Page 19 of 28
PE6.9-10 | Adolescent Friendly Health Services — SDL Guide (Part 2)
Referral Criteria from AFHC to Higher Care
Referral from an AFHC to a higher level of care (PHC medical officer → CHC/district hospital specialist → tertiary centre) is indicated when the presenting problem exceeds the scope or resources of first-line adolescent health services. Understanding the referral criteria is a mandatory competency because the AFHC counsellor — who is not a physician — depends on clear operational guidelines to make this decision safely, and the receiving physician at the higher level needs to know what to expect in a referred adolescent. The guiding principle of RKSK referral is: intervene at the lowest appropriate level; escalate when safety, diagnosis, or treatment complexity demands it.
The RKSK operational guidelines define the following categories of referral criteria:
Immediate/emergency referral (same day, to district hospital/emergency):
• Suicidal ideation with plan and intent — direct to mental health emergency
• Acute severe anaemia (haemoglobin < 7 g/dL with symptoms) — to inpatient care
• Suspected sexual assault (within 72 hours) — to designated OSCC (One Stop Crisis Centre) for POCSO-mandated response, medical examination, forensic evidence, legal aid
• Acute psychosis or severe depressive episode — to psychiatric facility
• Signs of domestic violence with immediate safety risk — to social welfare + police referral
• Severe acute malnutrition in adolescent — to NRC/paediatric unit
Scheduled/non-urgent referral (within 1–2 weeks, to CHC/district hospital):
• Haemoglobin 7–10 g/dL not responding to 3 months of WIFS — to check for malabsorption, haemoglobinopathy, chronic infection
• Irregular menstrual cycles beyond 2 years of menarche — to gynaecology/paediatric endocrinology
• Suspected precocious or delayed puberty — to paediatric endocrinology (bone age, LH/FSH)
• Hypertension (confirmed on two readings ≥130/80) — to internal medicine
• Suspected thyroid disorder (clinical goitre, symptoms) — to paediatrics/endocrinology for TSH
• Depression not responding to counselling — to psychiatry
• Substance dependence — to de-addiction centre
• STI symptoms (vaginal discharge, genital ulcer) — to gynaecology/dermatology
• Obesity with metabolic complications — to paediatrics/dietitian
Documentation of referral:
All referrals must be documented in the RKSK register with: date, referral destination, reason for referral, and follow-up plan. The adolescent should be given a referral slip with the above information, and the receiving facility should send a feedback note to the AFHC. This feedback loop is often the weakest link in the system — as a physician at the receiving end, complete the feedback to enable continuity of care.
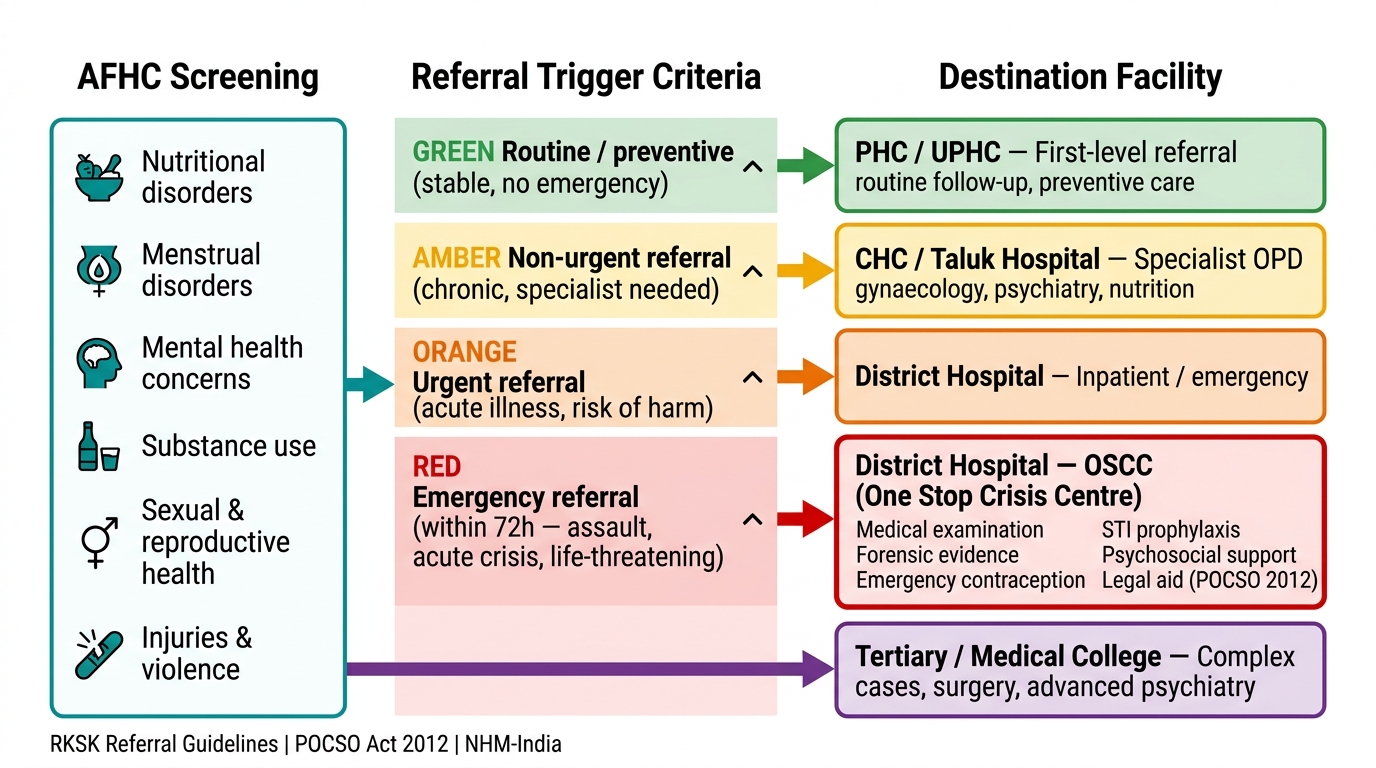
AFHC Referral Pathway — Adolescent Conditions to Facility Levels
SELF-CHECK
A 17-year-old girl visits the AFHC and discloses that she was sexually assaulted two days ago. She does not want her parents to know. What is the most appropriate immediate action?
A. Counsel her about STI prevention and schedule a follow-up in two weeks
B. Inform her parents because she is a minor and cannot consent to care independently
C. Refer her immediately to the designated One Stop Crisis Centre (OSCC) for medical examination, forensic evidence collection, and legal aid under POCSO Act 2012
D. Advise her to report to the police station and come back after the FIR is registered
Reveal Answer
Answer: C. Refer her immediately to the designated One Stop Crisis Centre (OSCC) for medical examination, forensic evidence collection, and legal aid under POCSO Act 2012
Sexual assault of a person below 18 years is a POCSO Act 2012 offence, and mandatory reporting is legally required. An acute assault within 72 hours constitutes an emergency referral criterion under RKSK guidelines. The One Stop Crisis Centre (OSCC), co-located at district hospitals, is the designated facility providing integrated medical examination (including forensic evidence collection), emergency contraception, STI prophylaxis, psychosocial support, and legal aid under one roof. Waiting two weeks would lose forensic evidence and the window for emergency contraception (~72 hours). Parental consent is not required for emergency medical treatment of a minor in an acute crisis situation; confidentiality obligations do not override the mandatory POCSO reporting requirement.
Self-Assessment
The questions below consolidate your understanding of AFHS objectives, RKSK programme structure, and referral criteria. They also prepare you to observe and critically evaluate the adolescent clinic during your PE6.10 visit — when you attend the clinic, try to identify how many of the WHO 8 quality criteria you can observe being met or unmet, and bring your observations to the post-visit debrief. A structured reflective observation is worth more educationally than a passive visit. Consider keeping a brief field note during the visit: what services are offered, who staffs the clinic, what the physical environment communicates to an adolescent, and whether you witness a referral being made. These observations, framed against the RKSK operational guidelines you have studied here, form the basis of your competency demonstration for PE6.10.
- Name the six strategic domains of RKSK and give one specific service under each domain.
- What is WIFS? State the dose and the target population under RKSK.
- List all eight WHO quality criteria for AFHS and identify which criterion is most commonly violated in practice.
- Under RKSK referral criteria, which three conditions constitute immediate/emergency referral from an AFHC?
- A 15-year-old boy presents to AFHC with persistent low mood for 6 weeks, not improving with two counselling sessions. What is the appropriate management?
- During your PE6.10 clinic visit, you observe a doctor speaking to an adolescent girl in the presence of her mother throughout the consultation. Which AFHS quality criterion is being violated?
- Distinguish between RKSK and AFHC — what is the relationship between the two?