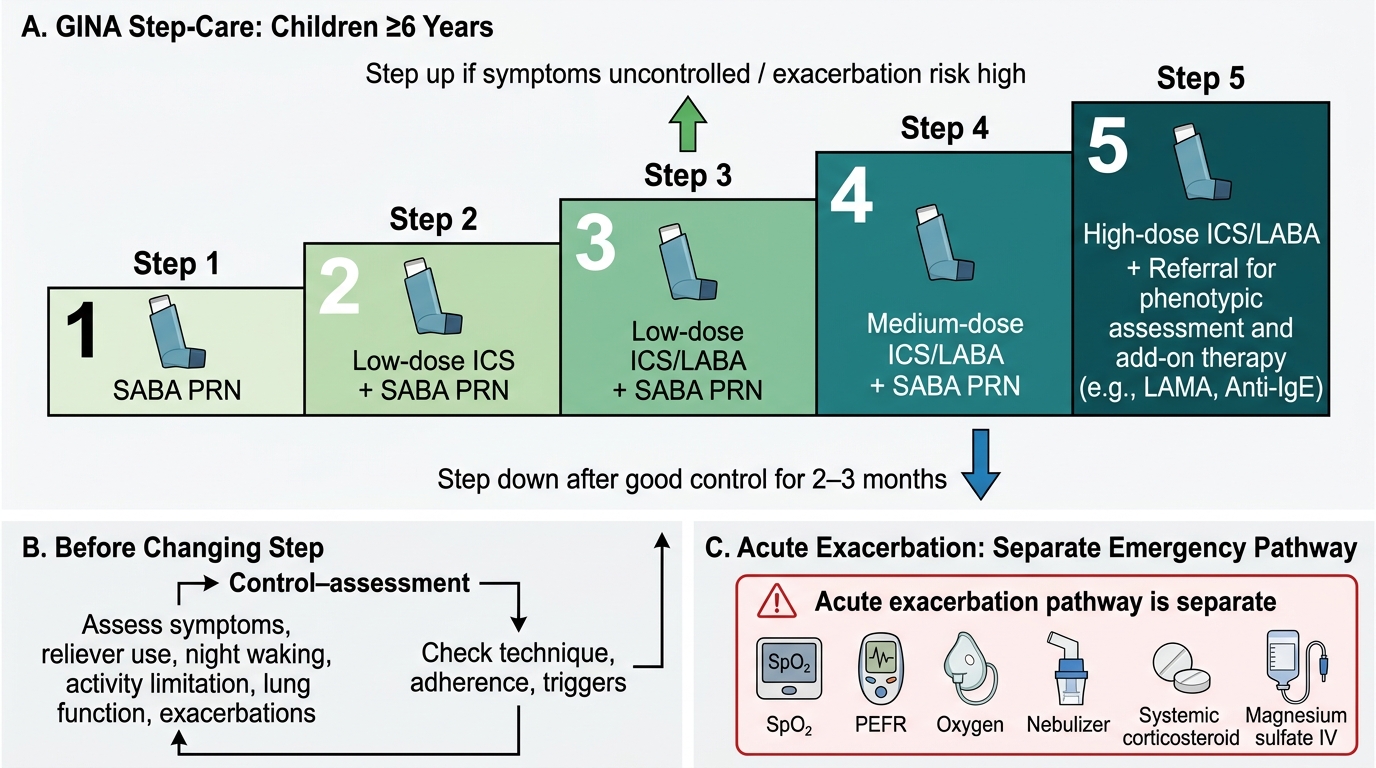
GINA Step-Care for Asthma in Children ≥6 Years
Acute Exacerbation Management
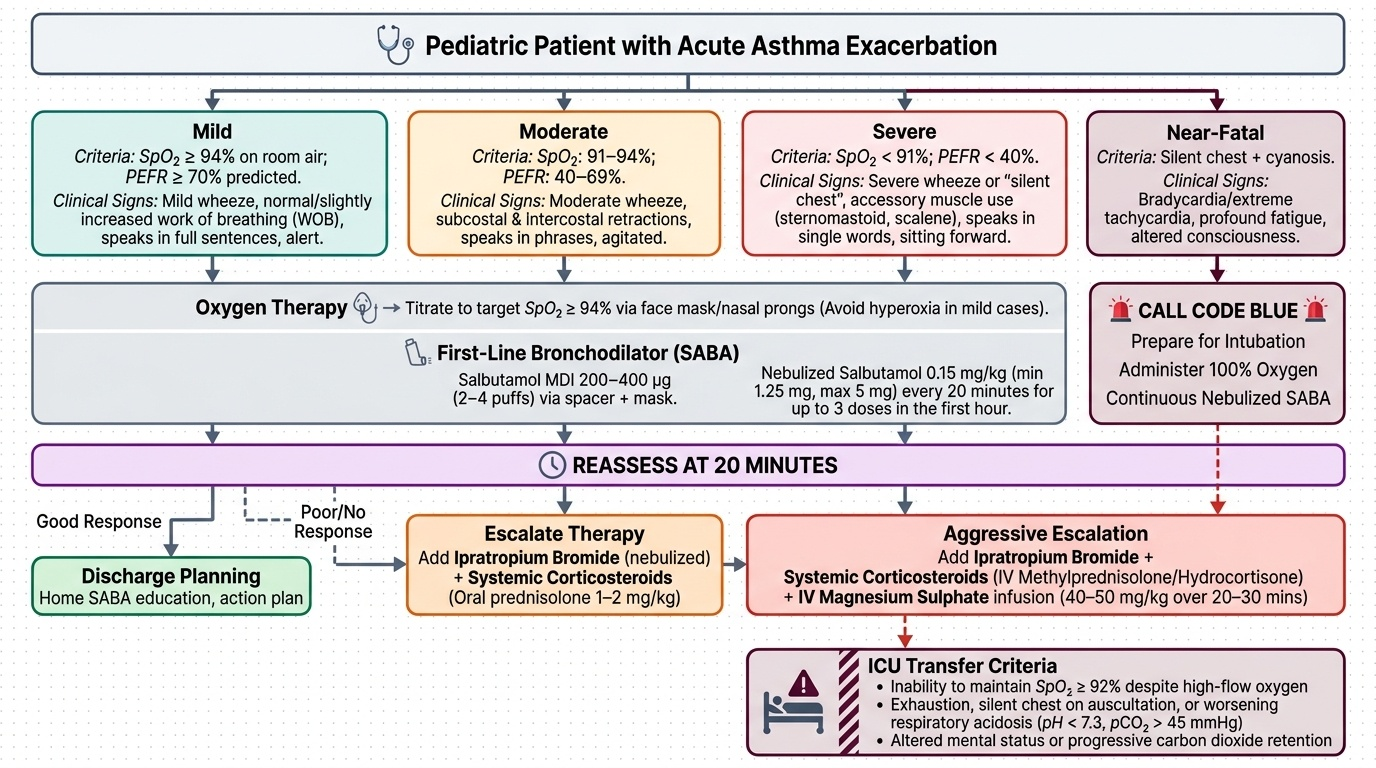
An acute asthma exacerbation is a progressive increase in symptoms (wheeze, breathlessness, chest tightness, cough) with a measurable decrease in expiratory flow that requires a change in treatment. Exacerbation severity is classified on a separate grid from the chronic severity/control classification — it uses an integrated assessment of clinical signs, SpO₂, and PEFR to determine the immediate management pathway. Recognising the severity of an acute exacerbation correctly and initiating treatment within minutes is one of the most time-critical decisions in paediatric emergency medicine. The clinician who misclassifies a severe exacerbation as mild — because the child looks 'not too bad' or has loud wheeze — may delay the life-saving interventions (oxygen, back-to-back nebulisation, systemic corticosteroids, and magnesium sulphate) that convert a near-fatal episode into a full recovery. Every assessment of an acutely wheezing child must therefore follow a structured severity-grading framework, combining clinical signs with objective SpO₂ and PEFR, before any management decision is made.
Provided image
Severity assessment — four categories:
- Mild: SpO₂ ≥94% on room air; PEFR ≥70% predicted; mild wheeze; normal or slightly increased work of breathing; child can speak full sentences; alert
- Moderate: SpO₂ 91–94%; PEFR 40–69%; moderate wheeze; subcostal and intercostal retractions; speaks phrases (not full sentences); agitated
- Severe: SpO₂ <91%; PEFR <40%; severe or absent wheeze ('silent chest'); accessory muscle use (sternomastoid, scalene); speaks single words; sitting forward; paradoxical abdominal movement
- Near-fatal / impending respiratory failure: silent chest + cyanosis + bradycardia or extreme tachycardia + fatigue + altered consciousness → CALL CODE BLUE; prepare for intubation
Management — time-critical, stepwise:
Immediate (all exacerbations):
- Oxygen: titrate to SpO₂ ≥94% via face mask or nasal prongs (avoid high-flow O₂ causing hyperoxia in mild cases, which can worsen V/Q mismatch)
- SABA (salbutamol): 0.15 mg/kg per dose (minimum 1.25 mg, maximum 5 mg) by nebulisation — repeat every 20 minutes for 3 doses in the first hour for moderate-severe exacerbations; then 1–4-hourly based on response. Alternatively, salbutamol MDI 200–400 µg (2–4 puffs) via spacer + mask is equivalent to nebulisation for mild-moderate exacerbation — BUT in severe exacerbation, nebulisation is preferred as it delivers drug while the child breathes passively.
Moderate-severe exacerbations — add:
- Ipratropium bromide (a short-acting muscarinic antagonist, SAMA): 250 µg per dose by nebulisation, mixed with salbutamol — every 20 minutes for 3 doses; then every 4–6 hours. The combination of SABA + SAMA provides superior bronchodilation in moderate-severe exacerbations compared to SABA alone (Cochrane evidence). Ipratropium is NOT a maintenance controller — it is used exclusively as an acute add-on.
- Systemic corticosteroids: prednisolone 1–2 mg/kg/day orally (maximum 40 mg/day) for 3–5 days; or hydrocortisone 5 mg/kg IV every 6 hours for severe cases (IV when oral route not feasible). Corticosteroids suppress the late-phase eosinophilic inflammation responsible for sustained bronchospasm, reduce the need for hospitalisation, and prevent relapse. Begin within 1 hour of presentation in moderate-severe exacerbation.
Severe exacerbations — additionally:
- Magnesium sulphate IV: 25–75 mg/kg (maximum 2.5 g) by slow IV infusion over 20 minutes — indicated when SABA + ipratropium + systemic corticosteroids fail to produce adequate response within 1 hour. Acts as a smooth-muscle relaxant by antagonising calcium-mediated bronchospasm. Monitor for hypotension and bradycardia during infusion.
- Heliox (helium-oxygen mixture) — reduces turbulent airflow resistance; not widely available in India.
- IV salbutamol or aminophylline: reserve for ICU management of near-fatal exacerbation.
Discharge criteria and follow-up:
Child can be discharged when SpO₂ ≥95% on room air, PEFR >70% predicted, no retractions, tolerating oral medications, and reliable carer is available. At discharge: ensure family has a written Asthma Action Plan (green/yellow/red zone guidance), prescribe ICS controller, provide SABA for acute relief, and book follow-up within 2–7 days.
Drug doses for acute asthma in children:
| Drug | Route | Dose | Frequency |
|---|---|---|---|
| Salbutamol | Nebuliser | 0.15 mg/kg (min 1.25 mg, max 5 mg) | Every 20 min × 3, then prn |
| Salbutamol | MDI + spacer | 2–4 puffs (100 µg/puff) | Every 20 min × 3 (mild-moderate) |
| Ipratropium bromide | Nebuliser | 250 µg per dose | Every 20 min × 3, then every 6 h |
| Prednisolone | Oral | 1–2 mg/kg/day (max 40 mg) | Once daily × 3–5 days |
| Hydrocortisone | IV | 5 mg/kg per dose | Every 6 h (severe) |
| Magnesium sulphate | IV | 25–75 mg/kg (max 2.5 g) | Single dose over 20 min |
| Oxygen | Mask/prongs | Titrate to SpO₂ ≥94% | Continuous until stable |
Nebulisation Technique and Inhaler Devices in Children
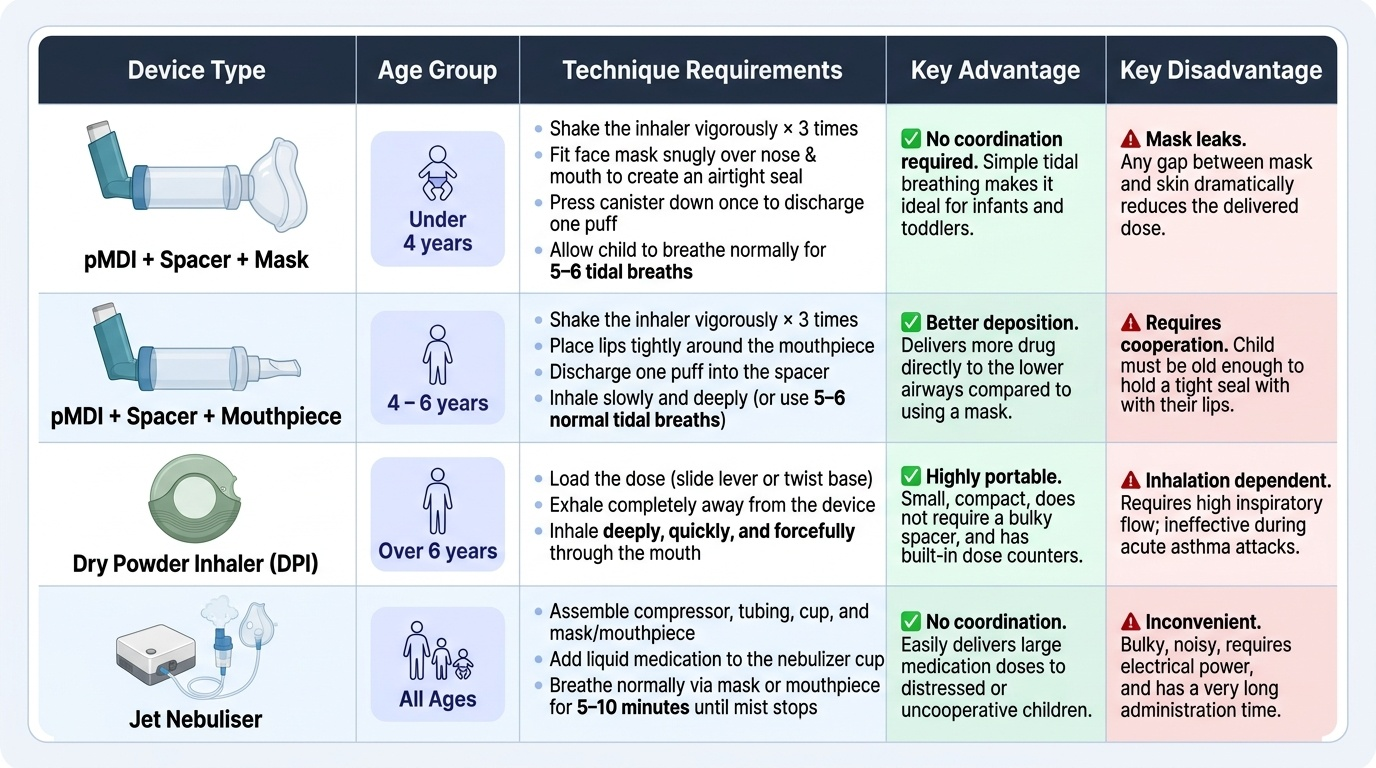
The correct delivery of inhaled bronchodilators and controllers is a core clinical competency because technique failure — not medication failure — is the most common cause of inadequate asthma control in children. Studies show that up to 80% of children and their carers use inhalers incorrectly, and that correcting technique alone improves control equivalently to a step-up in medication. Understanding the properties of each device and matching the device to the child's age and capability is therefore as therapeutically important as selecting the right drug.
Provided image
Pressurised metered-dose inhaler (pMDI) with spacer (most important device for children):
The pMDI discharges a high-velocity aerosol cloud; without a spacer, up to 80% of the dose impacts the oropharynx rather than reaching the airways. A spacer (valved holding chamber, VHC) slows the aerosol, allows the propellant to evaporate, and converts a coordination-dependent task into simple tidal breathing. The spacer is essential in all children below 5–6 years and preferred in all ages for improved lower airway deposition.
Technique — pMDI + spacer (with mask, for children <4 years):
1. Shake the inhaler vigorously × 3 times
2. Remove cap; attach inhaler to spacer; fit face mask snugly over nose and mouth
3. Press canister down ONCE to discharge one puff into the spacer
4. Child breathes normally through mask for 5–6 tidal breaths (or until spacer valve stops moving)
5. Remove mask; wait 30–60 seconds before next puff
6. For ICS: rinse mouth with water after use to prevent oral candidiasis
7. Wash spacer with mild detergent weekly (NOT dishwasher — electrostatic charge reduced by detergent, which increases drug deposition)
Technique — pMDI + spacer (with mouthpiece, for children ≥4–6 years):
Same as above but child seals lips around spacer mouthpiece and inhales slowly and deeply after puff discharge; breath-hold 5–10 seconds if possible.
Dry powder inhaler (DPI — Turbuhaler, Rotahaler, Accuhaler):
DPI devices require a vigorous, deep inspiratory effort to disperse and aerosolise the dry powder. Inspiratory flow needed: >30–60 L/min. This flow rate is typically achievable only in children ≥6–8 years with coaching. DPIs have no propellant (no spacer needed), are breath-actuated (no coordination required between canister press and inhalation), and are environmentally preferable. They CANNOT be used in very young children or during severe exacerbation when inspiratory flow is severely diminished.
Jet nebuliser (nebulisation):
A jet nebuliser uses compressed air (or oxygen) to convert liquid medication into an inhalable aerosol mist. Drugs commonly nebulised in children: salbutamol (0.15 mg/kg diluted in 2–3 mL normal saline), ipratropium bromide (250 µg), budesonide suspension (0.5–1 mg for acute exacerbation in children who cannot use pMDI).
Administration technique — nebulisation (PE28.5 — observe):
1. Check drug, dose, and diluent (usually 0.9% normal saline to total volume 2–3 mL)
2. Place drug + diluent in nebuliser chamber; attach tubing to compressor
3. Fit face mask snugly (or mouthpiece for children ≥5 years who cooperate)
4. Start compressor; verify mist from mask exhalation ports
5. Child breathes normally through mask; continue until mist stops (nebuliser 'sputter' — typically 8–12 minutes)
6. Turn off compressor; rinse and dry nebuliser chamber after each use
7. Do NOT add two medications in the same chamber without specific compatibility confirmation (salbutamol + ipratropium: compatible and commonly co-nebulised; ipratropium + budesonide: check)
8. For ICS (budesonide nebulised): rinse child's face and mouth with water after
Age-appropriate device selection:
| Age | Preferred device | Notes |
|---|---|---|
| <2–3 years | pMDI + spacer + face mask | Tidal breathing; mask must seal well |
| 3–5 years | pMDI + spacer + face mask → transition to mouthpiece | Begin mouthpiece training at age 4 |
| 5–6 years | pMDI + spacer + mouthpiece | Can manage with coaching |
| ≥6–8 years | pMDI + spacer OR DPI (if sufficient flow) | Spirometry guides DPI suitability |
| Acute severe | Jet nebuliser (any age) | Passive drug delivery; no effort needed |
SELF-CHECK
A 4-year-old with moderate persistent asthma uses a salbutamol pMDI with spacer and face mask at home. His mother reports the inhaler 'doesn't seem to work well'. On review of technique you find she presses the canister twice before putting the mask on the child. What is the most likely reason for poor drug delivery?
A. The spacer is too large for a 4-year-old
B. Two puffs discharged simultaneously increases the dose excessively
C. Actuating the canister before fitting the mask loses most of the dose before inhalation
D. A pMDI cannot be used in a 4-year-old — a DPI should be used instead
Reveal Answer
Answer: C. Actuating the canister before fitting the mask loses most of the dose before inhalation
The canister must be pressed ONCE AFTER the mask is in place (or once the mouthpiece is sealed), so that the aerosol cloud held in the spacer is available for the child's tidal breathing immediately. Pressing before fitting the mask allows the aerosol to escape from the spacer open end, reducing effective drug delivery dramatically. Option A is incorrect: standard spacers are appropriate for children of this age. Option B is incorrect: while double-dosing is an error, the question describes pressing the canister before applying the mask — the problem is timing (loss before inhalation), not dose. Option D is incorrect: pMDI + spacer + face mask is the preferred device for a 4-year-old; DPI requires a vigorous inspiratory flow (>30–60 L/min) not achievable in this age group.