Page 18 of 28
PE6.9-10 | Adolescent Friendly Health Services — SDL Guide
Learning Objectives
- Explain the objectives and functions of Adolescent Friendly Health Services (AFHS) and Adolescent Friendly Health Clinics (AFHC) in India
- Describe the structure and key components of the Rashtriya Kishor Swasthya Karyakram (RKSK) programme
- State the referral criteria from primary-level adolescent health services to higher levels of care
- Relate the clinical experience of a visit to an adolescent clinic to the programmatic framework of AFHS
INSTRUCTIONS
Adolescent health problems in India are substantial but largely invisible within conventional healthcare systems designed for children or adults. The creation of Adolescent Friendly Health Services (AFHS) and their Indian implementation under RKSK represents a deliberate public health response to this gap. As a future physician, understanding this system — its objectives, its structure, and the criteria that determine when to refer within it — is essential both for competent clinical practice and for meaningful participation in India's public health machinery. This module also prepares you for the PE6.10 clinic visit, helping you observe and interpret what you see with a structured framework.
References
- Ghai Essential Pediatrics, 9th Ed, Ch 7 (Adolescent Health) (textbook)
- RKSK Operational Guidelines, MoHFW India, 2014 (revised) (guideline)
- WHO Quality Assessment Guidebook for Adolescent Friendly Health Services, 2009 (guideline)
- National Health Mission — WIFS Programme Guidelines, MoHFW India (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 16-year-old girl walks into a general outpatient department complaining of irregular periods and low mood. The busy OPD doctor sees her for three minutes, prescribes iron tablets, and asks her to return in a month. She never comes back. Six months later she is brought to the emergency department with severe anaemia and depression. Somewhere in the system, a dedicated adolescent health service existed that could have provided her confidential counselling, nutritional supplementation, mental health screening, and coordinated follow-up — but she never reached it. What is this service, what does it offer, and what should have triggered her referral?
WHY THIS MATTERS
India has over 253 million adolescents — the largest adolescent population in the world. Yet adolescents access health services at lower rates than any other age group, largely because conventional facilities feel unwelcoming, judgmental, and non-confidential. The Adolescent Friendly Health Services (AFHS) framework, and its Indian operational form under RKSK, was created specifically to close this gap. Understanding AFHS is not merely academic: every physician in India will encounter adolescent patients in their practice, and knowing how to connect them to the right service tier — and when to refer upward — directly impacts outcomes for one of the most underserved demographic groups. Competency PE6.10 requires you to actually visit an adolescent clinic; this module provides the conceptual lens through which to make that visit meaningful.
RECALL
Before proceeding, recall the following:
- Adolescence = 10–19 years (WHO). The leading health burdens include anaemia, malnutrition, mental health disorders, substance use, and reproductive health risks.
- National Health Mission (NHM) is the umbrella programme under which RKSK and other reproductive and child health initiatives operate. The three-tier health system (Sub-Centre → PHC → CHC → District Hospital) provides the delivery infrastructure.
- HEEADSSS screening and the structured adolescent health checkup (PE6.8) are the clinical activities performed within AFHS settings — you studied these in the preceding SDL.
- WIFS (Weekly Iron and Folic Acid Supplementation) is a school-based intervention targeting adolescent anaemia — it will be detailed in this module as a key RKSK component.
Orientation: Why Adolescent-Friendly Services Exist
Adolescent Friendly Health Services (AFHS) emerged as a global concept in the 1990s when WHO documented that adolescents, despite a high burden of preventable health problems, were consistently underusing existing health facilities. Research identified a set of structural and attitudinal barriers that drove this under-utilisation: lack of privacy and confidentiality, judgmental provider attitudes, inaccessible hours and locations, costs, and services designed exclusively for younger children or adults. Adolescents who experienced any of these barriers were significantly less likely to return for care, even for serious problems.
In India, the magnitude of adolescent health need amplifies this problem. Nationally, approximately 56% of adolescent girls have anaemia; the prevalence of underweight is 40-45% in out-of-school adolescent girls; suicide is among the top five causes of death in the 15-24 age group; and first experience of tobacco or alcohol typically occurs before age 18. These are problems that respond to early identification and counselling — precisely what a conventional OPD is not designed to deliver.
The philosophical shift underlying AFHS is that adolescents have rights as health consumers — the right to confidentiality, to age-appropriate information, to services that respect their developing autonomy, and to non-judgmental care. This is not merely a quality-of-care aspiration; it is grounded in the United Nations Convention on the Rights of the Child (CRC) and India's own National Youth Policy. The practical implication is that designing a health service for adolescents requires deliberately building in the features that make it usable and acceptable to this age group — not simply pointing them to the existing paediatric or adult OPD.
In India, this conceptual foundation was operationalised through RKSK (launched 2014), which replaced the earlier Adolescent Reproductive and Sexual Health (ARSH) strategy with a broader, six-domain framework.
RKSK Programme Architecture
Structure and Magnitude of Adolescent Health Services in India
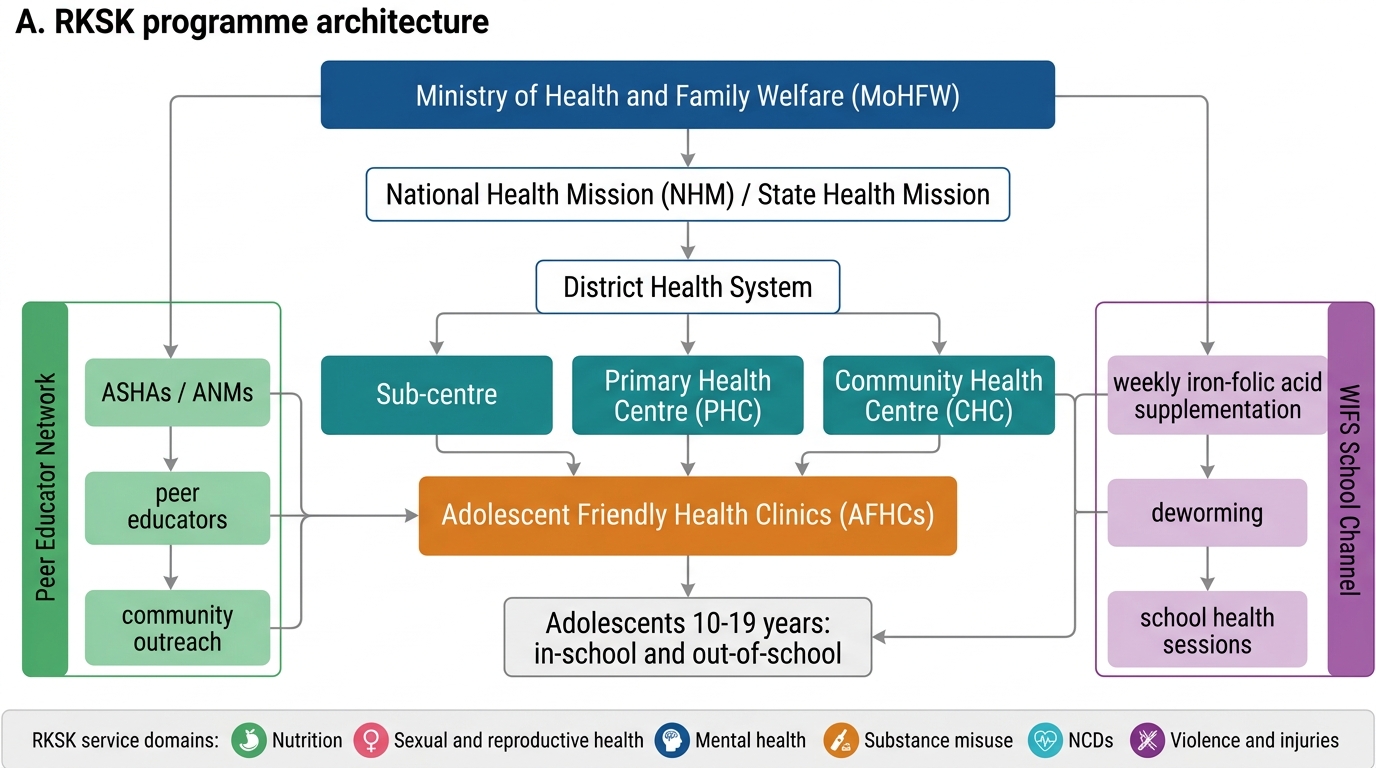
RKSK (Rashtriya Kishor Swasthya Karyakram) was launched by the Ministry of Health and Family Welfare in 2014 as India's comprehensive national adolescent health programme, replacing the earlier ARSH (Adolescent Reproductive and Sexual Health) strategy which had a narrower focus restricted to reproductive health. RKSK deliberately broadened the mandate to encompass the full spectrum of adolescent health determinants, recognising that a programme limited to SRH would miss the majority of the adolescent health burden — anaemia, mental health, substance use, NCDs, and violence. It covers both in-school and out-of-school adolescents aged 10–19 years, with a particular focus on the rural poor, marginalised communities, and out-of-school girls who are most vulnerable. RKSK is implemented through the National Health Mission infrastructure and represents the most significant structural investment India has made in adolescent health services at scale, with over 9,000 dedicated Adolescent Friendly Health Clinics established across the country.
RKSK operates across six strategic domains:
1. Nutrition — addressing adolescent anaemia, underweight, and overweight/obesity
2. Sexual and reproductive health — education, contraception access, prevention of early marriage and pregnancy
3. Substance use — prevention and brief intervention for tobacco, alcohol, and drugs
4. Non-communicable diseases — early identification of hypertension, diabetes risk, obesity
5. Mental health — screening, counselling, and referral for depression, anxiety, self-harm
6. Injuries and violence — road safety, prevention of sexual and physical violence
Key delivery components of RKSK:
- Adolescent Friendly Health Clinics (AFHC): These are dedicated weekly or bi-weekly clinics set up within existing Sub-Centres, PHCs, and CHCs, staffed by a trained RKSK counsellor. The AFHC is the primary clinical service point — it is where the adolescent health checkup, HEEADSSS screening, and first-line interventions are delivered. There are over 9,000 AFHCs operational across India (NHM progress reports).
- Peer Educator Programme: RKSK trains adolescent volunteers (Peer Educators / Saathiyas) who serve as information providers and health promoters within their communities and schools. Each peer educator is trained in basic health promotion across all six RKSK domains.
- WIFS (Weekly Iron and Folic Acid Supplementation): A school-based intervention delivering 1 tablet weekly (containing 100 mg elemental iron + 500 mcg folic acid) to all adolescent girls and boys in government schools. Out-of-school adolescents receive WIFS through AWC/health sub-centres. WIFS is a cornerstone of RKSK's nutrition strategy for anaemia reduction.
- Menstrual Hygiene Scheme (Kishori Scheme in some states): Subsidised sanitary napkins distributed through ASHA workers to rural adolescent girls, linked to menstrual hygiene education.
- School Health Programme: Annual health check-up of school-going children and adolescents, integrated with RKSK outreach.
The geographic scale is significant: RKSK targets approximately 253 million adolescents across all states and UTs, with priority districts identified under NHM for intensified implementation.
SELF-CHECK
A 15-year-old out-of-school girl in a rural area has been identified as anaemic during a community health survey. Under RKSK, which intervention should she receive as first-line nutritional support?
A. Daily iron-folic acid tablet for 3 months
B. Weekly iron-folic acid supplementation (WIFS) — 100 mg iron + 500 mcg folic acid once weekly
C. Intravenous iron infusion at the district hospital
D. Monthly iron syrup dispensed by the ASHA worker
Reveal Answer
Answer: B. Weekly iron-folic acid supplementation (WIFS) — 100 mg iron + 500 mcg folic acid once weekly
Under the RKSK WIFS programme, the standard intervention for adolescents is weekly supplementation — one tablet per week containing 100 mg elemental iron and 500 mcg folic acid. This applies to both in-school and out-of-school adolescents; out-of-school adolescents receive WIFS through AWCs or health sub-centres. Daily supplementation is the regimen for frank iron-deficiency anaemia treatment (which requires a clinical diagnosis and therapeutic dosing), not routine supplementation. IV iron and monthly syrup are not WIFS programme components.
Objectives and Functions of AFHS and AFHC
The objectives of AFHS, as defined by WHO (Quality Assessment Guidebook, 2009) and adopted in the RKSK framework, centre on making health services genuinely usable by adolescents. The core objective is to improve adolescent health outcomes by removing the structural, attitudinal, and knowledge barriers that prevent adolescents from accessing and utilising health services. Translated into specific programmatic goals, AFHS aims to: (a) provide age-appropriate, comprehensive health information and services to all adolescents regardless of sex, age, socioeconomic status, or marital status; (b) maintain confidentiality and respect adolescent autonomy while ensuring safety; (c) train healthcare providers in adolescent-sensitive communication; and (d) integrate community outreach with facility-based care.
Provided image
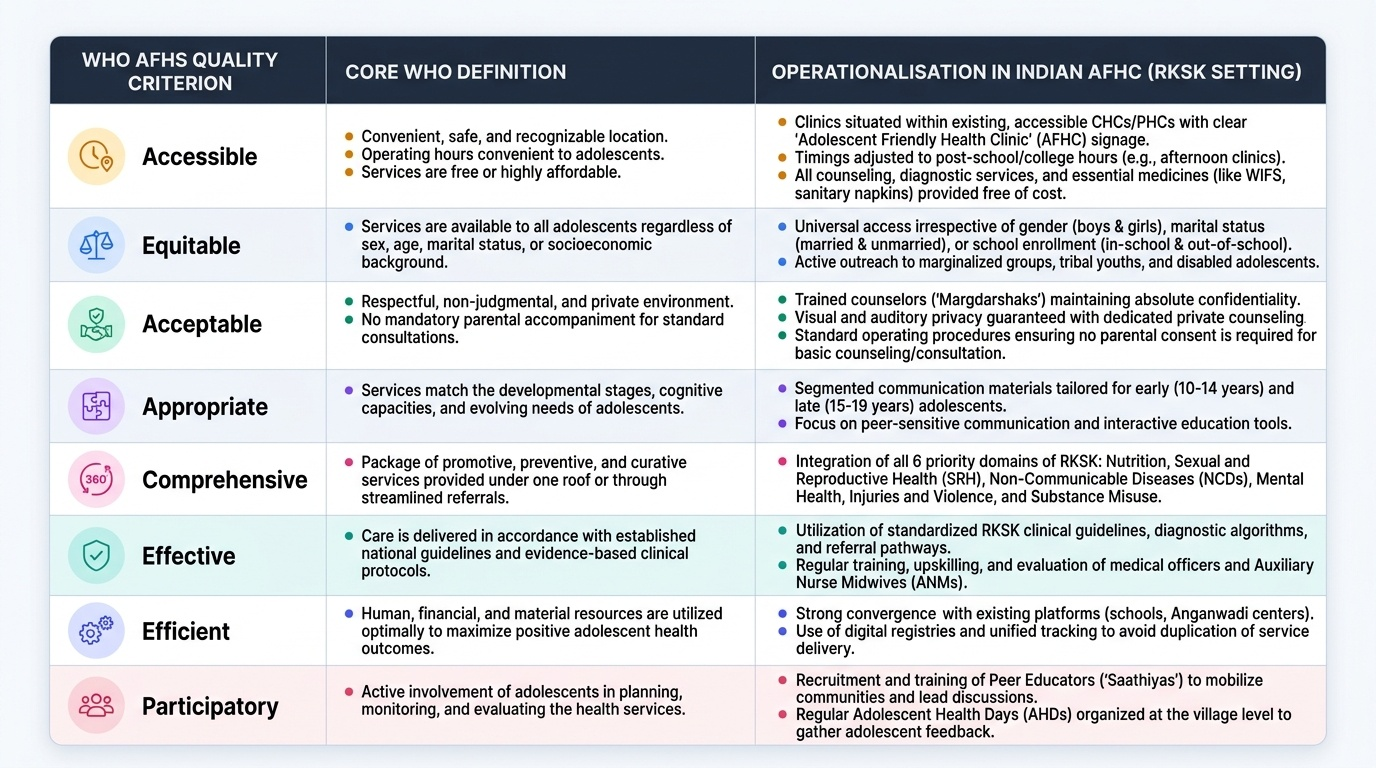
The WHO 8 Quality Criteria for AFHS define what an adolescent-friendly facility must achieve. An AFHC in India should meet all eight:
- Accessible — convenient location, opening hours that accommodate school schedules, affordable or free services
- Equitable — services available to ALL adolescents (boys and girls, married and unmarried, in-school and out-of-school, disabled, marginalised groups)
- Acceptable — non-judgmental staff attitude, privacy, no mandatory parental accompaniment for most services
- Appropriate — services matched to developmental stage and evidence-based; peer-sensitive communication
- Comprehensive — covers all six RKSK domains (nutrition, SRH, mental health, NCDs, substance use, violence)
- Effective — delivers measurable health outcomes; uses evidence-based interventions
- Efficient — minimal waiting time; well-coordinated referral; no unnecessary procedures
- Youth-friendly environment — physical setting designed to be welcoming; waiting area distinct from adult/paediatric areas where possible
Specific functions of an AFHC:
| Service Category | Function | Target Group |
|---|---|---|
| Health assessment | Adolescent health checkup + HEEADSSS + growth monitoring | All 10–19 yr |
| Nutrition | WIFS distribution; nutrition counselling; BMI assessment | All; esp. girls |
| Mental health | Psychosocial counselling; referral for depression/self-harm | All |
| SRH | Menstrual hygiene counselling; contraception information; STI screening | Girls/sexually active |
| Substance use | Brief advice; de-addiction referral | All |
| NCDs | BP screening; blood sugar if risk factors; obesity counselling | All |
| Immunisation | Td booster; HPV where available | Age-appropriate |
| Referral | Identify + refer complex cases per referral criteria | As clinically indicated |
The trained RKSK counsellor is the backbone of the AFHC. Unlike a nurse or doctor, the counsellor is specifically trained in adolescent communication, psychosocial screening, and the six RKSK domains. The counsellor conducts the HEEADSSS screen, provides counselling, and escalates to the AFHC medical officer or refers externally when criteria are met.
CLINICAL PEARL
Clinical Pearl — The 'Acceptable' Criterion Is the Most Commonly Violated:
Research on adolescent health service utilisation consistently identifies provider attitude as the single most powerful predictor of whether an adolescent returns for care. An AFHC that is accessible, well-stocked, and technically competent will fail if the counsellor or doctor is dismissive, moralistic, or breaks confidentiality. In your clinical practice, the 'acceptable' WHO criterion translates to one practical rule: always see the adolescent alone for at least part of the consultation, maintain a neutral face and voice regardless of what they disclose, and never share their information with parents unless safety demands it. The first visit sets the template for all future help-seeking behaviour.