Page 2 of 20
PE30.1-2 | Hypothyroidism — SDL Guide (Part 2)
Management: Levothyroxine and Follow-up
The treatment of hypothyroidism in children is levothyroxine (L-T4) given orally, once daily — the same molecule as endogenous T4, which is peripherally deiodinated to the active T3. Levothyroxine has excellent bioavailability when given on an empty stomach (30 minutes before feeds); it should not be given with soy formula, calcium, or iron supplements, which impair absorption. The starting dose depends on age and weight — dosing is weight-based and critical to get right, as under-treatment impairs brain development and over-treatment causes tachycardia, bone loss, and craniosynostosis. The critical principle in paediatric thyroid replacement is that the dose per kilogram is highest in neonates and decreases progressively as the child grows, mirroring the declining metabolic and neurodevelopmental demand for thyroid hormone. Parents must understand that the tablet must be given daily — never skipped — and always separate from feeds that could impair absorption.
Dosing by age:
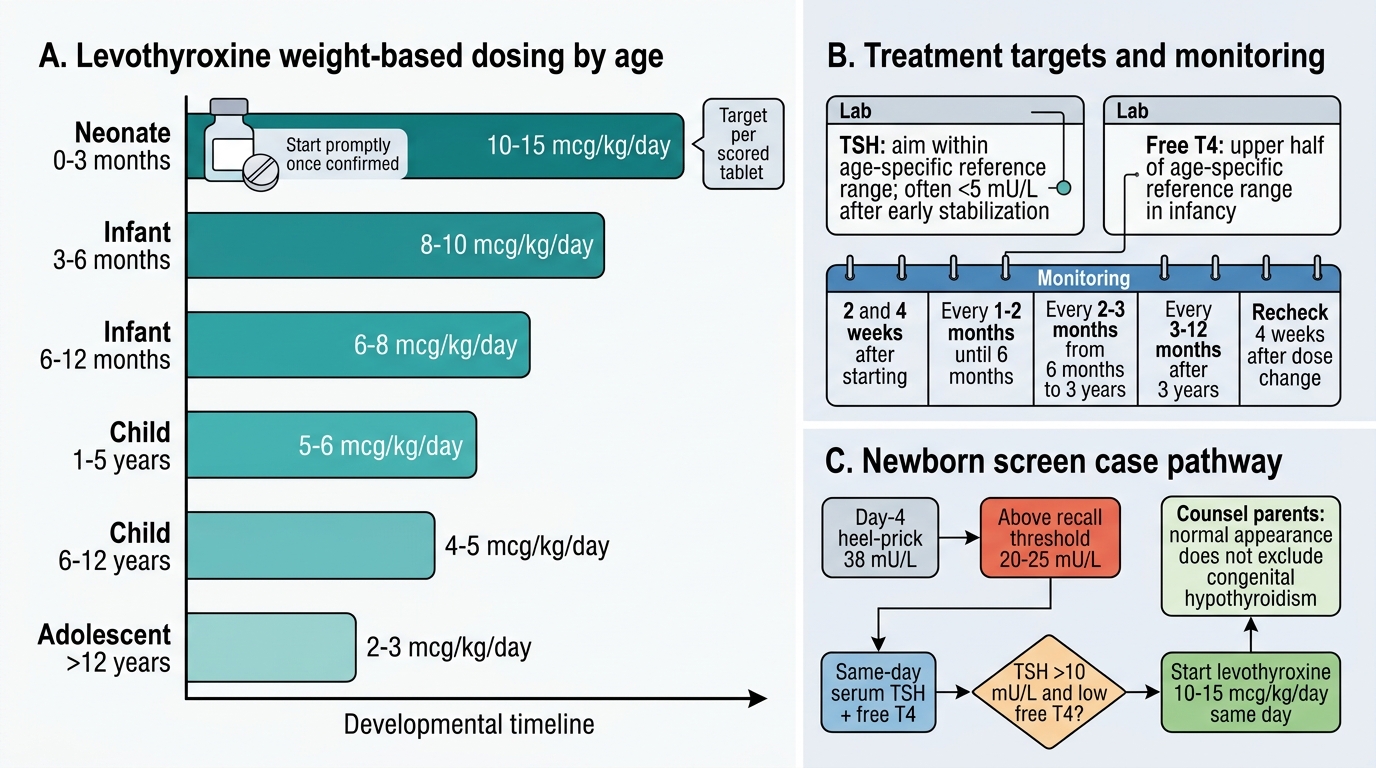
- Neonates (0–3 months): 10–15 mcg/kg/day — this higher dose in neonates reflects the high metabolic demand and brain-development urgency
- 3–6 months: 8–10 mcg/kg/day
- 6–12 months: 6–8 mcg/kg/day
- 1–5 years: 5–6 mcg/kg/day
- 6–12 years: 4–5 mcg/kg/day
- Adolescent: 2–3 mcg/kg/day
The practical approach is to start with a dose in the middle of the range for age and titrate by monitoring. Tablets can be crushed and dissolved in a small amount of breast milk or water (NOT soy or formula). Monitoring targets: Serum TSH should be maintained at 0.5–2.0 mU/L during the first three years of life in CH — a tighter target than for acquired hypothyroidism, because brain development is ongoing. fT4 should be in the upper half of the normal reference range for age. Follow-up schedule: every 2–4 weeks in the first 3 months, then every 2–3 months in the first year, and every 6 months thereafter. Bone age (wrist X-ray) at 1 year and annually monitors skeletal maturation. Neurodevelopmental assessment at 3, 12, and 24 months identifies any residual deficit early.
Prognosis is excellent when treatment begins within the first 2 weeks of life: IQ, height, and neurological outcome are normal. Delay beyond 1 month progressively worsens cognitive outcome. For acquired hypothyroidism, treatment is simpler — start levothyroxine, titrate to normal TSH and fT4, and the child's growth and performance recover fully.
For central (secondary) hypothyroidism, TSH is not the monitoring parameter (it may be low or normal). Dose is titrated to maintain fT4 in the normal range.
Levothyroxine Dosing and Monitoring in Congenital Hypothyroidism
Self-Assessment and Case Application
Now apply what you have learned. Consider the following case: A day-4 heel-prick filter-paper TSH comes back as 38 mU/L from the newborn screening lab. The baby appears clinically normal — no obvious signs yet. What is your interpretation and management plan? The following two cases illustrate how you move from a laboratory report to a clinical decision and a counselling conversation. In each case, identify the key biochemical features, determine the urgency of treatment, calculate an appropriate starting dose, and frame the communication with the family in plain language. Working through cases systematically — rather than jumping to a diagnosis — is the core skill of clinical paediatrics. Remember also that an apparently normal neonatal examination does not exclude congenital hypothyroidism — the classical features may take weeks to fully manifest, making biochemical screening the only reliable safety net.
Systematic approach:
• A TSH of 38 mU/L on a day-4 heel-prick, above the 20–25 mU/L recall threshold, mandates immediate confirmatory serum TSH and fT4 — do not wait.
• If confirmatory serum TSH is >10 mU/L and fT4 is low, this is overt congenital hypothyroidism requiring levothyroxine 10–15 mcg/kg/day to be started on the same day as confirmation, not deferred.
• Counsel the parents: 'The thyroid gland is not working well and your baby needs a daily tablet to replace the hormone. Starting today gives your child a fully normal brain and development — every day counts.'
• Arrange thyroid imaging (ultrasound ± scan) to identify the aetiology AFTER treatment has started.
• Refer to a paediatric endocrinologist for ongoing management, while commencing treatment immediately in primary care.
Second case — older child: A 9-year-old girl presents with weight gain, cold intolerance, dry skin, and constipation for 6 months. TSH = 12 mU/L, fT4 is low-normal. Anti-TPO antibodies are strongly positive. Diagnosis is Hashimoto's thyroiditis. Treatment: levothyroxine at 4–5 mcg/kg/day, titrate to normal TSH. Reassure parents: with treatment, her growth and energy will normalise over weeks to months.
CLINICAL PEARL
The two most important facts about congenital hypothyroidism:
1. Start treatment BEFORE imaging. A heel-prick TSH ≥20–25 mU/L confirmed on serum = begin levothyroxine today. Imaging tells you why the gland failed; it does not change the urgency of treatment.
2. Neonatal dose is 10–15 mcg/kg/day — higher per kg than in older children because brain myelination demands are maximal in the first three years of life. Treat aggressively early; taper dose with age.
Bonus: Absence of goitre does NOT exclude hypothyroidism — thyroid dysgenesis (85% of CH) has no goitre because there is no functioning gland to enlarge.