Page 8 of 14
PE14.3 | Paracetamol Poisoning — SDL Guide (Part 2)
Diagnosis and Investigation: The Rumack-Matthew Nomogram
The diagnosis of paracetamol poisoning is established by the history of ingestion, and the decision to treat is guided primarily by the Rumack-Matthew nomogram — a validated tool that plots plasma paracetamol concentration against time since ingestion to determine the likelihood of significant hepatotoxicity and the need for antidote therapy. The nomogram is central to management and must be understood both in terms of how to use it and what its limitations are.
When to measure plasma paracetamol: A plasma level should be measured at 4 hours or later after ingestion — before 4 hours, absorption may be incomplete and the level is uninterpretable for nomogram use. If the exact time of ingestion is unknown, draw a level immediately and repeat at 4 hours or at a known time reference to allow nomogram plotting.
How the Rumack-Matthew nomogram works: The nomogram has plasma paracetamol concentration on the Y-axis (µg/mL or µmol/L) and hours post-ingestion on the X-axis. A treatment threshold line (sometimes called the 'treatment line' at 150 µg/mL at 4 hours in its original form) defines the risk boundary:
- Plasma level ABOVE the treatment line → risk of significant hepatotoxicity → start NAC immediately
- Plasma level BELOW the treatment line → low risk → monitoring only, NAC not required
The original nomogram has been modified in different countries with varying degrees of conservatism (the UK uses a single line at 100 µg/mL at 4 hours regardless of risk factors; some authorities use 150 µg/mL). Use your institution's guideline and state which threshold you are applying.
Nomogram limitations — critical for clinical use:
- Valid ONLY for acute single-ingestion events — not for repeated/staggered dosing (therapeutic misadventure)
- Valid ONLY for levels taken at 4 hours or later post-ingestion
- Does NOT apply to patients with risk factors for enhanced toxicity (malnutrition, fasting, hepatic disease, enzyme-inducing drugs) — some guidelines use a lower treatment threshold for high-risk patients
- Not validated in children under 6 years with chronic ingestion patterns
Liver function and other investigations:
- ALT, AST, bilirubin, INR/PT — baseline at presentation; repeat at 24, 48, and 72 hours. Transaminases begin rising in Phase II and peak in Phase III.
- Blood glucose — hypoglycaemia in hepatic failure
- Renal function (creatinine, urea) — hepatorenal syndrome in severe cases
- ABG — metabolic acidosis indicates poor prognosis
- Full blood count, electrolytes
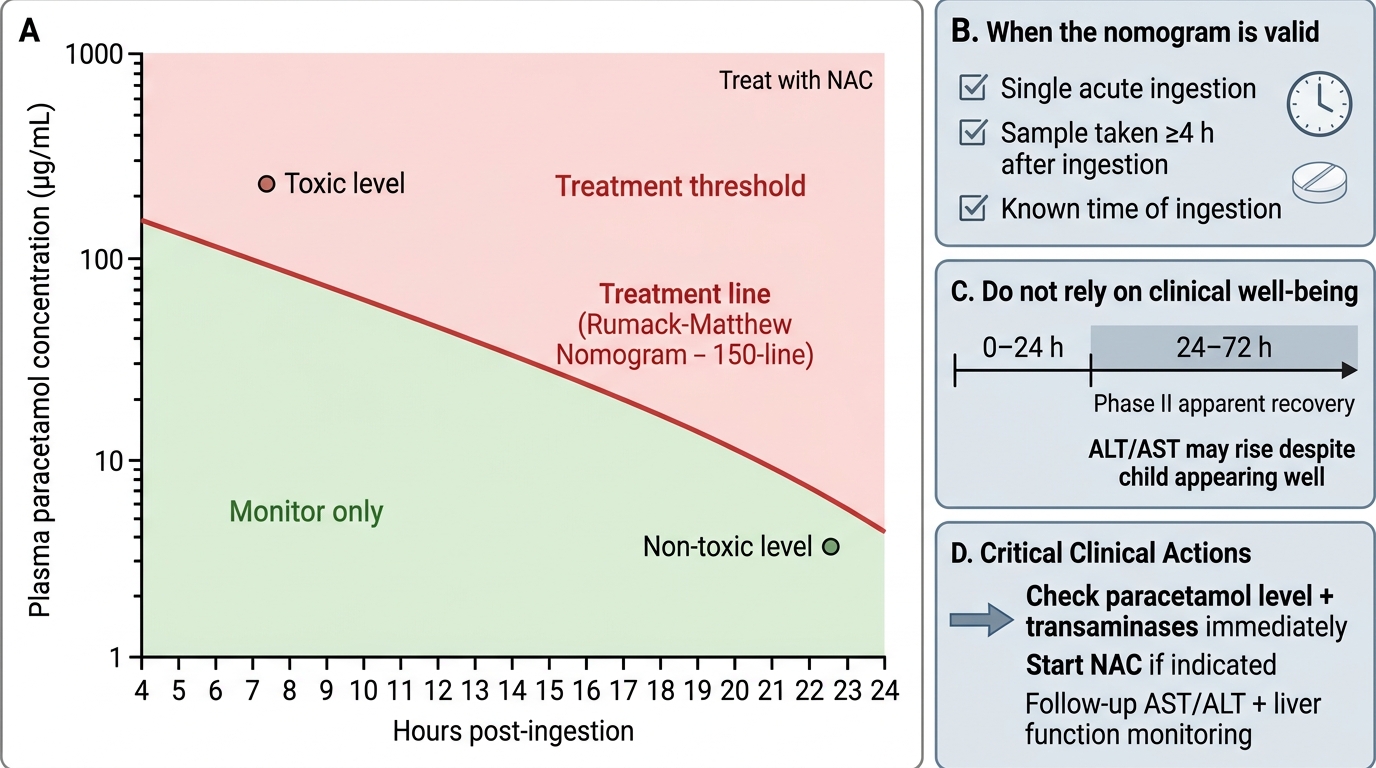
Rumack-Matthew Nomogram for Paracetamol Poisoning
CLINICAL PEARL
The Phase II apparent recovery is a clinical trap. A child who ingested a large paracetamol dose 36 hours ago and now looks well — eating, playing, afebrile — is in the most dangerous phase of paracetamol poisoning, not the safest. Phase II (24–72 hours) is when hepatocellular necrosis is occurring invisibly. Check transaminases (ALT, AST) and the plasma paracetamol level. If NAC has not been started and the level (corrected for time on the nomogram) or rising transaminases indicate toxicity, start NAC immediately — it retains partial benefit up to 24 hours and some benefit even beyond that in severe cases. Do not be falsely reassured by clinical well-being in this time window.
Management: N-Acetylcysteine and Supportive Care
Management of paracetamol poisoning is time-sensitive but follows a clear algorithmic approach: first, decontaminate if within the activated charcoal window; second, risk-stratify using the Rumack-Matthew nomogram; third, start NAC if indicated; fourth, provide supportive care for established hepatic failure. The most common error is delayed NAC initiation — 'waiting for symptoms' is the wrong approach, because by the time symptoms of hepatic failure appear, the optimal therapeutic window has passed. NAC must be started on the basis of dose and nomogram level, not on clinical appearance.
Provided image
Step 1 — Activated charcoal (within 1 hour of ingestion): If the child presents within 1 hour of a potentially toxic ingestion and can protect the airway, activated charcoal (1 g/kg, maximum 50 g) adsorbs paracetamol in the gut and reduces systemic absorption. Beyond 1 hour, charcoal is generally not recommended as paracetamol is rapidly absorbed. Note: this is different from hydrocarbons where charcoal is never used — paracetamol is adsorbed by activated charcoal.
Step 2 — Risk stratification using the Rumack-Matthew nomogram: Measure plasma paracetamol level at ≥4 hours post-ingestion. Plot on the nomogram. If above the treatment line, start NAC regardless of clinical status. If below the treatment line AND dose was <150 mg/kg, monitor clinically.
Step 3 — N-acetylcysteine (NAC) protocol:
NAC is a cysteine prodrug that replenishes hepatic glutathione stores and directly scavenges NAPQI. It is the definitive antidote.
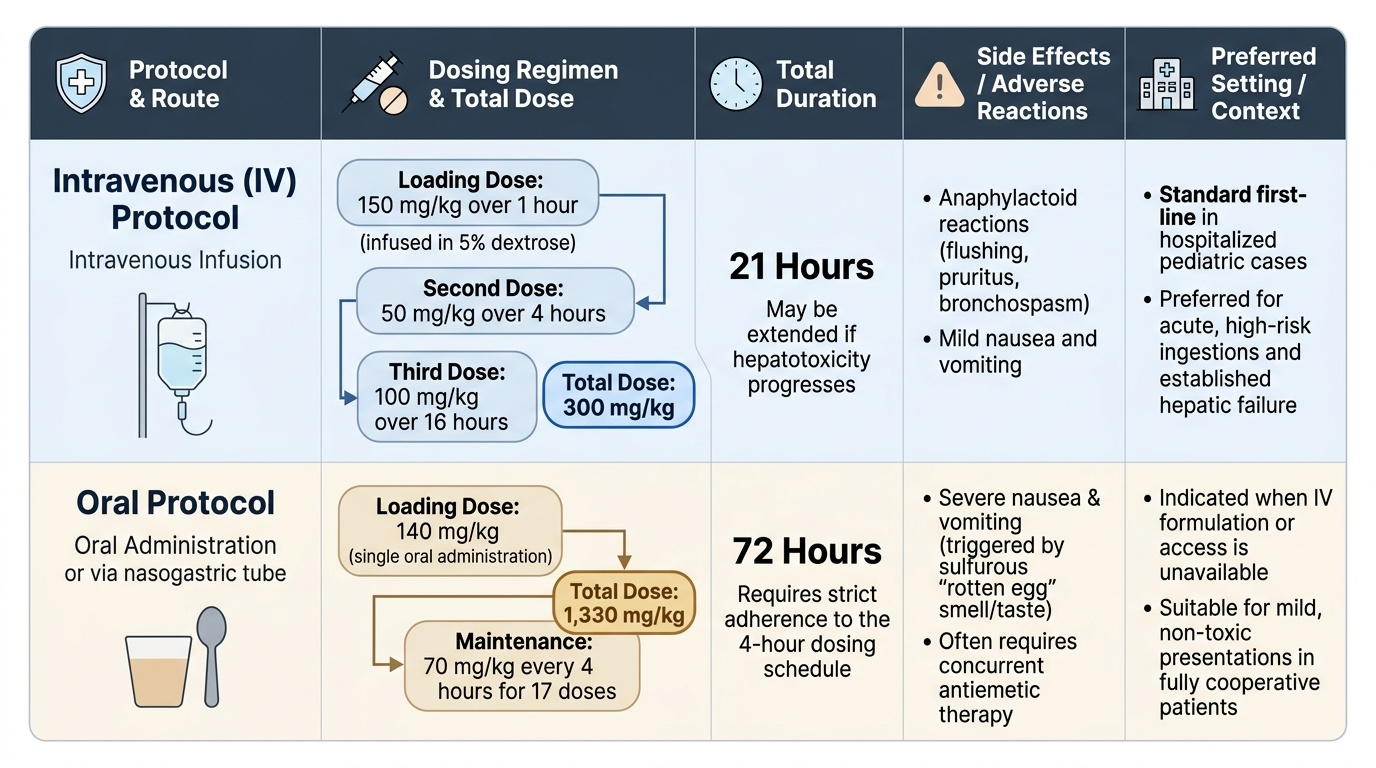
IV protocol (standard in hospitalised children):
- Loading dose: 150 mg/kg IV in 5% dextrose over 1 hour
- Second dose: 50 mg/kg IV over 4 hours
- Third dose: 100 mg/kg IV over 16 hours
- Total: 300 mg/kg over 21 hours; may be extended or repeated if hepatotoxicity progresses
Oral protocol (where IV unavailable):
- Loading: 140 mg/kg orally, then 70 mg/kg every 4 hours for 17 doses (total 72-hour course)
Timing and efficacy: NAC is most effective when started within 8–10 hours of ingestion — efficacy is nearly 100% in preventing hepatotoxicity in this window. Efficacy declines progressively beyond 10 hours but NAC is still given up to 24 hours and even later in cases with established hepatic injury (it improves hepatic blood flow and function independently). There is no contraindication to starting NAC empirically if the history is uncertain — delay is always more harmful than empirical treatment.
Adverse effects of NAC (IV): Anaphylactoid reactions (urticaria, bronchospasm) occur in 5–15% of cases, usually during the loading infusion; treat with antihistamine and slow the infusion. Rarely severe — true anaphylaxis is uncommon.
Step 4 — Supportive care for hepatic failure:
- IV glucose (prevent hypoglycaemia — hepatic gluconeogenesis fails)
- Fresh frozen plasma (FFP) or vitamin K for coagulopathy
- Lactulose for hepatic encephalopathy
- Renal replacement therapy if hepatorenal syndrome develops
- Consider liver transplantation assessment for King's College criteria (persistent pH <7.3, INR >6.5, creatinine >300 µmol/L, Grade III/IV encephalopathy)
SELF-CHECK
A 14-year-old girl, weight 50 kg, is brought in 5 hours after ingesting 15 tablets of paracetamol 500 mg (total 7,500 mg = 150 mg/kg). Her plasma paracetamol level at 5 hours is 120 µg/mL, which plots above the Rumack-Matthew treatment line. She appears well — no vomiting, no abdominal pain. What is the correct management?
A. Observe for 12 hours; start NAC only if she develops symptoms of liver injury
B. Start NAC immediately — the nomogram result, not clinical appearance, determines treatment
C. Discharge with instructions to return if vomiting or jaundice develops
D. Repeat plasma paracetamol level in 4 hours before deciding on NAC
Reveal Answer
Answer: B. Start NAC immediately — the nomogram result, not clinical appearance, determines treatment
NAC must be started immediately based on the nomogram result — a plasma level above the treatment line at 5 hours indicates significant hepatotoxicity risk regardless of clinical appearance. This patient is in Phase I or early Phase II (0–24 hours): she looks well precisely because hepatic injury has not yet caused symptoms. Waiting for symptoms means waiting until Phase III hepatic failure, by which time the NAC window has significantly narrowed. The ingested dose (150 mg/kg) equals the toxic threshold and the nomogram level confirms treatment is needed. Start IV NAC loading dose (150 mg/kg over 1 hour) now. Activated charcoal is not indicated — >1 hour has passed since ingestion.
Self-Assessment: Paracetamol Poisoning
Use these questions to consolidate your understanding of paracetamol poisoning from mechanism through management. This topic bridges basic science (hepatic metabolism, glutathione biochemistry) and acute clinical management (nomogram interpretation, NAC protocol). The critical clinical skill is recognising that normal appearance in the first 72 hours does NOT mean safety — it means the window for effective treatment is still open and must not be missed. A student who understands the four-phase clinical pattern and the biochemical basis of NAPQI toxicity will make the correct management decisions under the time pressure of an emergency consultation, without needing to recall a memorised list of steps. Paracetamol poisoning is unique in that the basic science is directly actionable — knowing why the nomogram uses a 4-hour level, why NAC works, and why Phase II is deceptive are not academic facts but the operational reasons behind every management decision.
Provided image
Key concepts to verify:
1. Why does paracetamol cause liver injury specifically (not kidney or cardiac injury) as its primary target?
2. At what dose (mg/kg) is paracetamol toxic in children, and what determines individual susceptibility at that dose?
3. Why does the clinical presentation in Phases I and II NOT correlate with the severity of hepatic injury?
4. What does a plasma paracetamol level drawn at 3 hours post-ingestion tell you, and what does it NOT tell you?
5. What are the two mechanisms by which NAC prevents hepatotoxicity?
6. What clinical and biochemical criteria would prompt consideration of liver transplantation?
Self-check questions:
Q1: A child ingested paracetamol 18 hours ago. Her ALT is 3× upper limit of normal. Is it too late to give NAC?
→ No. While NAC is most effective within 8–10 hours, it is still indicated at 18 hours and even beyond in patients with evidence of evolving hepatotoxicity (rising transaminases). NAC improves hepatic blood flow and has antioxidant effects independent of glutathione replenishment. Start immediately.
Q2: Why is a plasma paracetamol level drawn at 2 hours not interpretable on the Rumack-Matthew nomogram?
→ Absorption may be incomplete at 2 hours; the level does not reflect the maximum blood concentration and cannot be meaningfully compared to the nomogram treatment line (validated for 4+ hours post-ingestion).
Q3: Which hepatic zone is most affected by NAPQI-mediated necrosis, and why?
→ Zone 3 (centrilobular/perivenular) — highest CYP2E1 concentration, lowest oxygen tension, most susceptible to oxidative mitochondrial injury.