Page 5 of 28
PE6.{4,7,12} | Adolescent Sexuality — SDL Guide
Learning Objectives
- Describe adolescent sexuality, sexual identity formation, and common sexual health problems including STIs, unintended pregnancy, and menstrual concerns
- Enumerate the prevalence of sexual abuse and drug abuse among Indian adolescents, and recognise the clinical and behavioural indicators of each
- Describe the mandatory reporting obligations under the POCSO Act 2012 when sexual abuse of a child is suspected
- Apply the principles of confidentiality in adolescent clinical encounters, including the conditions under which it may be breached
- Demonstrate the HEEADSSS approach to probing sexuality and substance use domains in a clinical consultation
INSTRUCTIONS
Sexual health and substance use are among the most sensitive — and most clinically important — topics in adolescent medicine. They are also the topics most likely to remain unprobed in routine consultations because clinicians feel uncomfortable, lack the framework, or assume adolescents will not disclose. This module equips you with the clinical knowledge and practical consultation skills to recognise when an adolescent is at risk, how to conduct a non-judgmental, confidential assessment, and what your legal obligations are when sexual abuse is suspected. These competencies directly protect adolescent patients from harm.
References
- Ghai Essential Pediatrics, 9th ed., Chapter on Adolescent Health (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Adolescent Medicine — Sexual Behaviour and Substance Abuse (textbook)
- POCSO Act 2012 — Protection of Children from Sexual Offences, Ministry of Women and Child Development, India (law)
- IAP Standard Treatment Guidelines — Adolescent Health, 2022 (guideline)
- NFHS-5 (2019–21), International Institute for Population Sciences, Mumbai (data)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 16-year-old girl comes to the adolescent health clinic alone. She is visibly anxious and reluctant to speak. After you explain that the consultation is confidential, she discloses that she has been sexually active for six months with a 19-year-old boyfriend, has missed her last menstrual period, and has a vaginal discharge she is embarrassed about. She adds, almost as an afterthought, that she has been drinking alcohol on weekends to cope with stress. You have 15 minutes, no prior record, and a waiting room full of patients. How do you proceed — and what are your obligations if she further discloses that the sexual activity was not fully consensual?
WHY THIS MATTERS
Sexual and reproductive health problems account for a disproportionate share of adolescent morbidity in India and globally. According to NFHS-5 (2019–21), India's adolescent birth rate remains 6.8 per 1,000 women aged 15–19 — a substantial figure representing preventable adolescent pregnancies. STI rates in adolescents are under-reported but estimated to be among the highest of any age group, driven by inconsistent condom use, multiple or concurrent partnerships, and barriers to healthcare access. Drug use initiation is virtually universal during adolescence: tobacco and inhalants are the most common entry points, with alcohol and cannabis following. The POCSO Act 2012 mandates that any person — including a treating physician — who suspects sexual abuse of a person under 18 must report it to the police or Special Juvenile Police Unit (SJPU) within 24 hours, with criminal liability for non-reporting. This module teaches you the clinical knowledge and the consultation framework to address these realities competently and ethically.
RECALL
Recall from the previous SDL (Adolescent Development) the HEEADSSS psychosocial assessment framework, particularly the S (Sexuality) and D (Drugs) domains — these are the most sensitive domains and are introduced after rapport is established. Recall that confidentiality is the foundation of the adolescent clinical encounter, but has defined limits when harm is imminent. Recall from your Microbiology and Dermatology exposure the common presentations of gonorrhoea (urethral/vaginal discharge), chlamydia (often asymptomatic), syphilis (primary chancre), and HIV (variable, often asymptomatic at this age). These pathogens are directly relevant to the clinical assessment of a sexually active adolescent.
Why Adolescent Sexual and Drug Health Matters Clinically
Adolescent sexual and reproductive health, and adolescent substance use, are the two domains of adolescent medicine most likely to go unaddressed in a routine paediatric consultation — partly because they are perceived as adult concerns, and partly because clinicians lack confidence in probing these sensitive areas. Yet these are precisely the areas where early identification and brief intervention have the greatest impact on lifelong outcomes.
The epidemiological case is compelling. India's National Family Health Survey (NFHS-5, 2019–21) documents an adolescent birth rate of 6.8 per 1,000 women aged 15–19, reflecting ongoing adolescent sexual activity without reliable contraception. STIs — including chlamydial infection, gonorrhoea, syphilis, and HIV — are disproportionately prevalent in adolescents and young adults globally, and are largely asymptomatic in their early phases, making active probing essential. For substance use, the Global School-Based Student Health Survey data and NFHS data consistently show that tobacco use initiation occurs predominantly between 10 and 15 years, with alcohol and cannabis following in mid-to-late adolescence. The pattern of sequential substance initiation (tobacco or inhalants → alcohol → cannabis → other substances) means that identifying early-stage use creates a window for effective intervention before dependence develops.
For the clinician, the POCSO Act 2012 (Protection of Children from Sexual Offences) creates a mandatory duty to report suspected child sexual abuse — and ignorance of this law is not a defence. Every paediatric and general practitioner must know the provisions of Section 19, which requires any person (including a doctor) to report suspected sexual abuse of a person under 18 to the SJPU or local police within 24 hours, regardless of whether the child or parent consents to the report.
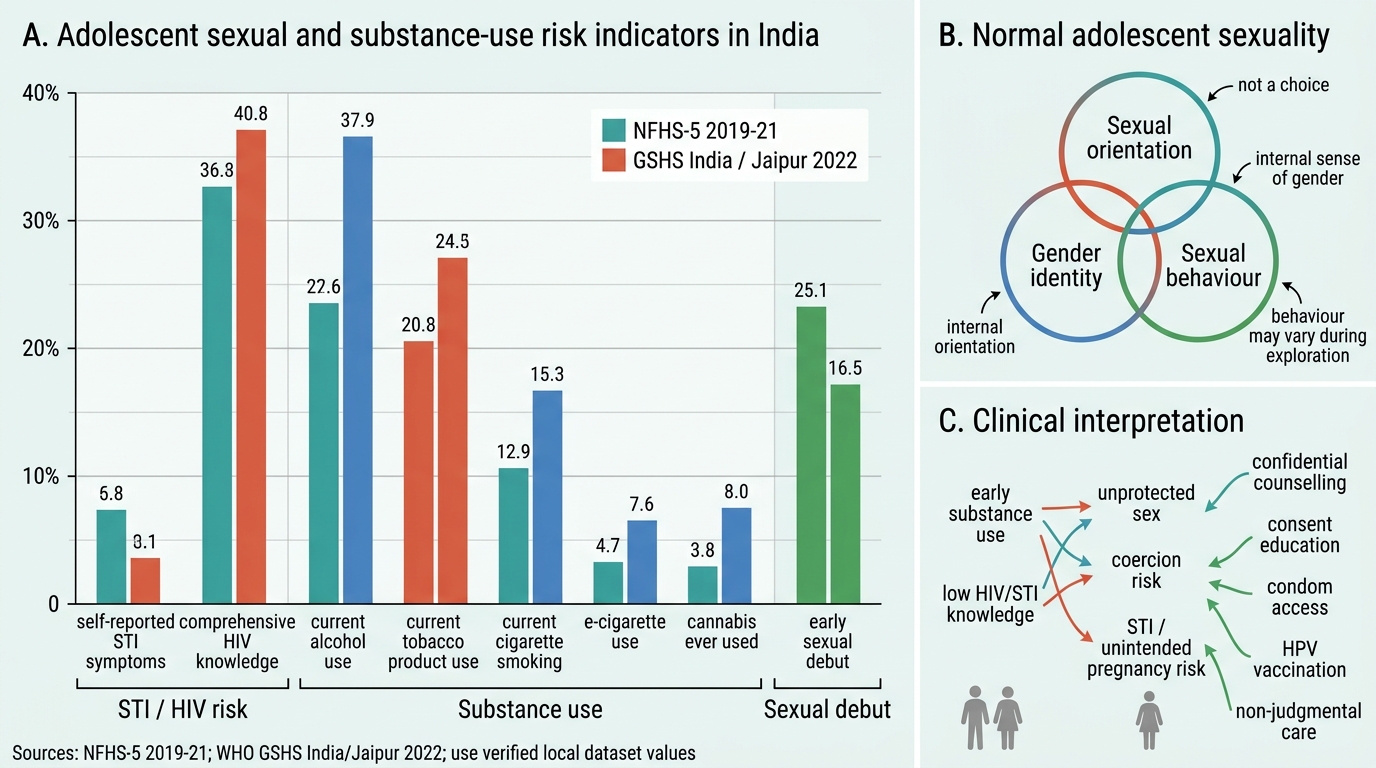
Adolescent Sexual Health Risk Indicators in India
Normal Sexual Development and Identity in Adolescence
Understanding what is normal in adolescent sexuality is the prerequisite for recognising what is pathological. Sexual development in adolescence encompasses three conceptually distinct but interrelated domains: sexual orientation, gender identity, and sexual behaviour.
Sexual orientation refers to the pattern of enduring emotional, romantic, and sexual attraction to others — whether to persons of the same sex (homosexual), the opposite sex (heterosexual), or both (bisexual). Adolescence is the period during which most individuals first become consciously aware of their sexual orientation; for many, this is a period of exploration and uncertainty before a stable orientation is recognised. Sexual orientation is not a choice, and the scientific and medical consensus is that it is a stable characteristic determined by a combination of biological and developmental factors. Attempts to change sexual orientation ('conversion therapy') are ethically condemned and have been shown to cause psychological harm without changing orientation.
Gender identity refers to a person's internal sense of their own gender — whether they feel themselves to be male, female, non-binary, or another gender identity. This is distinct from biological sex (chromosomal, gonadal, phenotypic) and from sexual orientation. Gender dysphoria is significant distress arising from a mismatch between one's gender identity and biological sex. It is a recognised clinical condition (DSM-5/ICD-11) but is not a pathological state of the person — the distress arises from the mismatch and from social stigma, not from the identity itself. Adolescents with gender dysphoria or non-heterosexual orientation are at significantly elevated risk of depression, self-harm, and suicidal ideation — making a non-judgmental, affirming clinical approach ethically and clinically essential.
Sexual behaviour in adolescence includes a spectrum from sexual curiosity and exploration to sexual activity. Masturbation is universal and a normal part of sexual development; it carries no physical harm. The clinical concern arises when sexual behaviour creates health risk (STIs, pregnancy), involves coercion (abuse), or occurs in developmentally inappropriate contexts (very young children, significant age differentials).
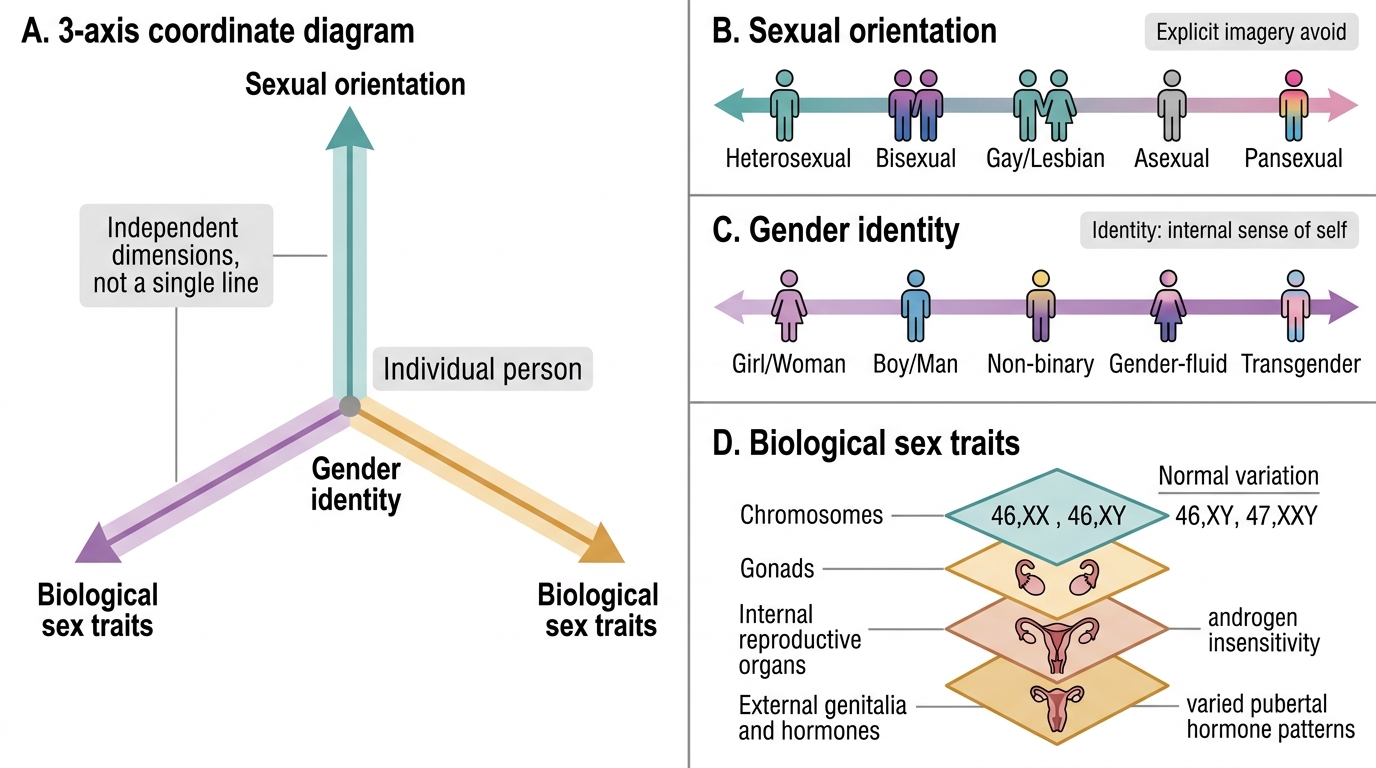
Independent Axes of Sexual Orientation, Gender Identity, and Biological Sex
Common Sexual Health Problems in Adolescents
Adolescents who are sexually active face a distinct set of reproductive health risks that arise from the intersection of biological vulnerability, inconsistent contraceptive use, and difficulty accessing confidential healthcare. The clinician who sees adolescents must be prepared to address these problems within a routine encounter.
Sexually transmitted infections (STIs) are disproportionately prevalent in adolescents. The biological vulnerability is real: cervical ectopy (extension of the columnar epithelium onto the ectocervix), present in most adolescent girls, increases susceptibility to Chlamydia trachomatis and Neisseria gonorrhoeae infection. Adolescent girls are also more likely to have coercive or partner-age-asymmetric sexual encounters that limit their negotiating power for condom use. Chlamydia is the most common bacterial STI — often asymptomatic but causing fallopian tube damage and infertility if untreated. Gonorrhoea presents with mucopurulent discharge (cervical/urethral) but is also frequently asymptomatic in girls. Syphilis presents in primary stage as a painless genital ulcer (chancre). HIV testing and counselling should be offered to any adolescent with STI risk. Management in adolescent settings typically follows syndromic management guidelines (for discharge, ulcer, or lower abdominal pain syndromes) with combined antibiotic cover, STI partner notification, and consistent condom promotion as the cornerstone of prevention and dual protection against both STI and pregnancy.
Unintended adolescent pregnancy is the consequence of inconsistent contraception combined with sexual activity. It carries elevated risks compared to adult pregnancy: anaemia, pre-eclampsia, preterm birth, low birth weight, maternal morbidity, and educational/economic disruption. Contraception counselling for sexually active adolescents should centre on condoms (dual protection) as the first-line recommendation; long-acting reversible contraceptives (implants, IUDs) are acceptable options where compliance with daily oral pills is uncertain. Emergency contraception (levonorgestrel 1.5 mg within 72 hours of unprotected intercourse) should be known to the clinician even if its discussion with young adolescents requires careful contextualisation.
Dysmenorrhoea and menstrual irregularity are common presenting complaints. Primary dysmenorrhoea (no pelvic pathology) affects up to 50–80% of adolescent girls and is the leading cause of school absenteeism. First-line treatment: NSAIDs (mefenamic acid 500 mg TDS, ibuprofen 400 mg TDS), initiated at the onset of menstrual flow. Irregular cycles for up to 2 years after menarche are normal; beyond this window, investigation for PCOS, thyroid disorders, or eating-disorder-associated amenorrhoea is warranted.
| Common Adolescent STI | Pathogen | Key Clinical Feature | First-line Treatment |
|---|---|---|---|
| Chlamydial cervicitis | Chlamydia trachomatis | Often asymptomatic; mucopurulent discharge | Doxycycline 100 mg BD × 7 days or azithromycin 1 g single dose |
| Gonorrhoea | Neisseria gonorrhoeae | Urethral/cervical discharge, dysuria | Ceftriaxone 500 mg IM single dose + treat for chlamydia |
| Primary syphilis | Treponema pallidum | Painless genital ulcer (chancre) | Benzathine penicillin 2.4 MU IM single dose |
| Genital herpes | HSV-2 (usually) | Painful vesicles/ulcers, dysuria | Aciclovir 400 mg TDS × 7-10 days |
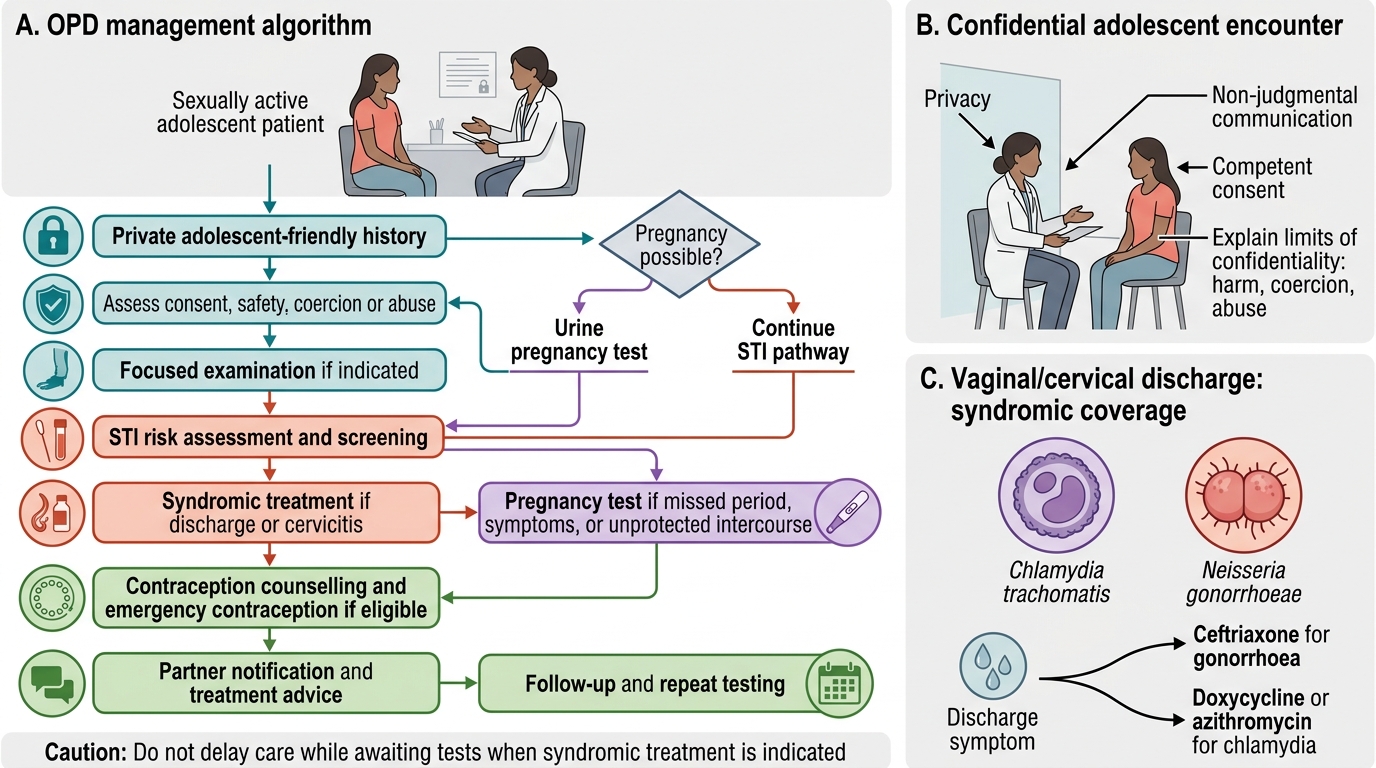
OPD Algorithm for Sexually Active Adolescents
SELF-CHECK
A 17-year-old girl presents with a 1-week history of vaginal discharge. She is sexually active with one partner. She asks you to keep this consultation private from her parents. The syndromic management of her likely STI involves treatment for which TWO pathogens?
A. Treponema pallidum and HSV-2
B. Chlamydia trachomatis and Neisseria gonorrhoeae
C. Gardnerella vaginalis and Trichomonas vaginalis
D. Herpes simplex virus and Candida albicans
Reveal Answer
Answer: B. Chlamydia trachomatis and Neisseria gonorrhoeae
Mucopurulent cervical or vaginal discharge in a sexually active adolescent is managed syndromically with coverage for BOTH Chlamydia trachomatis (most common bacterial STI, often asymptomatic) AND Neisseria gonorrhoeae (co-infection common). The standard syndromic approach provides dual coverage: ceftriaxone (for gonorrhoea) plus doxycycline or azithromycin (for chlamydia). Treating both simultaneously prevents treatment failure even when diagnostic tests are not immediately available. The patient's request for confidentiality is appropriate and should be respected — she is 17 years old, Gillick-competent to consent to her own treatment, and confidentiality is the cornerstone of the adolescent health encounter.