Page 8 of 32
PE31.3-4 | Tuberculosis Management Program — SDL Guide (Part 2)
Preventive Strategies: BCG, IPT, and Infection Control
Prevention of tuberculosis in children operates at three levels: universal vaccination to reduce severity of disease in the community, chemoprophylaxis to prevent progression from infection to active disease in high-risk individuals, and infection control to reduce transmission in households and healthcare settings. Understanding all three levels is essential for the clinician who manages not just the index case but the household ecosystem around that case.
1. BCG vaccination (primary prevention):
Bacille Calmette-Guérin (BCG) is a live attenuated strain of Mycobacterium bovis given as a single intradermal injection at birth under the Indian National Immunization Schedule (NIS). BCG is the first vaccine in the NIS — given on the day of birth, along with OPV-0 and Hepatitis B. The site is the left deltoid; a local ulcer forms and heals to leave the characteristic depressed scar at 4–6 weeks.
BCG's protection is primarily against the severe disseminated forms of childhood TB — it reduces the risk of miliary TB by ~80% and TB meningitis by ~70–80% in vaccinated infants. However, it does not reliably prevent pulmonary TB in adolescents and adults, and its protective effect wanes over years. This is why BCG-vaccinated adults can still develop pulmonary TB, but BCG-vaccinated infants are protected from the most lethal complications.
2. Isoniazid Preventive Therapy (IPT) — chemoprophylaxis:
IPT is the administration of isoniazid (INH) for 6 months to a child who has been infected (positive TST) but has no active disease (LTBI) — to prevent progression to active TB. NTEP and IAP indications:
• All children <5 years who are household contacts of a smear-positive pulmonary TB case, regardless of TST result (because TST may be negative at this age)
• Children of any age with HIV infection who are household contacts of TB
• Children with positive TST (≥10 mm standard; ≥5 mm immunocompromised) and no active disease — regardless of age
IPT dose: Isoniazid 10 mg/kg/day (max 300 mg/day) for 6 months. Active TB must be excluded before starting IPT by CXR and symptom screen — IPT given to a child with active TB is effectively monotherapy and will generate INH resistance.
3. Infection control in households:
The household of a smear-positive TB case is the highest-risk environment for child contacts. Key measures:
• Cough hygiene — cover mouth when coughing; avoid shared sleeping spaces when possible
• Ventilation — open windows to reduce airborne bacillary concentration
• Nutritional support — treat malnutrition in child contacts concurrently; SAM children are at highest risk of progression
• HIV testing — all TB contacts should be offered HIV counselling and testing; HIV-positive contacts need ART and intensive TB monitoring
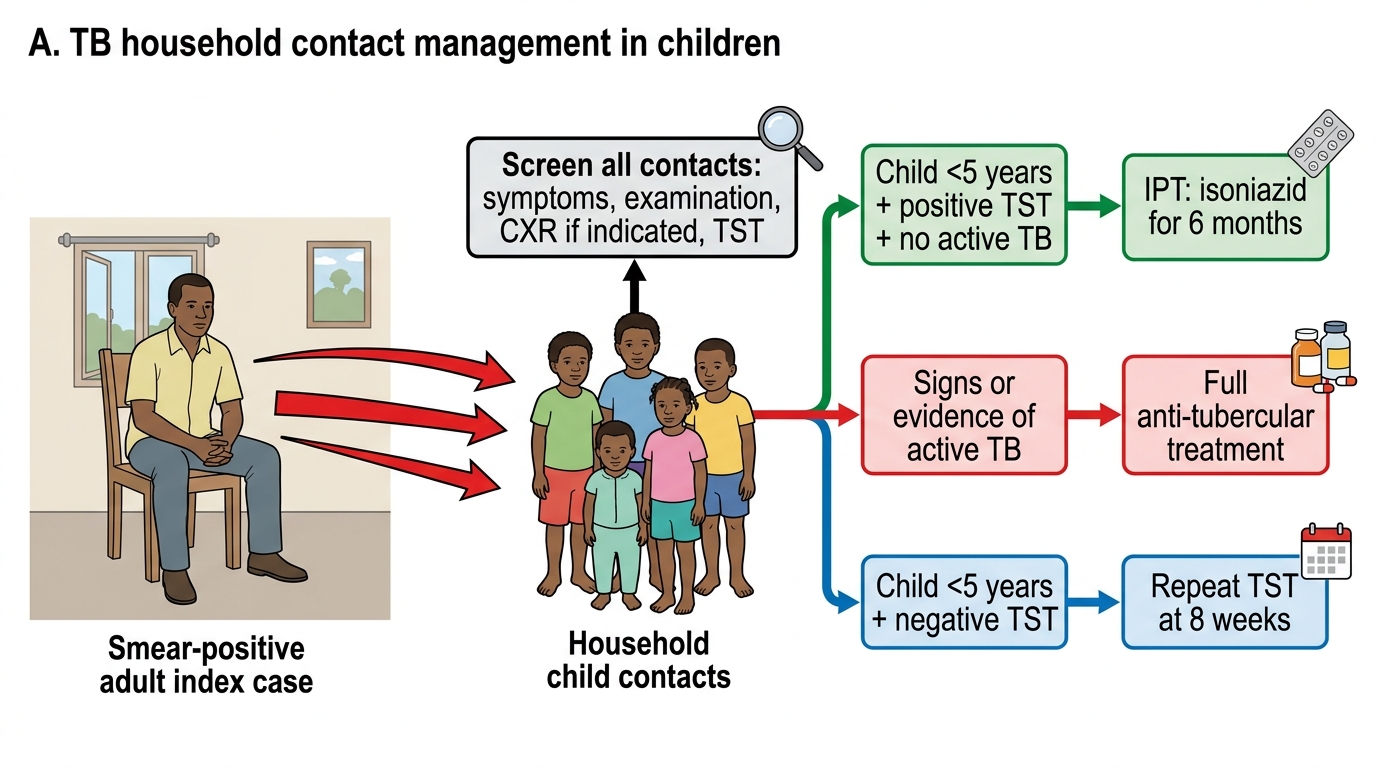
TB Household Contact Management in Children
SELF-CHECK
A 3-year-old child who is a household contact of a smear-positive pulmonary TB case has a Mantoux TST of 4 mm and a normal chest X-ray. According to NTEP/IAP guidelines, the MOST appropriate management is:
A. No treatment — TST is negative, so there is no infection
B. Start full TB treatment (2HRZE/4HRE) empirically
C. Give IPT (isoniazid 10 mg/kg/day for 6 months) regardless of TST result, as child is <5 years
D. Repeat the Mantoux test in 8 weeks only; no prophylaxis needed now
Reveal Answer
Answer: C. Give IPT (isoniazid 10 mg/kg/day for 6 months) regardless of TST result, as child is <5 years
For children <5 years who are household contacts of a smear-positive TB case, NTEP/IAP recommend IPT regardless of TST result. At this age, cell-mediated immunity is immature, TST may be falsely negative, and the risk of rapid progression to miliary TB or TBM is highest. Active TB must first be excluded (CXR normal, asymptomatic — done here). IPT is then given for 6 months at 10 mg/kg/day. Option A is incorrect because a negative TST in a child under 5 with known contact does not exclude infection. Option D is reasonable for children >5 years with negative TST but not for this high-risk <5 year group.
Self-Assessment
The following self-assessment questions integrate the TB management and prevention content from this module. They are designed to test knowledge of NTEP regimens, programmatic principles, and preventive strategies — covering PE31.3 (management regimens) and PE31.4 (preventive strategies and programme objectives). Each question demands application of the specific NTEP weight-band dosing framework and the current NTEP versus obsolete RNTCP distinction — a distinction that separates modern, evidence-based TB practice from outdated prescribing. Work through each question systematically: state your answer, give the NTEP/IAP source or rationale, consider potential examination traps such as the thrice-weekly vs daily distinction, and remember that mastery of the programme components — DOT supervision, Nikshay notification, and systematic contact screening — is equally as important for real-world practice as knowing the individual drug names and their correct doses.
- Write out the full 6-month NTEP treatment regimen for a 6-year-old child (weight 18 kg) with drug-sensitive pulmonary TB. Name the drugs, phases, duration of each phase, dosing frequency, and number of paediatric FDC tablets per day.
- What is the difference between the current NTEP regimen and the old RNTCP regimen? Why was the change made from thrice-weekly to daily dosing?
- A smear-positive mother with TB has three children: a 2-year-old, a 5-year-old, and a 9-year-old. For each child, outline the screening and preventive management steps per NTEP/IAP guidelines.
- Explain the rationale for including four drugs (HRZE) in the intensive phase but only three (HRE) in the continuation phase. What happens biologically in each phase?
- What are the NTEP indicators used to measure programme performance? What treatment success rate is targeted, and what does 'lost to follow-up' mean programmatically?