Page 1 of 20
PE30.1-2 | Hypothyroidism — SDL Guide
Learning Objectives
- Describe the aetiology of congenital and acquired hypothyroidism in children
- Enumerate the clinical features of hypothyroidism in neonates and older children
- Explain the rationale and interpretation of neonatal thyroid screening (heel-prick TSH)
- Outline the management of hypothyroidism including weight-based levothyroxine dosing and monitoring targets
INSTRUCTIONS
Hypothyroidism is the single most common preventable cause of intellectual disability worldwide. In India, congenital hypothyroidism occurs in approximately 1 in 1000–2000 live births, and without early detection and treatment, the child sustains irreversible cognitive damage. This module equips you to recognise subtle neonatal signs, interpret the newborn thyroid screening report, and initiate timely levothyroxine — skills that will directly impact patient outcomes when you practice.
References
- Ghai Essential Pediatrics, 9th edition, Ch 17 (Endocrinology) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 581 (Hypothyroidism) (textbook)
- IAP Guidelines on Neonatal Thyroid Screening, 2019 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 6-week-old infant is brought to your OPD for a routine vaccination visit. The mother mentions the baby has been 'very quiet' and sleeps most of the day. On examination you notice the anterior fontanelle is large, the tongue appears slightly large, the skin is dry and mottled, and the baby has a protuberant abdomen with an umbilical hernia. The birth weight was 3.2 kg and the baby has gained only 300 g in six weeks. The hospital where the baby was born did not do a newborn screening. Your clinical alarm bells are ringing — could this baby have congenital hypothyroidism? Every day without treatment is narrowing this child's potential.
WHY THIS MATTERS
Congenital hypothyroidism is the most common preventable cause of intellectual disability. Thyroid hormone is essential for myelination of the central nervous system; deficiency in the first three years of life causes irreversible brain damage. Acquired hypothyroidism — most often Hashimoto's thyroiditis in older children — impairs growth, pubertal development, and school performance. India introduced universal newborn thyroid screening in many states, but gaps in coverage mean clinicians must recognise the clinical picture. Understanding how to screen, diagnose, and treat hypothyroidism transforms the outcome from a child with severe intellectual disability to one with normal development — a powerful argument for the importance of this competency.
RECALL
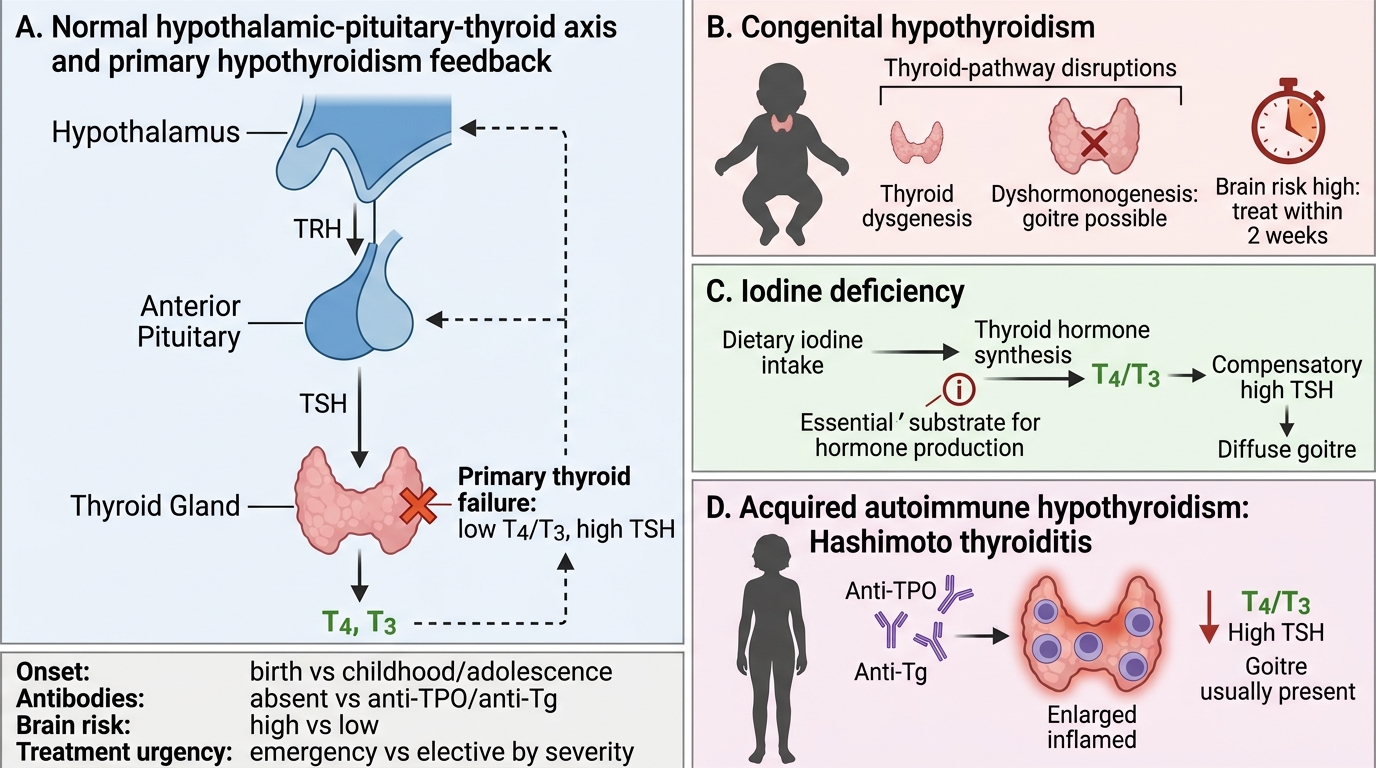
Before proceeding, recall these concepts from your basic sciences: Thyroid hormone synthesis involves iodine uptake by the follicular cell, organification (iodination of thyroglobulin), and coupling of iodotyrosines to form T3 and T4 — any defect in this cascade can cause dyshormonogenesis. The hypothalamic-pituitary-thyroid (HPT) axis operates by negative feedback: low T3/T4 → TRH release → TSH rise → thyroid stimulation. This is the basis for the screening test: in primary hypothyroidism TSH rises while T4 falls. Recall that T3 is the metabolically active form; T4 is converted to T3 peripherally. Thyroid hormone regulates basal metabolic rate, thermogenesis, cardiac output, bone turnover, and — critically in children — brain development and growth.
Clinical Presentation of Hypothyroidism in Children
The clinical presentation of hypothyroidism in children is dramatically different between neonates and older children, and this distinction reflects the developmental role of thyroid hormone. In the neonatal period, the signs are often subtle because maternal T4 crosses the placenta and provides partial protection for several weeks. The classic features of congenital hypothyroidism include prolonged neonatal jaundice (beyond the physiological 2 weeks), large posterior fontanelle (>0.5 cm at birth), macroglossia (large tongue), hoarse cry, hypotonia, constipation, poor feeding, mottled or cool dry skin, periorbital puffiness, abdominal distension, and umbilical hernia. The baby is often described as placid and a 'good' sleeper — deceptive signs that are actually symptoms of metabolic lethargy. Hypothermia and bradycardia may also be present. In contrast, acquired hypothyroidism in older children (most commonly Hashimoto's thyroiditis) presents with a slowing of linear growth (short stature, weight gain disproportionate to height), delayed bone age, constipation, cold intolerance, dry skin and hair, bradycardia, delayed deep tendon reflexes, and deterioration in school performance. A goitre is a hallmark of Hashimoto's thyroiditis and endemic iodine-deficiency goitre. Central (secondary/tertiary) hypothyroidism — from pituitary or hypothalamic disease — is rare and may lack the TSH elevation that characterises primary hypothyroidism.
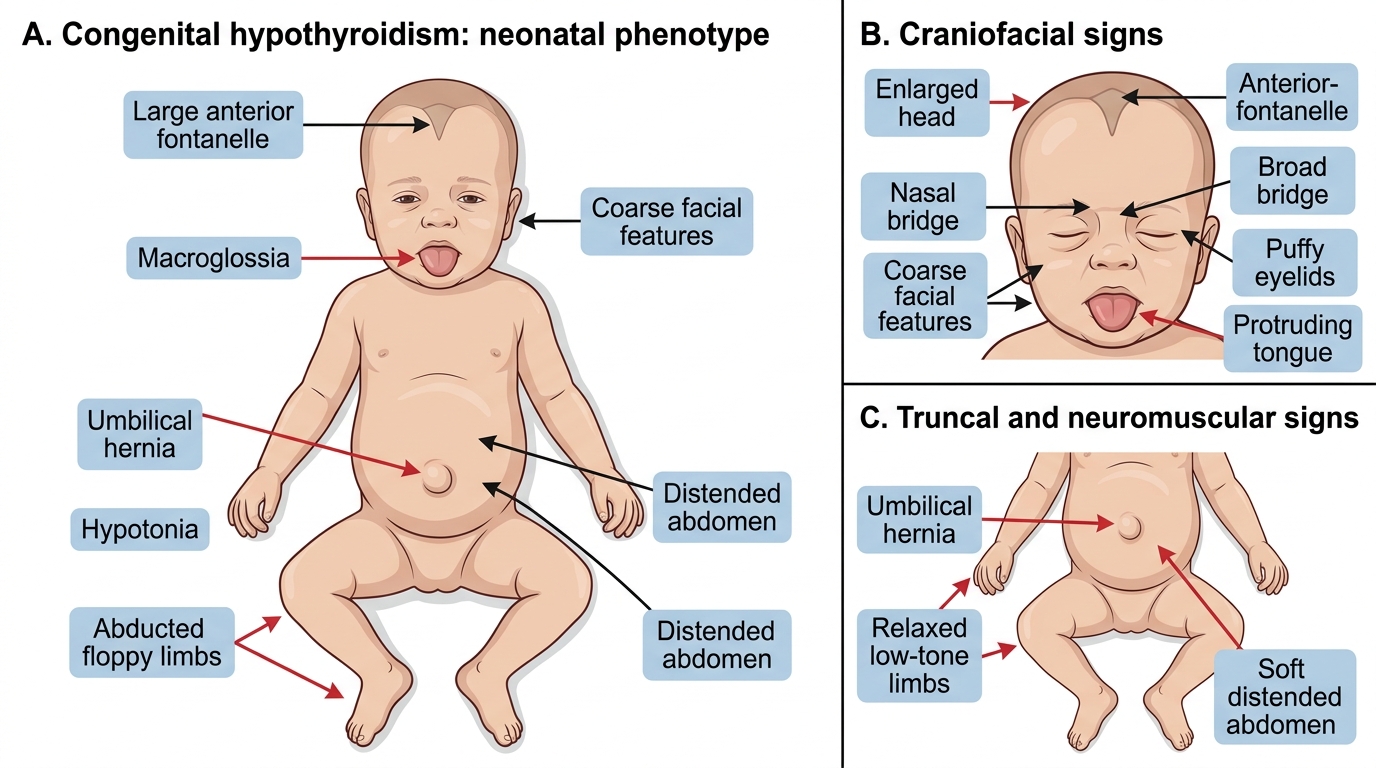
Neonatal Features of Congenital Hypothyroidism
Key clinical points: Growth charts are essential — a child with hypothyroidism will show velocity falling off across centile lines over months. Bone age on wrist X-ray is delayed. Absence of a goitre does NOT exclude hypothyroidism (thyroid dysgenesis has no goitre).
Pathophysiology and Aetiology
The aetiology of hypothyroidism in children divides cleanly into congenital and acquired causes, each with a distinct pathophysiological mechanism. Congenital hypothyroidism (CH) occurs in approximately 1 in 1000–2000 live births in India and accounts for the majority of permanent hypothyroidism. Thyroid dysgenesis — aplasia, hypoplasia, or ectopia of the thyroid gland — is responsible for approximately 85% of permanent CH. The gland either fails to develop, is too small to produce adequate hormone, or descends abnormally (ectopic, e.g. lingual thyroid). Dyshormonogenesis (10–15%) involves a structurally normal or enlarged gland with an enzymatic defect in one of the steps of thyroid hormone synthesis (NIS transporter, thyroid peroxidase, thyroglobulin). These children typically have a goitre because TSH continuously stimulates a gland that cannot produce hormone. Maternal iodine deficiency during pregnancy causes endemic cretinism in iodine-deficient regions — neurological cretinism features irreversible brain damage with normal or near-normal thyroid function at birth (the most severe and irreversible form). TSH receptor defects (loss-of-function mutations) cause a small, unresponsive gland. Transient CH can result from maternal antithyroid drugs (propylthiouracil, methimazole), maternal TSH-receptor-blocking antibodies, or iodine excess (neonatal iodine exposure from betadine, contrast agents).
Acquired hypothyroidism in children is most commonly Hashimoto's thyroiditis (autoimmune lymphocytic thyroiditis): T-cell-mediated destruction of follicular cells with anti-TPO and anti-thyroglobulin antibodies. It is commoner in girls, peaks in adolescence, and is associated with Down syndrome, Turner syndrome, and type 1 diabetes. Iodine deficiency remains a public health problem in some Indian districts — the thyroid enlarges (goitre) in compensation. Iatrogenic causes include post-thyroidectomy, post-radioiodine treatment, and long-term amiodarone/lithium use.
Hypothyroid Pituitary-Thyroid Axis Disruption Pathways
| Feature | Congenital | Acquired (Hashimoto's) |
|---|---|---|
| Onset | Birth (symptoms within weeks) | Childhood/adolescence |
| Goitre | Only in dyshormonogenesis | Usually present |
| Antibodies | Not typically | Anti-TPO, anti-Tg |
| Brain risk | High (irreversible if untreated early) | Low (brain mature) |
| Treatment urgency | EMERGENCY — start within 2 weeks | Elective, based on severity |
SELF-CHECK
A 4-week-old baby is found to have a TSH of 45 mU/L and fT4 of 5 pmol/L on neonatal screening. Which of the following best describes the immediate next step?
A. Repeat the test at 3 months of age to confirm
B. Start levothyroxine immediately at 10–15 mcg/kg/day and refer to a paediatric endocrinologist
C. Order a thyroid ultrasound before starting any treatment
D. Monitor clinically without treatment as maternal T4 will compensate
Reveal Answer
Answer: B. Start levothyroxine immediately at 10–15 mcg/kg/day and refer to a paediatric endocrinologist
A TSH of 45 mU/L with low fT4 confirms congenital hypothyroidism. Treatment with levothyroxine must begin immediately — within 2 weeks of birth ideally and certainly not delayed for imaging or repeat testing. Every day of untreated hypothyroidism risks irreversible neurological damage. Imaging (ultrasound, thyroid scan) is done after treatment is started to determine the aetiology, not before. Maternal T4 is insufficient to protect the brain once postnatal demand rises.
Diagnosis and Investigations — Including Newborn Screening
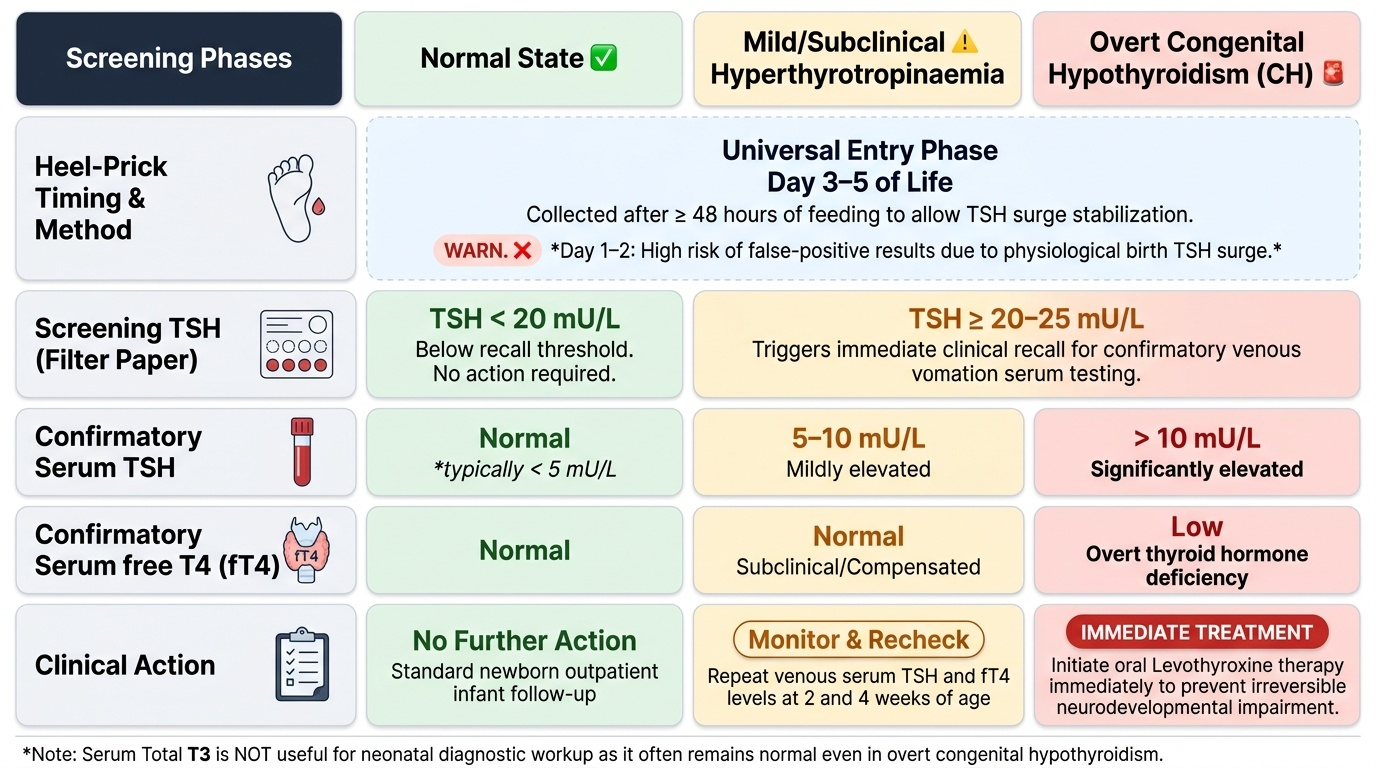
The cornerstone of early detection is the newborn thyroid screening programme, which detects CH before clinical signs develop — typically before any irreversible brain damage has occurred. In India, the IAP and several state governments recommend universal newborn screening. The test is a heel-prick blood spot on filter paper, collected on day 3–5 of life (after at least 48 hours of feeding to allow TSH surge stabilisation). If collected too early (day 1–2), a physiological TSH surge immediately after birth may produce false-positive results. The filter-paper specimen is sent to the screening laboratory; a TSH above the laboratory's recall threshold (typically 20–25 mU/L, cut-off varies by programme) triggers a recall for confirmatory serum testing.
Provided image
The confirmatory diagnostic workup includes: (1) Serum TSH — elevated in primary hypothyroidism; (2) Serum free T4 (fT4) — low in overt hypothyroidism, normal in subclinical/compensated; (3) Serum total T3 is not useful in neonates (often normal even in overt CH). Interpreting the neonatal thyroid screen report: a recalled infant should have serum TSH and fT4 measured; TSH >10 mU/L with low fT4 = overt CH requiring immediate treatment; TSH 5–10 mU/L with normal fT4 = mild TSH elevation (subclinical or transient) — monitor and recheck at 2 and 4 weeks. In acquired hypothyroidism, additional investigations include anti-TPO antibodies (positive in Hashimoto's) and thyroid ultrasound (heterogeneous echogenicity in Hashimoto's; diffuse/nodular goitre). Bone age (wrist X-ray) shows delay proportional to duration of hypothyroidism. In confirmed CH, a technetium thyroid scan or ultrasound is done AFTER starting treatment to identify dysgenesis or ectopic gland.
Pitfall: Do not delay levothyroxine treatment while awaiting thyroid imaging in a biochemically confirmed neonate. Start treatment first; investigate aetiology later.