Page 6 of 12
PE28.2-5 | Childhood Asthma — SDL Guide (Part 3)
Self-Assessment and Key Take-Aways
Childhood asthma is the most common chronic disease in paediatric practice — chronic airway inflammation driven by Th2 IgE-mast cell-eosinophil pathways, expressing as variable reversible airflow obstruction. This module has covered a broad but tightly integrated set of competencies: the pathophysiology that explains why ICS prevents exacerbations but SABA does not; the GINA severity and control classification grids that drive prescribing decisions; the PFT indications and spirometric criteria that confirm the diagnosis; the stepwise controller framework from intermittent SABA-only through to biologic therapy; the time-critical acute exacerbation algorithm with weight-based drug doses; and the inhaler-device selection and nebulisation technique that determine whether the correct drug actually reaches the child's airways. These pieces form a coherent clinical framework, not a list of isolated facts. Before reviewing the key points below, try to reconstruct the management of Arjun from memory — that active-recall exercise will embed the framework more durably than re-reading the notes. The essential take-aways are:
Diagnosis: Variable wheeze, breathlessness, and cough with characteristic triggers; confirmed by spirometry showing obstructive pattern with ≥12% reversibility after SABA. In children <5 years: clinical diagnosis using Asthma Predictive Index.
Two classification grids — do NOT confuse them:
- Severity (initial assessment, untreated): Intermittent / Mild persistent / Moderate persistent / Severe persistent — based on symptom frequency, nocturnal awakenings, SABA use, FEV₁ % predicted
- Control (ongoing management): Well-controlled / Partially controlled / Uncontrolled — drives step-up or step-down decisions
- Acute exacerbation severity (separate third grid): Mild / Moderate / Severe / Near-fatal — drives immediate management
PFT indications (PE28.4): Diagnosis confirmation, severity assessment, monitoring, reversibility testing, exercise challenge, exacerbation PEFR grading
Stepwise controller therapy (GINA):
- Step 1 (intermittent): SABA as needed only
- Step 2 (mild persistent): low-dose ICS (first-line controller)
- Step 3 (moderate persistent): medium-dose ICS OR low-dose ICS + LABA
- Step 4 (severe persistent): medium-high ICS/LABA ± LAMA
- Step 5 (refractory): high-dose ICS/LABA + biologics (omalizumab)
- LABA NEVER as monotherapy; ICS is the backbone at Steps 2–5
Acute exacerbation management:
- Oxygen → SABA nebulisation (0.15 mg/kg every 20 min × 3) → add ipratropium (moderate-severe) → systemic corticosteroids (prednisolone 1–2 mg/kg/day max 40 mg) → magnesium sulphate IV (severe non-responder: 25–75 mg/kg max 2.5 g over 20 min)
- Silent chest = medical emergency; SpO₂ <91% = severe
Nebulisation (PE28.5): 0.15 mg/kg salbutamol in 2–3 mL saline; drive with compressed air or O₂; tidal breathing through snug mask; rinse face after ICS nebulisation
Inhaler device by age: pMDI + spacer + mask (< 4 yr) → pMDI + spacer + mouthpiece (4–6 yr) → DPI (≥ 6–8 yr with adequate flow); nebuliser for any age in acute severe
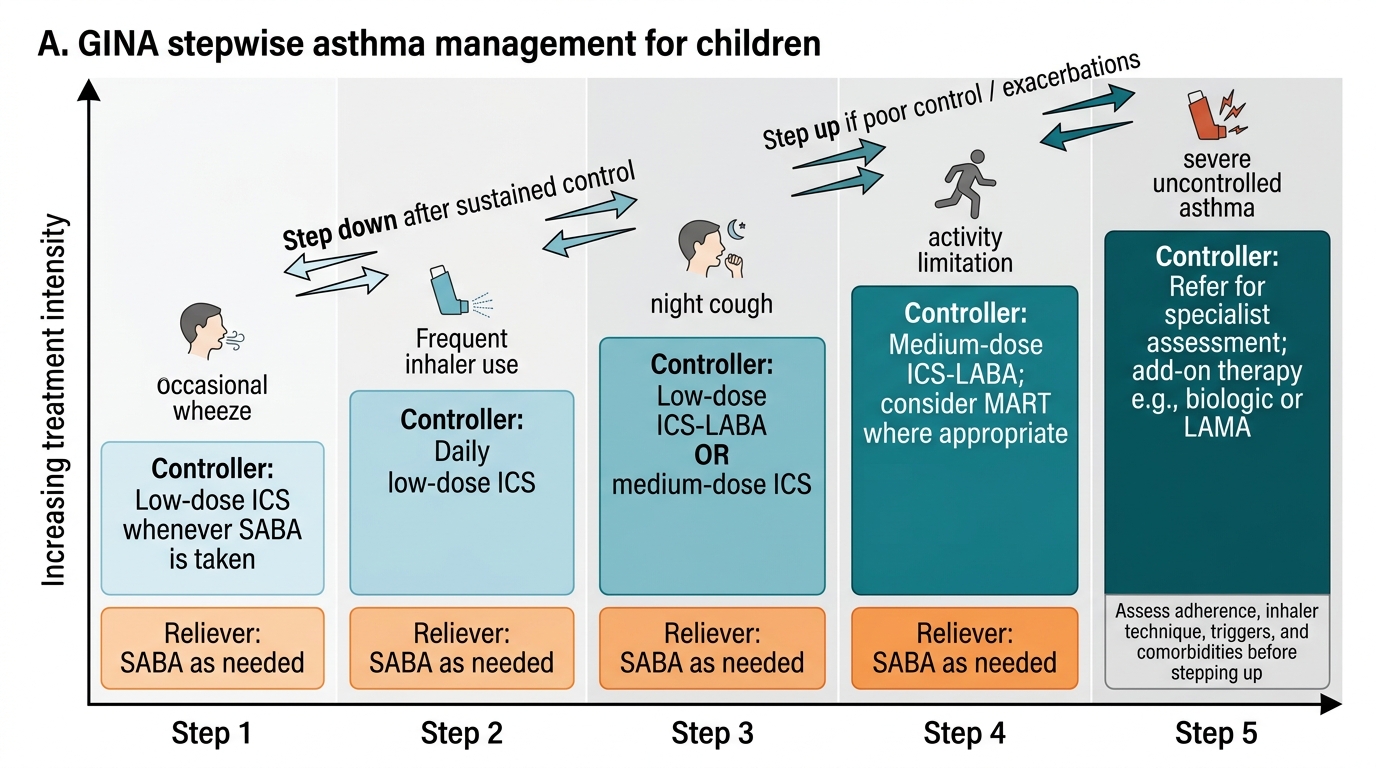
GINA Stepwise Asthma Management in Children
SELF-CHECK
In a child with severe acute asthma (SpO₂ 89%, PEFR 35%), after 60 minutes of oxygen, salbutamol × 3 doses, ipratropium × 3 doses, and IV hydrocortisone, the child remains in moderate-severe bronchospasm. What is the most appropriate next add-on?
A. Oral prednisolone — the IV route is unnecessary at this stage
B. Repeat high-dose salbutamol nebulisation every 5 minutes continuously
C. IV magnesium sulphate 25–75 mg/kg over 20 minutes
D. Immediate intubation and mechanical ventilation
Reveal Answer
Answer: C. IV magnesium sulphate 25–75 mg/kg over 20 minutes
IV magnesium sulphate (25–75 mg/kg, maximum 2.5 g, over 20 minutes) is the evidence-based add-on for severe acute asthma not responding to initial SABA + SAMA + systemic corticosteroids within 1 hour. It acts as a smooth-muscle relaxant by blocking calcium-mediated bronchospasm. Option A is incorrect: IV hydrocortisone is appropriate in severe exacerbation when oral route is unavailable or insufficient; switching to oral at this point would reduce bioavailability in a severe case. Option B is incorrect: continuous salbutamol at >1 nebulisation per 20 minutes risks tachycardia and hypokalaemia without additional bronchodilation benefit at this stage. Option D is incorrect: intubation in asthma carries high risk (barotrauma, dynamic hyperinflation) and should be a last resort; magnesium sulphate should be tried before escalating to ventilation.