Page 7 of 14
PE14.3 | Paracetamol Poisoning — SDL Guide
Learning Objectives
- Identify the risk factors for paracetamol poisoning in children, including accidental ingestion, intentional overdose, and therapeutic misadventure
- Explain the pathophysiology of paracetamol-induced hepatotoxicity through NAPQI production and glutathione depletion
- Recognise the four clinical phases of paracetamol poisoning and the deceptive apparent improvement in Phase II
- Interpret the Rumack-Matthew nomogram to determine whether N-acetylcysteine treatment is indicated
- Apply the correct management: activated charcoal within 1 hour, N-acetylcysteine (NAC) protocol with correct paediatric dosing, and supportive care for hepatic failure
- Explain why the NAC window (most effective within 8–10 hours) is the critical therapeutic decision point
INSTRUCTIONS
Paracetamol (acetaminophen) is the most widely available over-the-counter analgesic and antipyretic in India — and in overdose, a cause of potentially fatal hepatic failure that is both preventable and treatable if identified early. The insidious danger is the Phase II apparent recovery, where the child looks well for 24–72 hours after a large ingestion while hepatocellular destruction is already occurring. By the time jaundice, coagulopathy, and encephalopathy appear in Phase III, the window for effective antidote therapy may have passed. This module teaches you to recognise the poisoning early, use the Rumack-Matthew nomogram correctly, and initiate N-acetylcysteine (NAC) within the therapeutic window.
References
- Ghai Essential Pediatrics, 9th Edition — Chapter on Poisoning (textbook)
- Nelson Textbook of Pediatrics, 21st Edition — Acetaminophen Toxicity (textbook)
- IAP Guidelines on Management of Common Childhood Poisoning (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 13-year-old girl is brought to the emergency department by her mother at 11 PM. The mother says she found an empty strip of paracetamol tablets (500 mg × 10 tablets = 5 g) in her daughter's room. When asked, the girl says she took them 'about 3 hours ago' after a fight with her parents. She weighs 35 kg. Her calculated dose is approximately 143 mg/kg. She appears well — no vomiting, no abdominal pain, alert and oriented. Her mother is reassured: 'She looks fine, doctor.' What is the correct assessment and plan? Should you send her home, observe for 6 hours, or start treatment immediately?
WHY THIS MATTERS
Paracetamol poisoning is uniquely dangerous because of the gap between the time of ingestion and the appearance of serious clinical harm. Unlike most toxins where symptoms guide urgency, paracetamol's most dangerous phase — hepatic failure — begins biochemically and invisibly while the patient looks and feels well. The therapeutic window for the antidote N-acetylcysteine is narrow: most effective within 8–10 hours, efficacy declining progressively beyond that. In India, paracetamol is sold without prescription, stocked in every household, and used as the first response to fever and pain — making accidental ingestion by young children and intentional overdose by adolescents a recurring emergency. Understanding the pathophysiology, using the Rumack-Matthew nomogram correctly, and initiating NAC without waiting for symptoms is the clinical skill this module builds.
RECALL
Before studying paracetamol toxicology, recall these key concepts:
- Hepatic drug metabolism: Most drugs undergo Phase I reactions (CYP450 oxidation/reduction/hydroxylation) and Phase II conjugation (glucuronidation, sulfation, or glutathione conjugation) before renal or biliary excretion. Phase II reactions generally produce water-soluble, non-toxic products.
- CYP2E1 is a cytochrome P450 isoenzyme particularly active in the metabolism of paracetamol at high doses, and is induced by alcohol and fasting.
- Glutathione is a tripeptide (glutamate-cysteine-glycine) that acts as a cellular antioxidant and electrophile scavenger in hepatocytes. Stores are finite and can be depleted by sustained toxic metabolite production, nutritional deficiency, or fasting.
- Liver function tests: ALT (alanine aminotransferase) and AST (aspartate aminotransferase) are released from damaged hepatocytes — elevated in hepatocellular injury. INR (international normalised ratio) reflects hepatic synthetic function; prolongation indicates coagulation factor deficiency.
Clinical Presentation of Paracetamol Poisoning
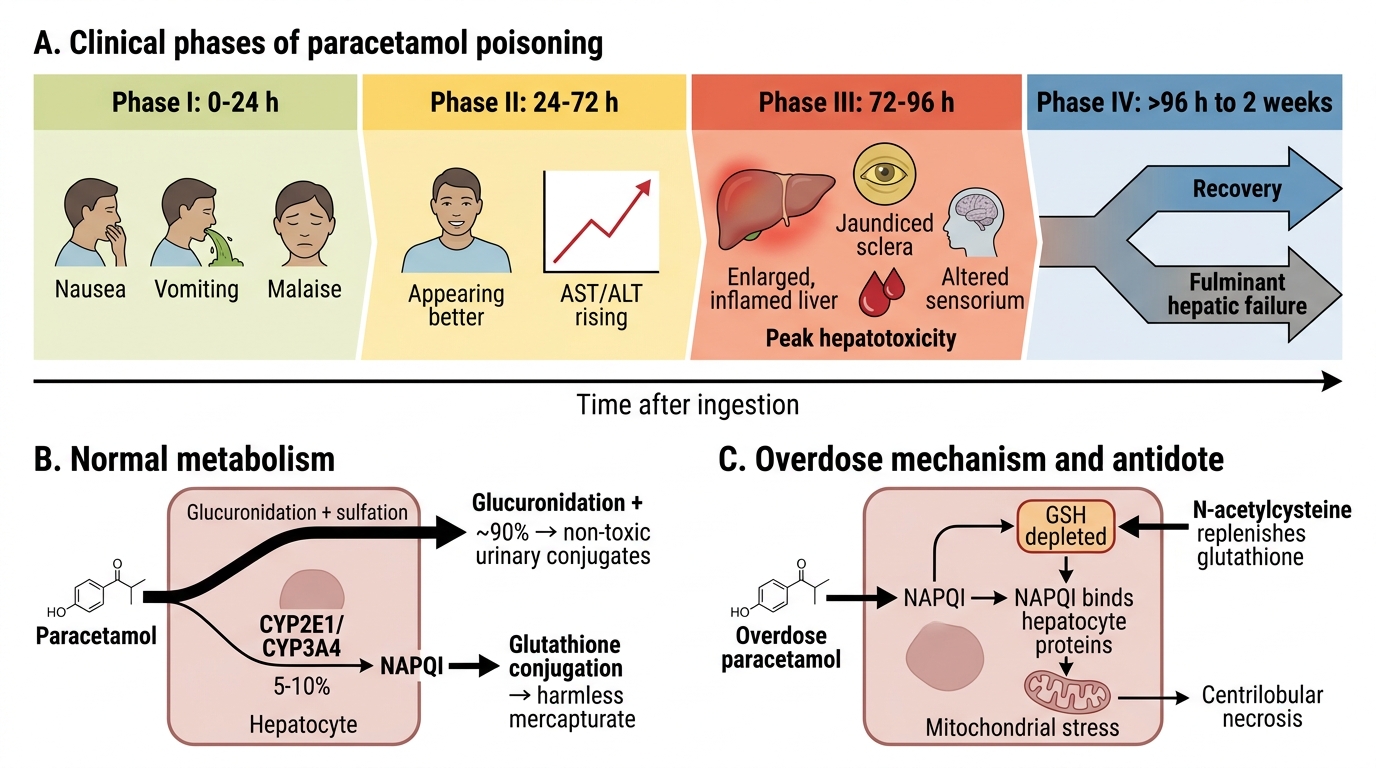
The clinical presentation of paracetamol poisoning is characterised by four sequential phases that span 4–7 days following a significant overdose. Understanding this temporal pattern is essential because the most dangerous phase (Phase III, hepatic failure) is preceded by a period of apparent well-being that can falsely reassure both the family and an inexperienced clinician. The critical clinical insight is that normal examination and absence of symptoms in the first 24 hours do NOT rule out serious paracetamol toxicity — the biochemical injury has already begun. Final-year students must resist the temptation to reassure based on appearance alone and instead act on the ingested dose and the Rumack-Matthew nomogram result.
Phase I (0–24 hours): Initial symptoms. The child may experience nausea, vomiting, anorexia, malaise, and pallor. These symptoms are non-specific and mild, often dismissed as a viral illness. Some children with large overdoses remain entirely asymptomatic in Phase I. This phase does not correlate with the eventual severity of hepatic injury.
Phase II (24–72 hours): Apparent recovery. Phase I symptoms resolve. The child appears clinically well. This is the most treacherous phase — the patient looks recovered, but hepatocellular necrosis is actively occurring. Transaminases (ALT, AST) begin to rise silently. Families and clinicians who are not aware of this phase may conclude that no harm occurred. Right upper quadrant tenderness may develop.
Phase III (72–96 hours): Peak hepatotoxicity. This is the fulminant phase if the overdose was large and treatment was not given. Features of acute hepatic failure appear: jaundice, hepatomegaly with right upper quadrant pain, coagulopathy (INR rise, bleeding), hypoglycaemia, metabolic acidosis, oliguria, and hepatic encephalopathy (ranging from confusion to deep coma). ALT and AST peak — values of >1000 U/L or even >10,000 U/L in severe poisoning. Renal failure (hepatorenal syndrome or direct tubular toxicity) may accompany hepatic failure.
Phase IV (days 4–7): Resolution or death. With adequate NAC treatment given early, the vast majority of patients recover completely, including biochemical normalisation. Without treatment, severe cases progress to fulminant hepatic failure and death. Survivors without transplantation have complete hepatic regeneration.
| Phase | Timing | Key Features | Danger |
|---|---|---|---|
| I | 0–24 h | Nausea, vomiting, malaise (may be asymptomatic) | May reassure falsely — injury already beginning |
| II | 24–72 h | Apparent recovery; transaminases rise silently | Most dangerous for missing treatment window |
| III | 72–96 h | Jaundice, coagulopathy, encephalopathy, renal failure | Fulminant hepatic failure, death |
| IV | Day 4–7 | Recovery (with treatment) or death (without) |
Clinical Phases and Mechanism of Paracetamol Poisoning
Pathophysiology: Glutathione Depletion and Hepatotoxicity
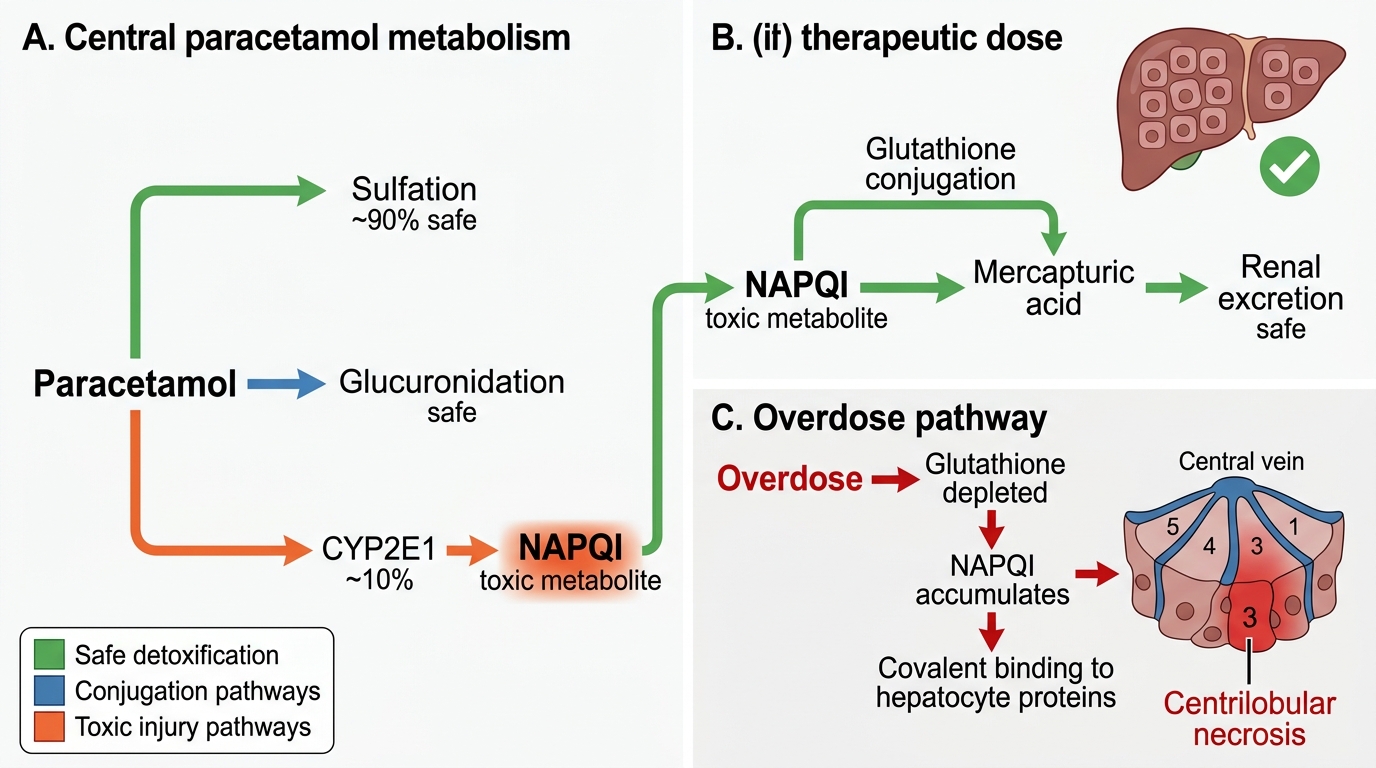
The pathophysiology of paracetamol poisoning centres on a single toxic metabolite — NAPQI (N-acetyl-p-benzoquinone imine) — that is produced in small amounts during normal therapeutic use but accumulates to dangerous levels in overdose. Understanding this mechanism makes the rationale for both the dose threshold and the NAC antidote immediately logical.
Normal paracetamol metabolism: At therapeutic doses, paracetamol is metabolised primarily by hepatic Phase II reactions — approximately 90% undergoes glucuronidation and sulfation, both producing water-soluble, non-toxic conjugates that are excreted in urine. A minor fraction (approximately 5–10%) is oxidised by CYP2E1 (and CYP3A4) to produce NAPQI, a highly reactive electrophile. At therapeutic doses, NAPQI is rapidly and completely detoxified by conjugation with glutathione (a tripeptide antioxidant in hepatocytes), producing a harmless mercapturate that is excreted. Hepatocytes contain sufficient glutathione under normal circumstances to handle this small NAPQI burden without injury.
Overdose mechanism — glutathione depletion: When paracetamol is ingested in toxic amounts (>150 mg/kg in children), the glucuronidation and sulfation pathways become saturated, and proportionally more paracetamol is channelled through CYP2E1, generating a larger NAPQI load. Glutathione stores are finite and become depleted — once stores fall below approximately 30% of normal, NAPQI is no longer adequately detoxified. The unquenched NAPQI then binds covalently to hepatocyte proteins and mitochondria, disrupting cellular respiration and causing centrilobular hepatic necrosis (zone 3 of the hepatic acinus, where CYP2E1 activity is highest and oxygen tension is lowest).
Why centrilobular? Zone 3 hepatocytes (perivenular, surrounding the central vein) are most susceptible because CYP2E1 is most concentrated there and oxygen tension is lowest — making them most vulnerable to oxidative mitochondrial injury.
Factors that increase susceptibility: Conditions that reduce glutathione stores or upregulate CYP2E1 increase toxicity at lower paracetamol doses: fasting and malnutrition (glutathione synthesis requires cysteine), chronic alcohol use (CYP2E1 induction), and concurrent hepatic disease.
How NAC works: N-acetylcysteine (NAC) is a cysteine prodrug — it replenishes hepatocyte cysteine (the rate-limiting substrate for glutathione synthesis), thereby restoring glutathione stores and providing additional capacity to detoxify NAPQI. It also acts as a direct NAPQI scavenger and improves hepatic microcirculation. Its efficacy is greatest when given before or during NAPQI accumulation (within 8–10 hours), though it retains some benefit up to 24 hours.
Paracetamol Metabolism and Hepatotoxicity in Overdose
Risk Factors and Epidemiology
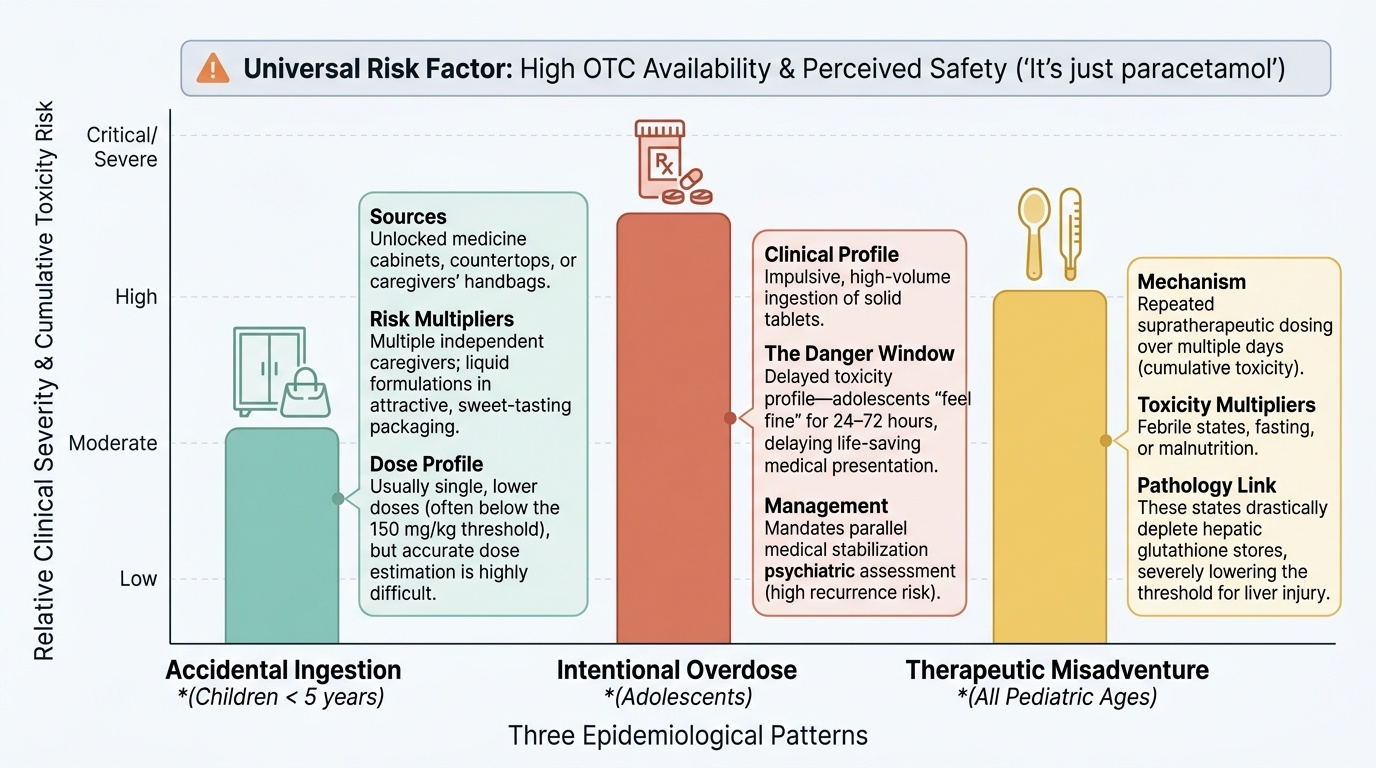
Paracetamol poisoning in children occurs through three distinct epidemiological patterns, each with different risk factors, clinical profiles, and prevention implications. Understanding these patterns helps the clinician anticipate which patients are at highest risk and direct counselling appropriately. In India, the universal availability of paracetamol as an OTC medication, its perceived safety ('it's just paracetamol'), and its use across all socioeconomic groups make it the most common pharmaceutical agent in paediatric poisoning.
Provided image
Pattern 1 — Accidental ingestion (children <6 years): Young children ingest tablets or syrup found at home, typically from unlocked cabinets or caregivers' handbags. Doses are often lower and less likely to reach the toxic threshold (>150 mg/kg), but accurate dose estimation can be difficult. Risk factors include storage of medications within reach, multiple caregivers administering doses independently, and liquid formulations in attractive packaging.
Pattern 2 — Intentional overdose (adolescents): The most clinically dangerous pattern — adolescents in distress may ingest large numbers of tablets impulsively. Paracetamol is chosen because of its accessibility rather than lethality intent; the adolescent may not realise that the harm is delayed and that they 'feel fine' for 24–72 hours. This group requires both medical and psychiatric management. Suicide attempt in adolescence carries significant recurrence risk and requires formal psychiatric assessment.
Pattern 3 — Therapeutic misadventure: Repeated supratherapeutic dosing — giving slightly higher-than-recommended doses multiple times over days — can accumulate toxicity, particularly in children who are febrile, fasting, or malnourished (all states that reduce glutathione). This pattern presents with chronic, progressive hepatic injury rather than an acute single-ingestion history.
Risk factors for greater toxicity at any given dose:
- Malnutrition or prolonged fasting (reduced hepatic glutathione)
- Concurrent use of CYP2E1-inducing medications
- Pre-existing hepatic disease
- Young age with proportionally higher per-kg doses from accidental ingestion
SELF-CHECK
A 4-year-old child, weight 18 kg, is thought to have ingested one 500 mg paracetamol tablet approximately 2 hours ago. She is asymptomatic. What is the ingested dose, and how should this be managed?
A. Dose is 28 mg/kg — below the toxic threshold of 150 mg/kg; reassure and discharge
B. Dose is 28 mg/kg — below the toxic threshold; give activated charcoal immediately
C. Dose is 28 mg/kg — below the toxic threshold; observe 6 hours and check LFTs
D. Dose is 28 mg/kg — requires N-acetylcysteine regardless of dose
Reveal Answer
Answer: A. Dose is 28 mg/kg — below the toxic threshold of 150 mg/kg; reassure and discharge
The ingested dose is 500 mg ÷ 18 kg = 27.8 mg/kg, well below the toxic threshold of 150 mg/kg. At this dose, significant hepatotoxicity is not expected. The child may be reassured and discharged with advice to return if any symptoms develop. Activated charcoal is only indicated for doses above the potentially toxic threshold (>150 mg/kg) and within 1 hour of ingestion. NAC is reserved for doses above the treatment threshold on the Rumack-Matthew nomogram. Always calculate doses in mg/kg for children — never estimate from the adult threshold alone.