Page 7 of 32
PE31.3-4 | Tuberculosis Management Program — SDL Guide
Learning Objectives
- Describe the NTEP treatment regimens for drug-sensitive childhood TB including weight-band daily fixed-dose combinations
- Explain the rationale for directly observed therapy (DOT) and the two-phase treatment structure
- Describe the preventive strategies for childhood TB including BCG vaccination and isoniazid preventive therapy
- Explain the objectives, key components, and outcome indicators of the National Tuberculosis Elimination Programme (NTEP)
- Distinguish current NTEP daily FDC regimens from the obsolete intermittent regimens
INSTRUCTIONS
Tuberculosis cannot be cured by prescribing drugs alone — it requires a structured programme approach to ensure adherence, prevent drug resistance, and break transmission chains in communities. India's National Tuberculosis Elimination Programme (NTEP, formerly RNTCP) is the backbone of this effort, providing free diagnosis, free daily fixed-dose combination treatment, and directly observed therapy to every patient in India. For paediatric TB specifically, NTEP provides weight-band FDC formulations designed for children. This module covers both the clinical treatment regimen and the programmatic framework — understanding both is essential because a drug prescribed without DOT supervision is likely to produce drug-resistant TB, which is far harder and costlier to treat.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 10 — Tuberculosis (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 254 — Tuberculosis (textbook)
- NTEP (National Tuberculosis Elimination Programme) — Standards for TB Care in India (STCI), 2022 (guideline)
- NTEP Paediatric TB Module, 2022 (guideline)
- IAP Consensus Statement on Childhood Tuberculosis, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A health worker at a district TB unit asks you: 'Doctor, the mother of a 5-year-old with TB says she is giving the tablets at home every day, but the child is no better at 2 months. The sputum culture is still positive. What do we do?' You review the case and find: the child was prescribed the correct drugs but the mother was not enrolled in DOT; she has been giving half the tablets to save them for the younger sibling; and no one checked the weight at enrolment, so the dose was under-calculated. This case — missed DOT, incorrect dosing, inadequate follow-up — illustrates exactly why TB management cannot be individualised drug therapy but must be delivered as a structured programme.
WHY THIS MATTERS
India has the world's highest TB burden, with approximately 2.8 million notified cases annually. The creation of multidrug-resistant TB (MDR-TB) is almost entirely a human-made disaster — it results from incomplete, irregular, or incorrectly dosed treatment. Every MDR-TB case in India represents a treatment failure of the drug-sensitive programme, requiring second-line drugs that are more toxic, more expensive, and require 18–24 months rather than 6 months of treatment. Paediatric TB, if treated correctly and completely, is almost always curable with first-line drugs. The gap between this potential and actual outcomes is determined by programme implementation — by whether DOT is used, whether doses are weight-adjusted, and whether contacts are screened and protected. This module gives you the knowledge to apply the NTEP programme correctly every time.
RECALL
Activate the following prior knowledge:
• M. tuberculosis requires prolonged treatment because a subpopulation of organisms ('persisters') are metabolically quiescent and not killed by short-course therapy — they need months of bactericidal exposure; recall from Microbiology/Pharmacology.
• TB drugs and mechanisms: Isoniazid (H) — bactericidal, inhibits mycolic acid synthesis; Rifampicin (R) — bactericidal, inhibits RNA polymerase; Pyrazinamide (Z) — bactericidal in acidic environment (kills intracellular persisters); Ethambutol (E) — bacteriostatic, inhibits arabinosyl transferase.
• TB clinical spectrum and diagnosis — reviewed in pe24-tb-clinical and pe24-tb-diagnosis SDLs.
• BCG vaccine — given at birth (NIS), protects ~80% against miliary TB and TBM in infants.
• Drug-resistant TB — MDR-TB = resistant to at least isoniazid AND rifampicin; the commonest cause is irregular treatment.
Orientation: Why TB Management Requires a Programme, Not Just a Drug
The biology of Mycobacterium tuberculosis makes it uniquely difficult to treat with a short course of a single drug. Unlike most bacteria that can be eradicated in 5–7 days, tuberculosis requires a minimum of 6 months of multi-drug therapy because of the existence of multiple bacterial sub-populations within a lesion. The rapidly dividing organisms in cavities are killed within the first 2 months by the bactericidal drugs isoniazid and rifampicin. However, a second population — dormant 'persister' organisms — survive inside caseous material and macrophages, protected from drugs by low metabolic activity. Pyrazinamide is uniquely active against these intracellular persisters in the acidic environment of macrophage phagosomes, which is why it is included in the first 2 months. Rifampicin in the continuation phase prevents relapse from the slowly reviving persister population over the subsequent 4 months. This understanding — that different drugs target different sub-populations at different phases — is the pharmacological rationale for the two-phase regimen.
The second biological reality is that M. tuberculosis mutates spontaneously, producing drug-resistant organisms at a rate of approximately 1 in 10⁶–10⁸ divisions for each drug. In any large bacterial population, a few pre-existing resistant mutants are always present. When a single drug is used, these resistant mutants survive and multiply — producing a drug-resistant strain within weeks. Using multiple drugs simultaneously (at least 4 in the intensive phase) ensures that the probability of a bacillus being resistant to all four drugs simultaneously is astronomically low (10⁻²⁴ to 10⁻³²). This is the pharmacological rationale for combination therapy and is why monotherapy for TB is absolutely contraindicated.
The third reality is adherence. Even a correctly prescribed regimen fails if doses are missed, taken irregularly, or stopped prematurely. A patient who discontinues treatment after 2 months because symptoms have improved has not been cured — the persister population has survived and will relapse with potentially drug-resistant organisms. Directly Observed Therapy (DOT) — having a designated health worker or community volunteer physically watch the patient swallow every dose — is the operational solution to this adherence problem. DOT is the single most important programme component that separates a well-functioning TB programme from one that generates MDR-TB.
NTEP Treatment Regimens for Drug-Sensitive TB
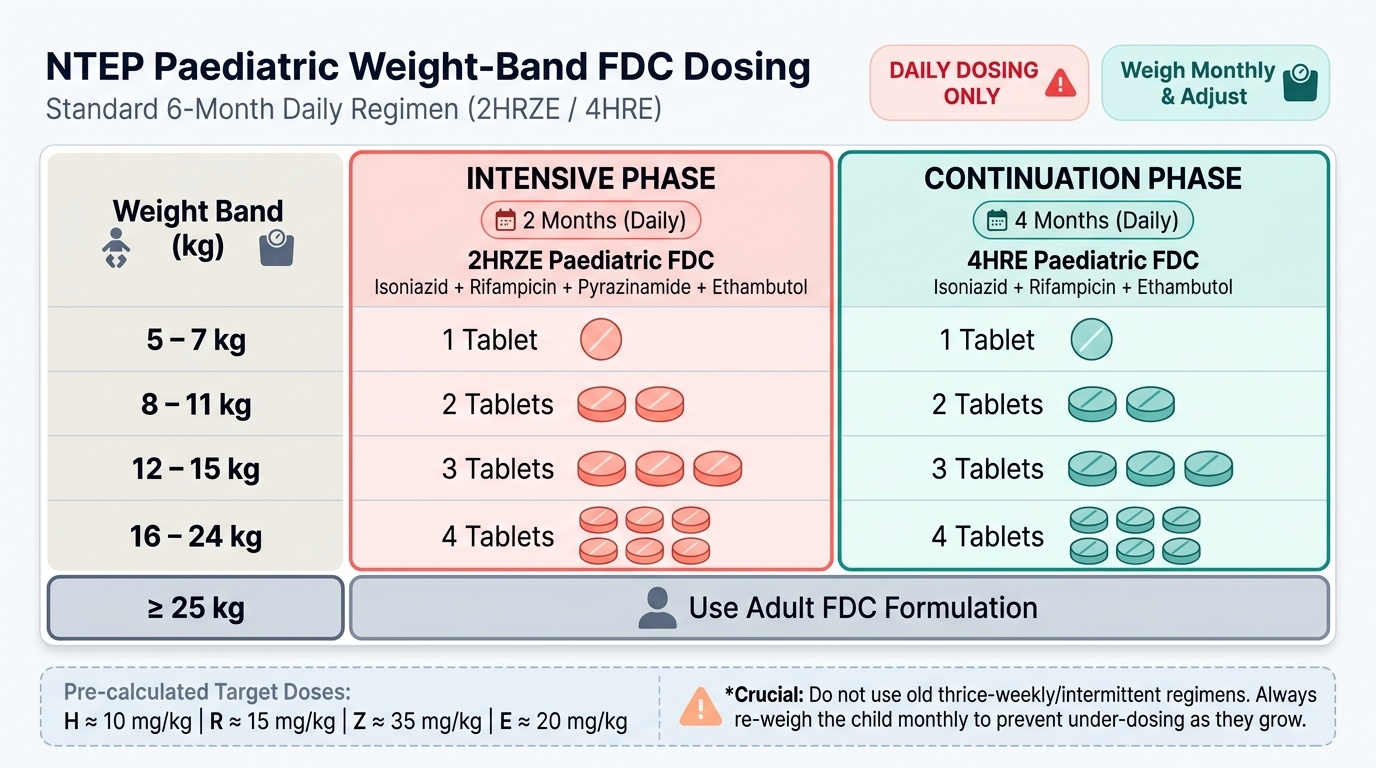
The National Tuberculosis Elimination Programme (NTEP) prescribes all TB treatment using weight-band daily fixed-dose combinations (FDCs). A fixed-dose combination tablet is a single formulation that contains a predetermined ratio of all the required drugs, ensuring that the correct proportions are always delivered simultaneously — this is critical because taking drugs separately increases the risk that a patient will selectively stop one drug while continuing others, a pattern that reliably generates drug resistance. For children, a specific paediatric FDC formulation is provided with lower drug concentrations, and doses are calculated by the child's current weight, not by age, because a fixed age-based dose would under-dose a heavier child and over-dose a lighter one.
Provided image
Standard drug-sensitive TB regimen: The regimen is written in abbreviated form as 2HRZE / 4HRE:
• Intensive phase (2 months): Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) — daily
• Continuation phase (4 months): Isoniazid (H) + Rifampicin (R) + Ethambutol (E) — daily
• Total duration: 6 months for drug-sensitive pulmonary TB
• Extended regimens: TBM and osteoarticular TB — 12 months total (2HRZE + 10HRE); miliary TB — 9–12 months
CRITICAL: The thrice-weekly intermittent regimen (previously used under RNTCP) is NO longer the current NTEP standard. The current NTEP standard is DAILY dosing — not three times a week. This distinction is high-yield for examinations and clinically critical — citing the old intermittent regimen is a factual error.
Paediatric FDC weight-band dosing (NTEP 2022):
| Weight Band | Intensive Phase (HRZE tablets/day) | Continuation Phase (HRE tablets/day) |
|---|---|---|
| 5–7 kg | 1 tablet | 1 tablet |
| 8–11 kg | 2 tablets | 2 tablets |
| 12–15 kg | 3 tablets | 3 tablets |
| 16–24 kg | 4 tablets | 4 tablets |
| ≥25 kg | Use adult FDC (adult weight-band) |
Doses are mg/kg: H ~10 mg/kg, R ~15 mg/kg, Z ~35 mg/kg, E ~20 mg/kg — the FDC is pre-calculated to deliver these targets. Always re-weigh the child monthly and adjust the weight band as the child gains weight during treatment (under-dosing in a growing child risks treatment failure).
Drug-resistant TB (DR-TB): Any CBNAAT showing rifampicin resistance, or a culture-confirmed MDR/XDR TB isolate, requires referral to a NTEP DR-TB centre for the appropriate standardised second-line regimen. First-line 2HRZE/4HRE must NOT be used for MDR-TB. Second-line drugs include bedaquiline, linezolid, fluoroquinolones — under NTEP supervision.
SELF-CHECK
A 4-year-old child with drug-sensitive pulmonary TB weighs 13 kg. According to NTEP paediatric FDC weight-band dosing, what is the correct number of paediatric FDC tablets daily in the intensive phase?
A. 1 tablet (5–7 kg band)
B. 2 tablets (8–11 kg band)
C. 3 tablets (12–15 kg band)
D. 4 tablets (16–24 kg band)
Reveal Answer
Answer: C. 3 tablets (12–15 kg band)
A child weighing 13 kg falls in the 12–15 kg weight band, which requires 3 paediatric FDC tablets daily in the intensive phase (HRZE). Weight-band dosing must be based on current weight, not age. This delivers approximately H 10 mg/kg, R 15 mg/kg, Z 35 mg/kg, E 20 mg/kg — within the therapeutic range. The child should be re-weighed monthly and the weight band updated if there is significant weight gain during treatment.
The NTEP Programme Structure and DOTS
The National Tuberculosis Elimination Programme (NTEP) — formerly the Revised National TB Control Programme (RNTCP, 1997–2020) — is India's government programme for TB prevention, diagnosis, treatment, and elimination. The programme is implemented through a network of Designated Microscopy Centres (DMC), CBNAAT testing sites, and Treatment Units (TU) at district level. Every TB patient in India is registered, diagnosed, and treated free of charge through this network. The programme was renamed from RNTCP to NTEP in 2020 to reflect India's declared national goal of achieving TB elimination (fewer than 1 case per million population) by 2025 — an extraordinarily ambitious target given the current burden, but one that has fundamentally reshaped all current policy, diagnostic tools, treatment regimens, and programme design priorities.
Key NTEP programme components:
• Case finding: Systematic identification of presumptive TB cases at health facilities + active case finding in high-risk communities (mining, prisons, migrant populations)
• Diagnosis: CBNAAT as first-line rapid test (replacing AFB smear as the initial test at TU level); drug susceptibility testing (DST) for all cases
• Notification: All TB cases (public AND private sector) must be notified to NTEP through the Nikshay portal (India's online TB notification and monitoring system) — mandatory since 2012, reinforced by legal provisions
• Directly Observed Therapy (DOT): A designated DOT provider (health worker, ASHA, community volunteer) watches the patient swallow every dose; the cornerstone of treatment adherence; evidence shows it doubles treatment success rates compared to self-administration
• Follow-up monitoring: Sputum smear/culture at 2 months (intensive phase completion) to confirm treatment response; end-of-treatment culture for confirmation of cure
• Contact tracing: All household contacts of a smear-positive case must be screened; children <5 years who are contacts receive priority evaluation
• Nutritional support (Nikshay Poshan Yojana): DBT payment of ₹500/month to TB patients during treatment to offset nutritional impact — this recognises malnutrition as both a cause and consequence of TB
Treatment outcomes (NTEP definitions):
• Cured: Smear-negative at end of treatment (pulmonary TB)
• Treatment completed: Finished full course without smear evidence (non-pulmonary or unavailable)
• Treatment failed: Smear/culture positive at 5 months or later
• Lost to follow-up: Interrupted treatment ≥2 consecutive months
• Not evaluated / Died
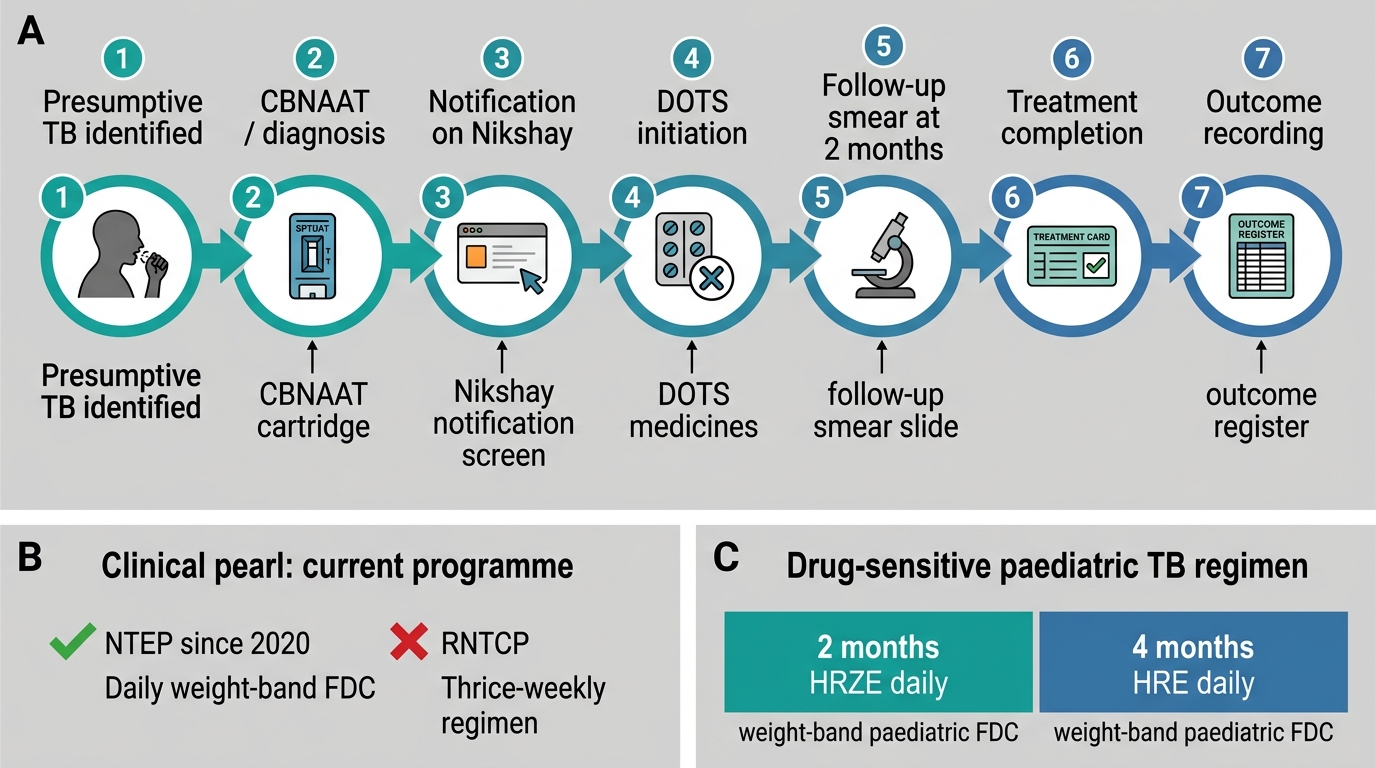
NTEP Patient Pathway for Tuberculosis
CLINICAL PEARL
RNTCP is dead — use NTEP and DAILY dosing. A common examination error and clinical error is citing the Revised National Tuberculosis Control Programme (RNTCP) as the current programme, or prescribing thrice-weekly intermittent therapy. RNTCP was replaced by NTEP in 2020, and the new programme uses DAILY weight-band FDC — not the old thrice-weekly (3×/week) regimen. This shift was driven by evidence that daily therapy has higher cure rates and lower rates of acquired drug resistance than the intermittent regimen. If you write 'RNTCP' or 'thrice weekly' in an examination, expect to lose marks; if you prescribe it in clinical practice, you risk treatment failure and drug-resistant TB.
SELF-CHECK
Under the current NTEP policy, which of the following represents the correct treatment regimen for a 7-year-old child with drug-sensitive pulmonary TB?
A. 2 months HRZE daily + 4 months HR daily (no ethambutol in continuation phase)
B. 2 months HRZE thrice-weekly + 4 months HR thrice-weekly
C. 2 months HRZE daily + 4 months HRE daily using weight-band paediatric FDC
D. 6 months HRZE daily (no continuation phase)
Reveal Answer
Answer: C. 2 months HRZE daily + 4 months HRE daily using weight-band paediatric FDC
The current NTEP standard regimen for drug-sensitive paediatric TB is 2HRZE (intensive phase, 2 months, daily) followed by 4HRE (continuation phase, 4 months, daily) — a total of 6 months, using weight-band paediatric FDC. Ethambutol is included in the continuation phase in the current Indian paediatric regimen (unlike some international guidelines that use only HRE without ethambutol — the NTEP includes E throughout). The thrice-weekly regimen (Option B) is the obsolete RNTCP regimen and must NOT be prescribed. Option A omits ethambutol from the continuation phase, which is incorrect per current NTEP paediatric guidelines.