Page 2 of 14
PE14.1 | Kerosene Ingestion — SDL Guide (Part 2)
Diagnosis and Investigation
The diagnosis of kerosene ingestion is primarily clinical, established by the history of exposure, the characteristic smell of petroleum on the child's breath and clothing, and the pattern of respiratory symptoms that follow. Investigations are directed at assessing the degree of respiratory compromise and monitoring for complications rather than confirming the diagnosis biochemically — there is no specific serum marker for hydrocarbon toxicity.
History: The most important diagnostic step is a careful history from the carer. Key questions include: the type and quantity of substance ingested, the time elapsed since ingestion, whether vomiting occurred (and whether it was spontaneous or induced), and any symptoms since ingestion. Note whether the container was labelled — in India, unlabelled soft-drink bottles containing kerosene are a common presentation pattern.
Clinical examination: Assess the airway for secretions or burns; examine the respiratory system for tachypnoea, recession (subcostal, intercostal), wheeze, and crepitations; measure SpO2 by pulse oximetry (the single most useful bedside tool). Document mental status — drowsiness or altered consciousness indicates either significant hypoxaemia or, rarely, direct CNS toxicity.
Chest X-ray (CXR): CXR is essential but must be interpreted with an important caveat — radiographic changes may lag clinical symptoms by 4–6 hours. A normal initial CXR does not exclude significant aspiration. Classic findings, when present, include bilateral lower zone infiltrates (particularly right lower lobe, due to its more vertical bronchus), perihilar haziness, and areas of hyperinflation or atelectasis. Serial CXRs may be needed to track progression.
Pulse oximetry: Continuous SpO2 monitoring is the cornerstone of assessment. SpO2 <94% on room air indicates significant respiratory compromise; SpO2 <90% warrants urgent supplemental oxygen and close respiratory support planning.
Blood investigations: Routine bloods are not required for diagnosis but may guide management:
- ABG (arterial blood gas): for pH, pO2, pCO2 in children with SpO2 <90% or increasing work of breathing
- Complete blood count: elevated neutrophil count may suggest bacterial superinfection (though absence of fever does not rule out early pneumonitis)
- Renal and liver function: in severe poisoning with suspected systemic absorption
There is NO role for serum hydrocarbon levels in routine management — results do not change immediate management and are not clinically validated for kerosene specifically.
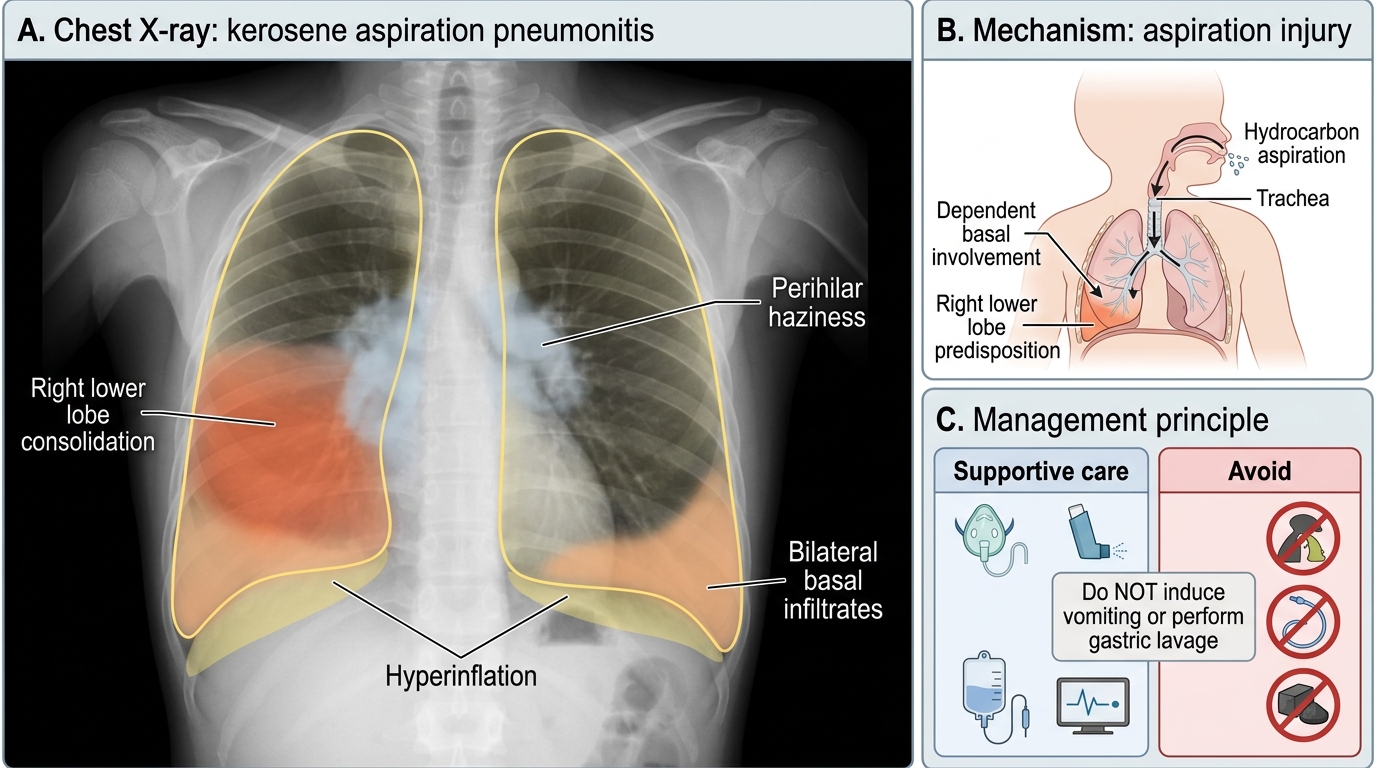
Kerosene Aspiration Pneumonitis: Chest X-ray Findings
CLINICAL PEARL
Critical trap — do NOT induce vomiting or perform gastric lavage in kerosene ingestion. This applies regardless of how much was ingested and how alert the child appears. The primary mechanism of harm is aspiration pneumonitis, not GI absorption. Even a small additional aspiration event can convert a mild ingestion into severe respiratory failure. Activated charcoal is also not effective for hydrocarbons and is NOT recommended. Management is entirely supportive: oxygen therapy, bronchodilators for wheeze, IV fluids if oral intake is impaired, and antibiotics ONLY if there is confirmed secondary bacterial pneumonia (not prophylactically). If in doubt about any intervention, ask: does this reduce aspiration risk, or increase it?
Management: Supportive Care and Contraindicated Interventions
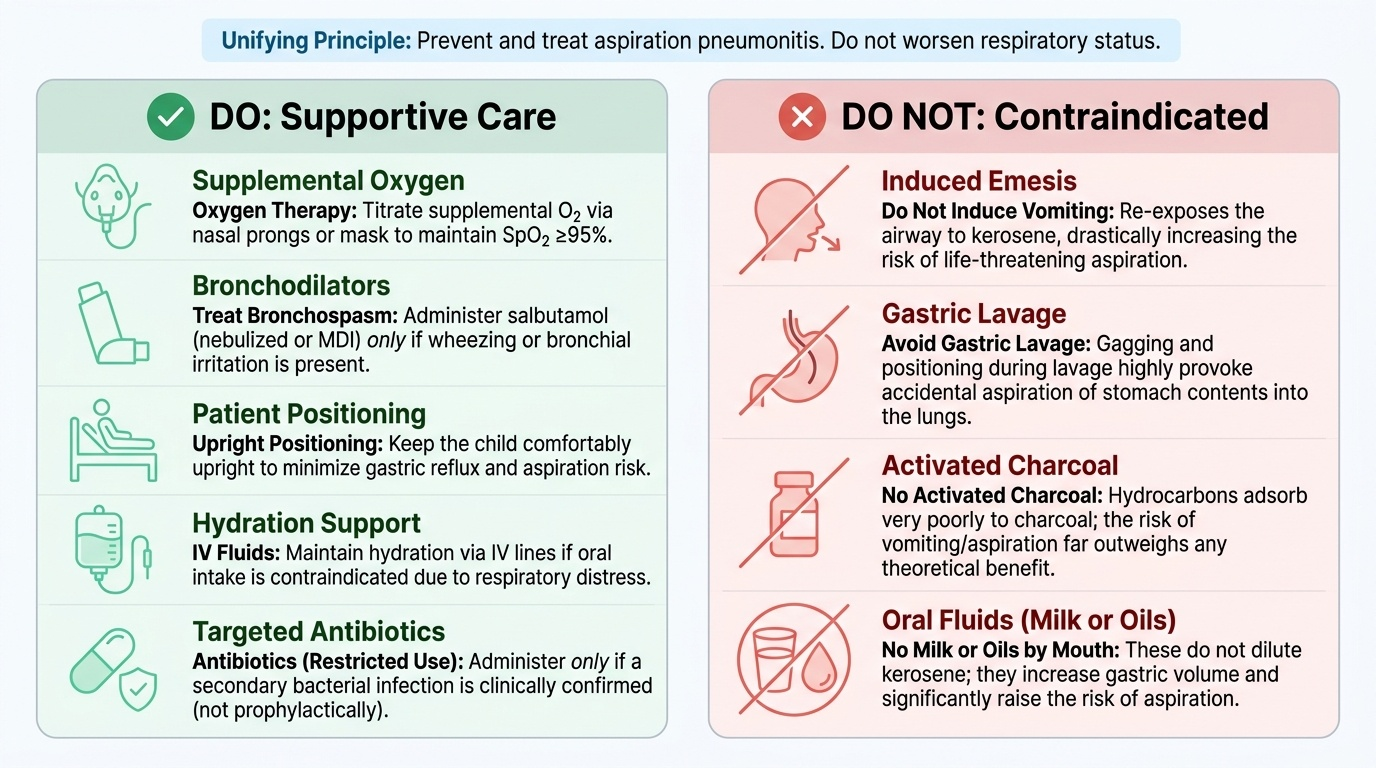
The management of kerosene ingestion is built on a single unifying principle: prevent and treat aspiration pneumonitis, and avoid any manoeuvre that worsens it. Every management decision flows from this principle. Because the primary mechanism of harm is aspiration — not systemic gastrointestinal absorption — the correct approach is entirely supportive, focused on oxygen delivery, monitoring, and treating complications. This contrasts sharply with the lay instinct of 'getting the poison out of the stomach,' which is the most dangerous thing a carer or untrained practitioner can do. The clinician must rapidly assess respiratory severity, categorise the child as mild, moderate, or severe, and act within a framework that includes a clearly defined list of contraindicated interventions. Understanding why these interventions are harmful — not merely that they are listed as contraindicated — enables confident clinical reasoning in any future poisoning scenario.
Provided image
Immediate assessment at presentation:
- Assess airway, breathing, and circulation (ABC)
- Apply pulse oximetry immediately
- Note the time of ingestion, quantity, and whether vomiting has occurred
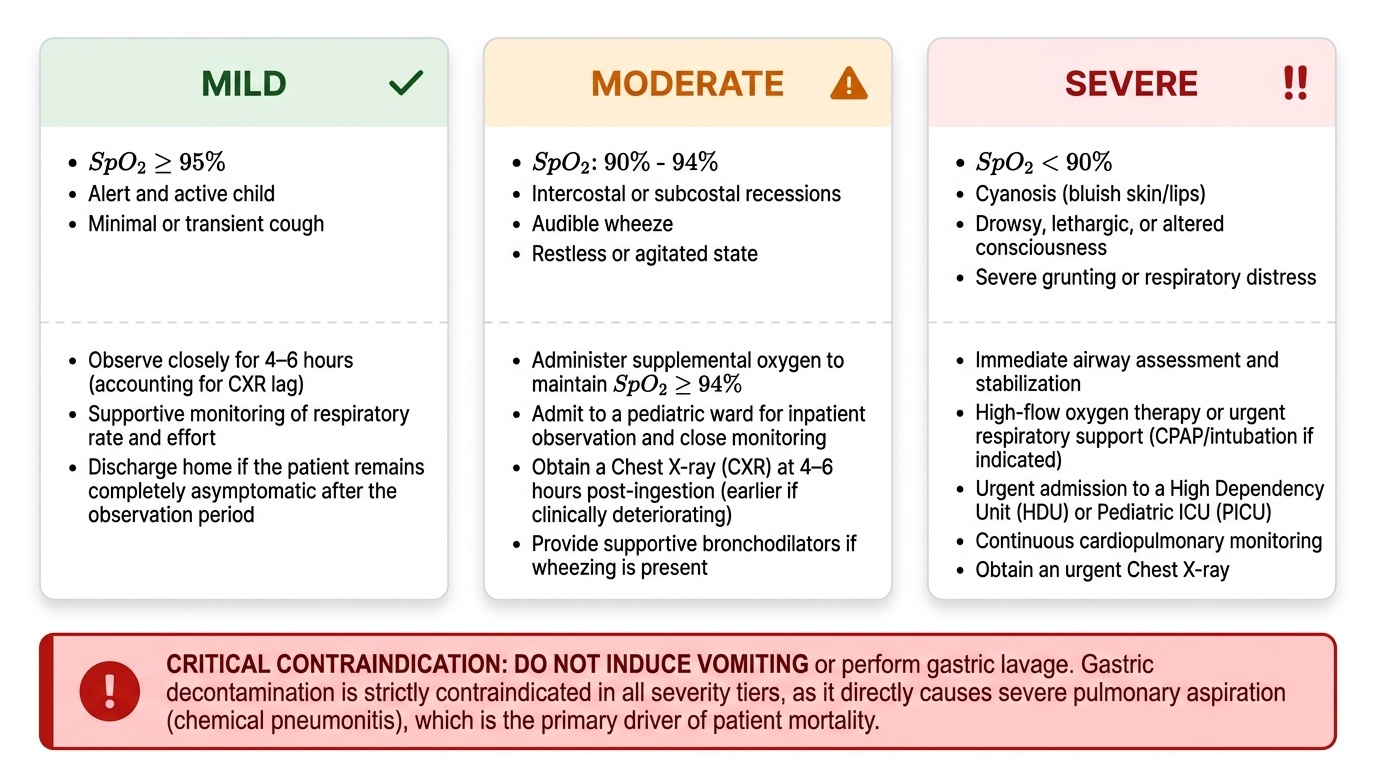
- Assign a severity level: mild (SpO2 ≥95%, no recession, minimal cough, alert), moderate (SpO2 90–94%, recession, wheeze, restless), severe (SpO2 <90%, marked recession, drowsy, cyanosis)
CONTRAINDICATED interventions (absolutely do NOT perform):
1. Induced emesis — re-exposes the airway to kerosene, greatly increases aspiration risk
2. Gastric lavage — same reason; also gagging and positioning required for lavage provokes aspiration
3. Activated charcoal — hydrocarbons adsorb poorly to charcoal; risk of aspiration outweighs any theoretical benefit
4. Oils or milk by mouth — do not give these in an attempt to dilute kerosene; no evidence of benefit and increases aspiration risk
Supportive management (the correct approach):
Respiratory support:
- Supplemental oxygen via nasal prongs, face mask, or non-rebreather mask, titrated to SpO2 ≥95%
- Bronchodilators (salbutamol via nebuliser or MDI, 2.5 mg nebulised or 2 puffs) if wheeze is present — kerosene irritates the bronchial mucosa and may induce bronchospasm
- Positioning: keep the child comfortable and upright (reduces aspiration risk from residual gastric contents)
- Avoid unnecessary stimulation that may cause vomiting
- In severe cases with respiratory failure: CPAP, mechanical ventilation via paediatric ICU
Systemic support:
- IV fluids if the child cannot drink safely (glucose maintenance as per Holliday-Segar: 100 mL/kg/day for first 10 kg, 50 mL/kg/day for next 10 kg, 20 mL/kg/day thereafter)
- Monitor urine output, glucose, and vital signs
- Nil by mouth until cough reflex is intact and respiratory status is stable
Antibiotics:
- NOT given prophylactically — early kerosene pneumonitis is a chemical/inflammatory process, not bacterial. Prophylactic antibiotics increase resistance without benefit.
- Give ONLY if secondary bacterial pneumonia is confirmed: fever persisting >48–72 h after ingestion, new consolidation on CXR, leucocytosis with neutrophilia, clinical deterioration after initial improvement
- If required, use co-amoxiclav (25 mg/kg/day amoxicillin component, twice daily) or ampicillin-cloxacillin based on local protocol
Corticosteroids: Not recommended — evidence does not support their use in hydrocarbon pneumonitis.
Observation and discharge criteria:
- Observe for minimum 6 hours from ingestion; longer (24 h) if any respiratory symptoms
- Discharge if: SpO2 ≥95% on room air, no respiratory distress, alert and able to take oral fluids, CXR (if taken) without progressive infiltrates
- Discharge with family counselling on danger signs requiring return (worsening cough, fast breathing, cyanosis)
Prevention and Counselling
Prevention of accidental kerosene ingestion requires a combination of household-level behavioural changes, community education, and policy-level interventions. The paediatrician and general practitioner play a key role in anticipatory guidance — proactively advising families about household chemical hazards at each well-child visit, before an accident occurs rather than only in response to one. In India, where kerosene remains a subsidised cooking and lighting fuel distributed through the public distribution system, the risk is embedded in the domestic environment of millions of low-income families. Effective prevention therefore addresses both individual family behaviour (how and where kerosene is stored) and broader determinants (access to safer fuels, poison control awareness, community education). The paediatrician's role is to translate this population-level risk into actionable, specific advice at the individual consultation — advice that parents can implement immediately and remember in an emergency.
Household storage counselling (primary prevention):
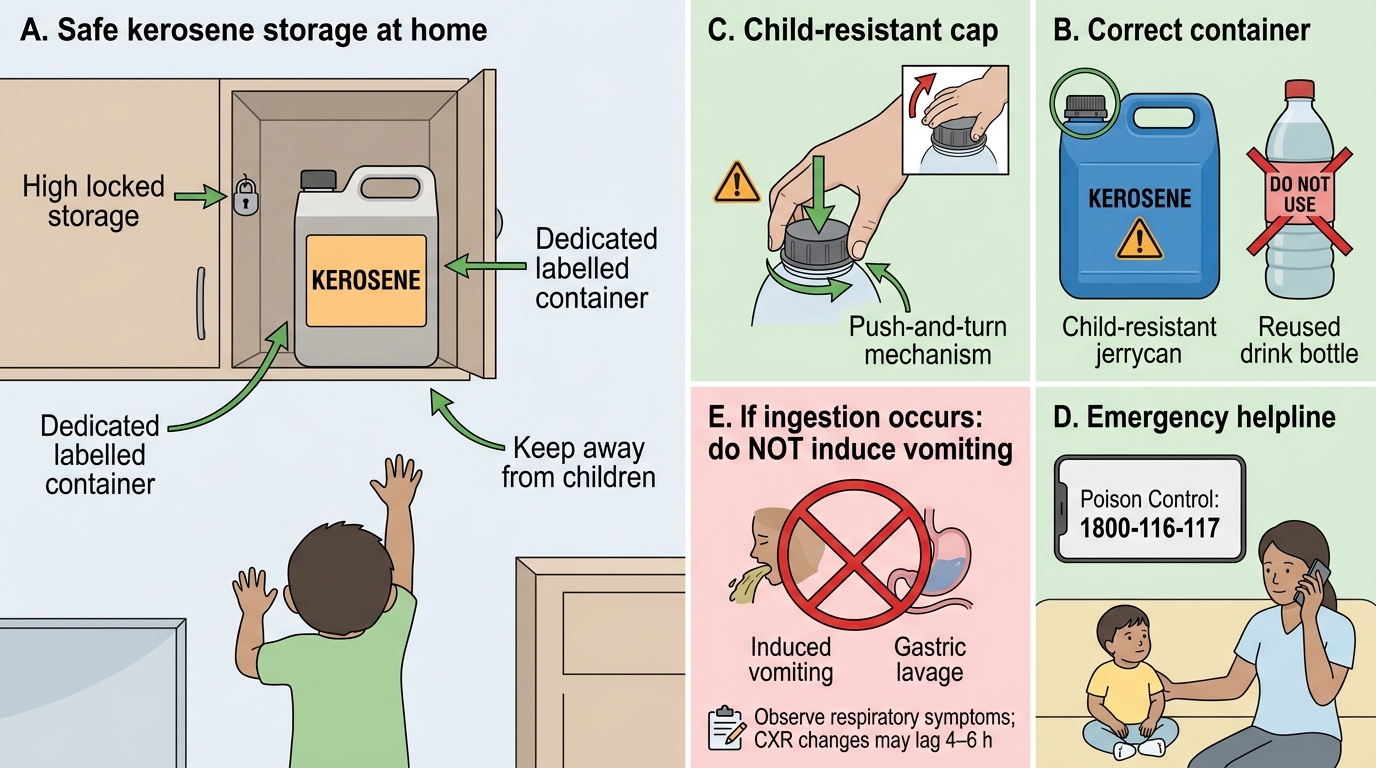
- Never store kerosene in food or beverage containers. Kerosene must be kept in its original, clearly labelled container — ideally a dedicated, distinctively shaped, colour-coded container that a child does not associate with a drink.
- Store kerosene at height — in a locked, high cupboard inaccessible to young children. The same applies to all household chemicals and medications.
- Child-resistant closures: If available, use containers with child-proof caps.
- Designate a specific, secure storage location and consistently use it — many accidents occur because the container was temporarily left accessible during use.
Supervision: Never leave young children (1–5 years) unsupervised in the kitchen, storeroom, or near cooking equipment. Developmental curiosity is normal; environmental safety is the caregiver's responsibility.
National Poison Control Helpline: Families should be informed of the national helpline 1800-116-117 (toll-free, 24-hour). Advise them to call immediately on suspected ingestion for guidance, and to bring the container or a photograph of the label to the emergency department.
What to do if ingestion occurs:
- Do NOT give anything by mouth to induce vomiting
- Do NOT give milk or oil
- Remove the child from further exposure; remove contaminated clothing
- Rinse the mouth with water if the child is alert and can cooperate — do not make the child swallow
- Proceed to the nearest hospital immediately
Advocacy: At the population level, advocacy for safer kerosene containers with child-resistant closures, community awareness programmes, and eventual transition to safer cooking fuels (LPG, electric induction) are the long-term preventive strategies.
Household Kerosene Safety and First Response
SELF-CHECK
A 4-year-old child has a chest X-ray taken 1 hour after kerosene ingestion. The X-ray is reported as normal. His SpO2 is 97% and he has a mild cough. What is the correct interpretation and plan?
A. Normal CXR confirms no aspiration has occurred — discharge the child immediately
B. CXR changes in aspiration pneumonitis may lag by 4–6 hours — observe for at least 6 hours
C. A normal CXR means gastric lavage is now safe to perform
D. Start prophylactic antibiotics to prevent secondary bacterial pneumonia
Reveal Answer
Answer: B. CXR changes in aspiration pneumonitis may lag by 4–6 hours — observe for at least 6 hours
CXR changes in kerosene aspiration pneumonitis characteristically lag clinical symptoms by 4–6 hours. A normal initial CXR does NOT exclude significant aspiration. The child should be observed for at least 6 hours (and longer if symptoms develop) with continuous pulse oximetry. Gastric lavage remains contraindicated regardless of CXR findings. Prophylactic antibiotics are not indicated — antibiotics are reserved for confirmed secondary bacterial pneumonia (fever persisting >48–72 h, progressive consolidation).
Self-Assessment: Kerosene Ingestion
Use these questions to consolidate your understanding of the key principles from this module before moving on. Kerosene ingestion is a topic where a single conceptual error — believing that gastric decontamination is the correct first response — can cause direct patient harm. Final-year students are expected to handle this poisoning confidently: to know the mechanism of toxicity (aspiration chemical pneumonitis, not systemic gastrointestinal absorption), to immediately identify and refuse the contraindicated interventions even under pressure from carers, to interpret an initially normal chest X-ray correctly (CXR changes lag by 4–6 hours), and to apply purely supportive management without adding harmful interventions. Self-assessment at this stage is not merely about recall — it is about verifying that your clinical reasoning is sound enough that you would make the correct decision at the bedside without hesitation.
Provided image
Key concepts to be able to explain:
1. Why is kerosene ingestion primarily a pulmonary emergency, not a GI emergency?
2. What is the exact contraindication to gastric decontamination, and why?
3. What chest X-ray finding is expected in aspiration pneumonitis, and at what time point?
4. When (if ever) are antibiotics indicated in kerosene ingestion?
5. What are the discharge criteria after kerosene ingestion?
6. What anticipatory guidance should you provide to the family of a child presenting with kerosene ingestion?
Self-check questions:
Q1: A neighbour calls to say her 2-year-old has just swallowed kerosene. She asks: 'Should I make him vomit?' Your answer:
→ Absolutely NOT. Instruct her to keep the child calm, do not give anything to induce vomiting, and bring him immediately to the nearest emergency department. Induce vomiting only increases aspiration risk.
Q2: Why is the right lower lobe the most commonly affected zone in aspiration pneumonitis?
→ The right main bronchus is more vertical than the left and has a larger diameter, making it the preferential airway for aspirated material to travel down under gravity.
Q3: Name two interventions that should be performed and two that are contraindicated in kerosene ingestion.
→ Perform: supplemental oxygen (titrate to SpO2 ≥95%), bronchodilators if wheeze present. Contraindicated: induced emesis, gastric lavage.