Page 1 of 14
PE14.1 | Kerosene Ingestion — SDL Guide
Learning Objectives
- Identify the risk factors and epidemiological context of childhood kerosene ingestion in India
- Explain the pathophysiology of aspiration chemical pneumonitis as the primary mechanism of toxicity
- Recognise the clinical features of kerosene ingestion affecting respiratory, GI, and central nervous systems
- Interpret relevant investigations including chest X-ray findings and oxygen saturation monitoring
- Apply the correct management approach — including knowing which interventions are CONTRAINDICATED (emesis, gastric lavage)
- Counsel families on storage safety and accidental poisoning prevention
INSTRUCTIONS
Kerosene ingestion is one of the most common accidental childhood poisonings in India, with unique and life-threatening management principles that differ from most other toxic ingestions. The central danger is not systemic absorption from the gut — it is aspiration into the airway during ingestion or vomiting, causing chemical pneumonitis. This module equips you to manage this emergency correctly, including recognising the critically important contraindications to gastric decontamination.
References
- Ghai Essential Pediatrics, 9th Edition — Chapter on Poisoning (textbook)
- Nelson Textbook of Pediatrics, 21st Edition — Chapter on Poisoning (textbook)
- IAP Guidelines on Management of Common Childhood Poisoning (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 2-year-old boy is brought to the emergency department by his mother. She reports that 30 minutes ago he was playing near the kitchen storeroom and she found him with an open container of kerosene — the family uses it for their cooking stove. He immediately coughed and choked, began crying, then vomited. He now has a persistent cough and appears restless. On examination his respiratory rate is 42/minute, there is subcostal recession, and his SpO2 is 94% on room air. His mother asks: 'Doctor, should we make him vomit to get the kerosene out?' — How do you respond, and what do you do next?
WHY THIS MATTERS
Accidental kerosene ingestion is the most common childhood poisoning in India, accounting for a substantial proportion of paediatric poisoning admissions. India's continued dependence on kerosene as a domestic fuel — for cooking stoves, lamps, and heating — means the substance is widely accessible in households, often stored in unlabelled bottles or food containers within reach of young children. The population at greatest risk is children aged 1–5 years, who are developmentally curious but lack the judgment to recognise hazardous substances. The unique danger of kerosene lies not in gut absorption but in aspiration: a well-intentioned but incorrect response — inducing vomiting or performing gastric lavage — can transform a mild ingestion into a life-threatening aspiration pneumonitis. As a future physician, you must be prepared to make this distinction instantly and act on it correctly.
RECALL
Before studying kerosene toxicity, recall these foundational concepts from Year 1:
- Respiratory anatomy: The larynx, trachea, and bronchial tree provide a continuous open airway in an alert person; the epiglottis and cough reflex protect it during swallowing. In a vomiting or sedated child, these protective reflexes are diminished.
- Surfactant physiology: Type II pneumocytes secrete pulmonary surfactant (primarily dipalmitoylphosphatidylcholine) to reduce alveolar surface tension and prevent collapse. Any agent that disrupts surfactant causes alveolar instability, atelectasis, and ventilation-perfusion mismatch.
- V/Q mismatch: When lung segments are perfused but not ventilated (as in consolidation or atelectasis), deoxygenated blood passes into the systemic circulation, causing hypoxaemia.
- Basic toxicology: Toxic substances may cause harm by local mucosal effects, systemic absorption, or aspiration into the airway. The route of harm determines the correct intervention — gastric decontamination is useful only when systemic absorption from the gut is the primary danger.
Clinical Presentation of Kerosene Ingestion
The clinical presentation of kerosene ingestion reflects the tissue surfaces it contacts — predominantly the oropharyngeal and tracheobronchial mucosa rather than the systemic circulation. The onset of symptoms is typically within minutes to 30 minutes of ingestion and directly reflects the child's degree of exposure and whether aspiration has occurred. Understanding the pattern of presentation across organ systems helps the clinician assess severity and guide monitoring intensity.
Respiratory symptoms are the most important and dangerous. Immediate coughing and choking are almost universal and represent the initial protective reflex against aspiration. Within minutes to hours, children may develop tachypnoea, increased work of breathing (subcostal, intercostal, or suprasternal recession), and wheeze or crepitations on auscultation. In severe cases, respiratory failure with cyanosis can develop. Importantly, symptoms may initially appear to improve after the acute phase, then worsen at 4–6 hours as the full inflammatory response to aspiration develops.
Gastrointestinal symptoms include burning sensation in the mouth and throat, nausea, and vomiting. The vomiting is of particular concern because it significantly increases the risk of aspiration — hydrocarbon-containing vomitus can be aspirated into the airway. Abdominal discomfort and diarrhoea may occur.
Central nervous system manifestations depend on the degree of systemic absorption and hypoxaemia. Mild cases show restlessness and irritability. In severe poisoning or when significant aspiration causes hypoxaemia, the child may develop drowsiness, altered consciousness, seizures, or coma.
Local effects include erythema and chemical burns of the lips, buccal mucosa, and oropharynx. If kerosene contacts the eyes or skin, it causes local irritation and chemical conjunctivitis or dermatitis.
| System | Features | Clinical Significance |
|---|---|---|
| Respiratory | Cough, choking, tachypnoea, wheeze, recession, cyanosis | Most dangerous — aspiration pneumonitis |
| GI | Burning mouth, vomiting, diarrhoea | Vomiting ↑ aspiration risk |
| CNS | Restlessness, drowsiness, seizures, coma | Reflects hypoxaemia or direct toxicity |
| Local | Oral mucosal erythema, chemical burns, eye/skin irritation | Direct contact injury |
Pathophysiology: Why Aspiration is the Central Danger
The pathophysiology of kerosene toxicity is determined primarily by the physicochemical properties of hydrocarbons — specifically their low viscosity and low surface tension — which make aspiration into the airways both easy and devastating. This understanding is the key to logical management: the goal is to minimise aspiration, not to empty the stomach.
Physicochemical basis of aspiration risk: Kerosene is an aliphatic petroleum distillate with a low viscosity (flows easily) and low surface tension (spreads readily across surfaces). These properties mean that during ingestion, vomiting, or any manoeuvre that brings kerosene near the larynx, it can penetrate deeply into the distal airways rather than being cleared by the cough reflex. It behaves very differently from water or food, which are viscous enough to pool in the pharynx and be swallowed or expelled as droplets.
Chemical pneumonitis mechanism: Once in the respiratory tract, chemical pneumonitis develops through a cascade of events. Kerosene directly dissolves pulmonary surfactant, causing alveolar instability and collapse. The lipophilic hydrocarbon irritates the bronchial and alveolar epithelium, triggering an intense inflammatory response — neutrophil influx, cytokine release, and mucosal oedema. The result is patchy ventilation-perfusion (V/Q) mismatch: perfused alveoli that are no longer ventilated divert deoxygenated blood directly to the pulmonary veins, causing hypoxaemia. In severe cases, secondary bacterial infection can complicate the picture (though prophylactic antibiotics are NOT indicated and worsen outcomes by promoting resistance).
Systemic absorption: Kerosene is poorly absorbed from an intact gastrointestinal mucosa because of its chemical nature. The systemic CNS effects seen in severe poisoning are largely attributable to hypoxaemia from aspiration pneumonitis rather than direct CNS toxicity from absorbed kerosene. This is a crucial distinction — it reinforces that the primary harm is pulmonary, and interventions should target the lungs (supportive oxygen therapy), not the gut.
Why gastric decontamination is contraindicated: Inducing vomiting or performing gastric lavage re-exposes the airway to kerosene. Because kerosene has already spread across the mucous membranes and the child's airway protective reflexes may be partially compromised, any further pharyngeal exposure dramatically increases the aspiration risk. The small benefit of removing a non-systemically-absorbed toxin from the gut is vastly outweighed by this risk. This is categorically different from, say, a paracetamol overdose where systemic absorption is the mechanism of harm and gastric decontamination has a role.
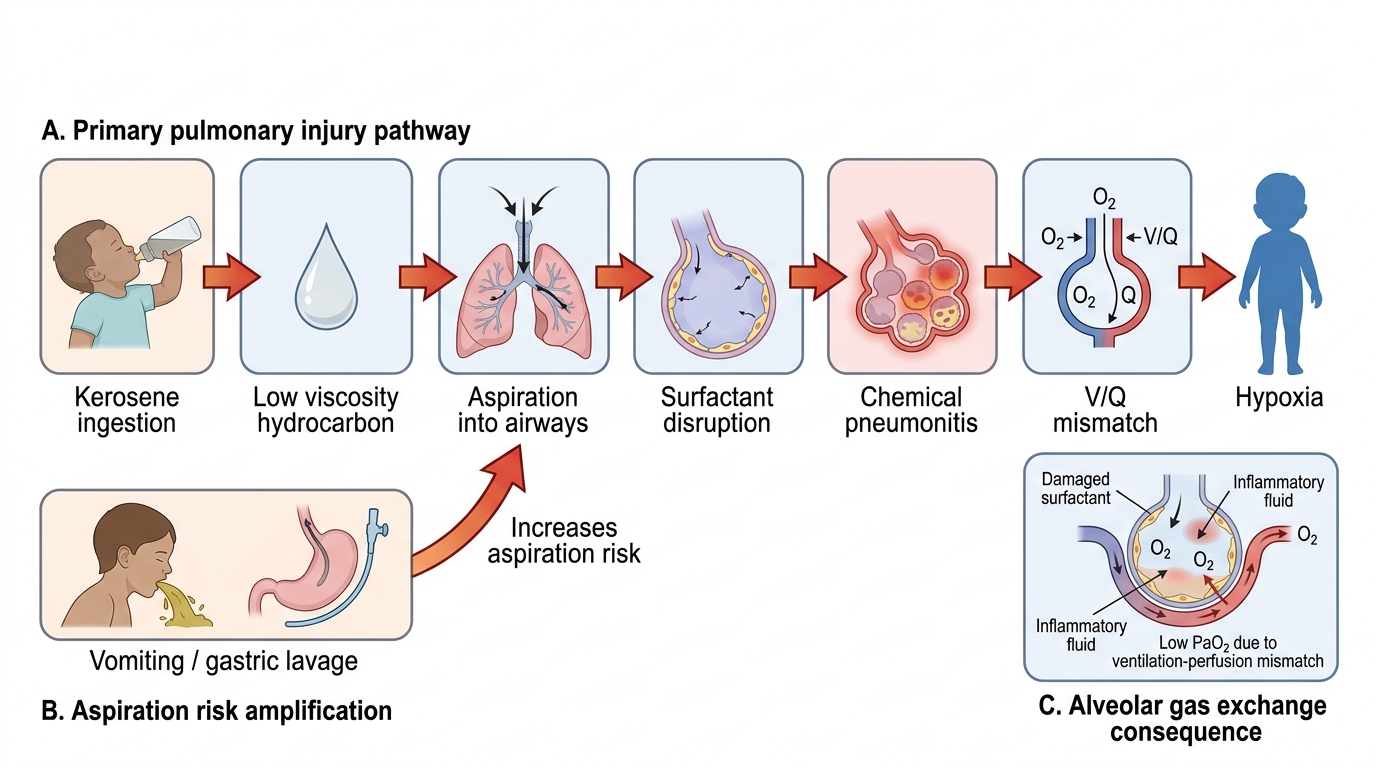
Kerosene Poisoning: Pulmonary Injury Mechanism
Risk Factors and Epidemiology in India
Understanding why kerosene ingestion is so prevalent in India requires examining the social, economic, and behavioural risk factors that converge in low-resource household settings. Epidemiological awareness guides preventive counselling — a core responsibility of the paediatrician.
Epidemiological profile: Kerosene poisoning accounts for approximately 10–15% of all childhood poisoning admissions in Indian paediatric hospitals. The peak age group is 1–5 years, when children are developmentally mobile and curious but lack the cognitive understanding of danger. Boys and girls are roughly equally affected at this age. Incidence is highest in summer months in some regions (when kerosene is more likely to be stored in accessible locations for cooking or lighting) and in households with lower socioeconomic status.
Household storage risk factors are the most important and modifiable:
- Unlabelled or repurposed containers: Kerosene is routinely stored in soft-drink bottles, water bottles, or tea tins — containers that a child associates with safe, palatable beverages. The child drinks it before the taste triggers an aversion.
- Accessible storage: Kerosene is stored at floor level or in low shelves within easy reach of toddlers, unlike medications which are often in higher cupboards.
- Subsidised kerosene distribution: Government PDS (Public Distribution System) kerosene supplies ensure its presence in almost every low-income household using traditional cooking or lighting methods.
Behavioural risk factors include unsupervised time in the kitchen or storeroom and the child's developmental stage of oral exploration. Rural households with poor access to childproofing materials and limited parental awareness of poisoning hazards have higher incidence.
Systemic risk factors: Limited access to Poison Control Centres (the national helpline is 1800-116-117), delayed presentation to secondary/tertiary care due to geographic barriers, and the persisting myth that inducing vomiting is the correct immediate response all worsen outcomes.
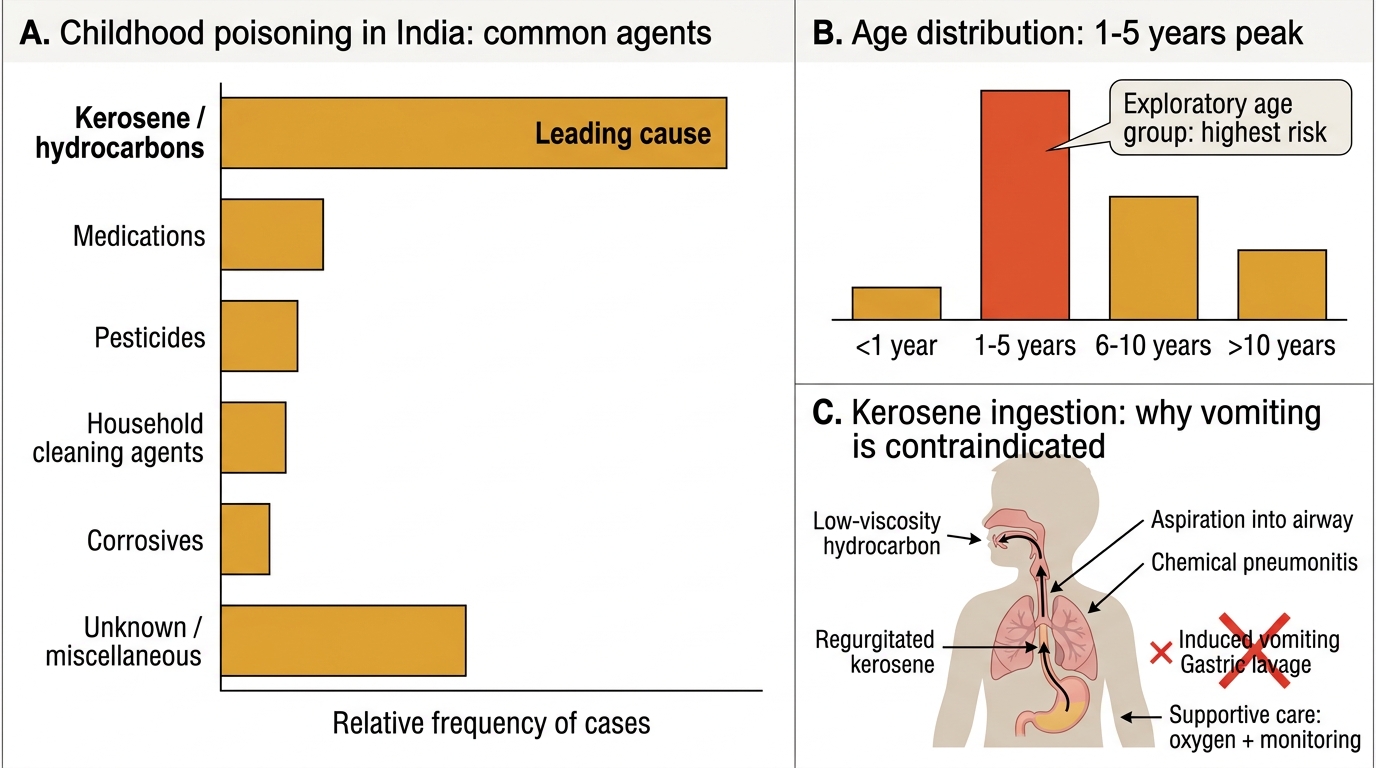
Childhood Poisoning in India: Agents, Age Peak, and Kerosene Risk
SELF-CHECK
A 3-year-old child is brought to the emergency department 20 minutes after kerosene ingestion. She is alert, coughing, and her SpO2 is 96% on room air. Her father asks whether he should have induced vomiting at home before bringing her. What is the correct response?
A. Vomiting should have been induced — it reduces gastric absorption of kerosene
B. Vomiting is contraindicated because kerosene aspiration into the airway is the primary mechanism of harm
C. Vomiting is safe if done within 1 hour of ingestion in alert children
D. Gastric lavage should be performed now at the hospital to clear residual kerosene
Reveal Answer
Answer: B. Vomiting is contraindicated because kerosene aspiration into the airway is the primary mechanism of harm
Vomiting (and gastric lavage) is CONTRAINDICATED in kerosene ingestion. Kerosene is a low-viscosity hydrocarbon that spreads readily across mucosal surfaces. The primary mechanism of harm is aspiration pneumonitis — not systemic GI absorption. Inducing vomiting or performing gastric lavage re-exposes the airway to kerosene, dramatically increasing aspiration risk. Management is supportive: oxygen, monitoring, bronchodilators if wheeze, no gastric decontamination.