Page 6 of 28
PE6.{4,7,12} | Adolescent Sexuality — SDL Guide (Part 2)
Sexual Abuse in Adolescents — Recognition and Mandatory Reporting
Sexual abuse is any sexual act involving a person under 18 years of age that is non-consensual, coercive, or involves a person in a position of power or trust over the child, or where the child is below the legal age of consent (in India, 18 years). It is critical to understand that under the POCSO Act 2012, any sexual contact with a person under 18 years is an offence — the law does not recognise consent from a person under 18 for sexual activity. This differs from the clinical and ethical reality that adolescents develop sexual agency and may engage in consensual sexual activity — the clinician must navigate this tension carefully.
Prevalence in India: sexual abuse of children and adolescents is substantially under-reported. The Ministry of Women and Child Development report (2007) found that 53% of children surveyed reported some form of sexual abuse, with boys and girls equally affected. The perpetrator is most often known to the child — a family member, family friend, neighbour, or person in authority. Stranger-perpetrated abuse, while it occurs, is not the typical pattern.
Recognition — behavioural indicators: Adolescents who are being sexually abused may present with:
- Unexplained changes in school performance or attendance
- Withdrawal, depression, self-harm, or suicidal ideation
- Age-inappropriate sexual knowledge or sexualised behaviour
- Avoidance of a specific person or situation
- Substance use as a coping mechanism
- Running away from home
- Vague somatic complaints — abdominal pain, headache, sleep disturbance — without organic explanation
Recognition — clinical/physical indicators: Physical findings in sexual abuse may include genital or anal injuries, STIs in a pre-pubertal child or in a child who denies sexual activity, pregnancy in a young adolescent, or signs of chronic trauma. However, the absence of physical findings does NOT exclude sexual abuse — most cases leave no physical trace. Clinical examination in suspected sexual abuse should be performed only by a trained forensic clinician in an appropriate setting, never in a rushed OPD encounter.
POCSO Act 2012 — mandatory reporting provisions: Section 19 of the POCSO Act 2012 mandates that ANY PERSON who suspects that a child (under 18 years) has been or is being sexually abused MUST report it to the Special Juvenile Police Unit (SJPU) or the local police. This duty applies to healthcare providers, teachers, and any other person. Key provisions:
- The report must be made within 24 hours of gaining the information
- No consent from the child or parent is required to make the report — it is a MANDATORY duty
- Failure to report is a criminal offence under Section 21 of the POCSO Act, punishable with imprisonment up to 6 months and/or fine
- Medical examination of the child should follow Section 27 provisions (conducted within 24 hours; female child examined by a female doctor; guardian/trusted adult present)
- The child's identity must be protected — no disclosure to media
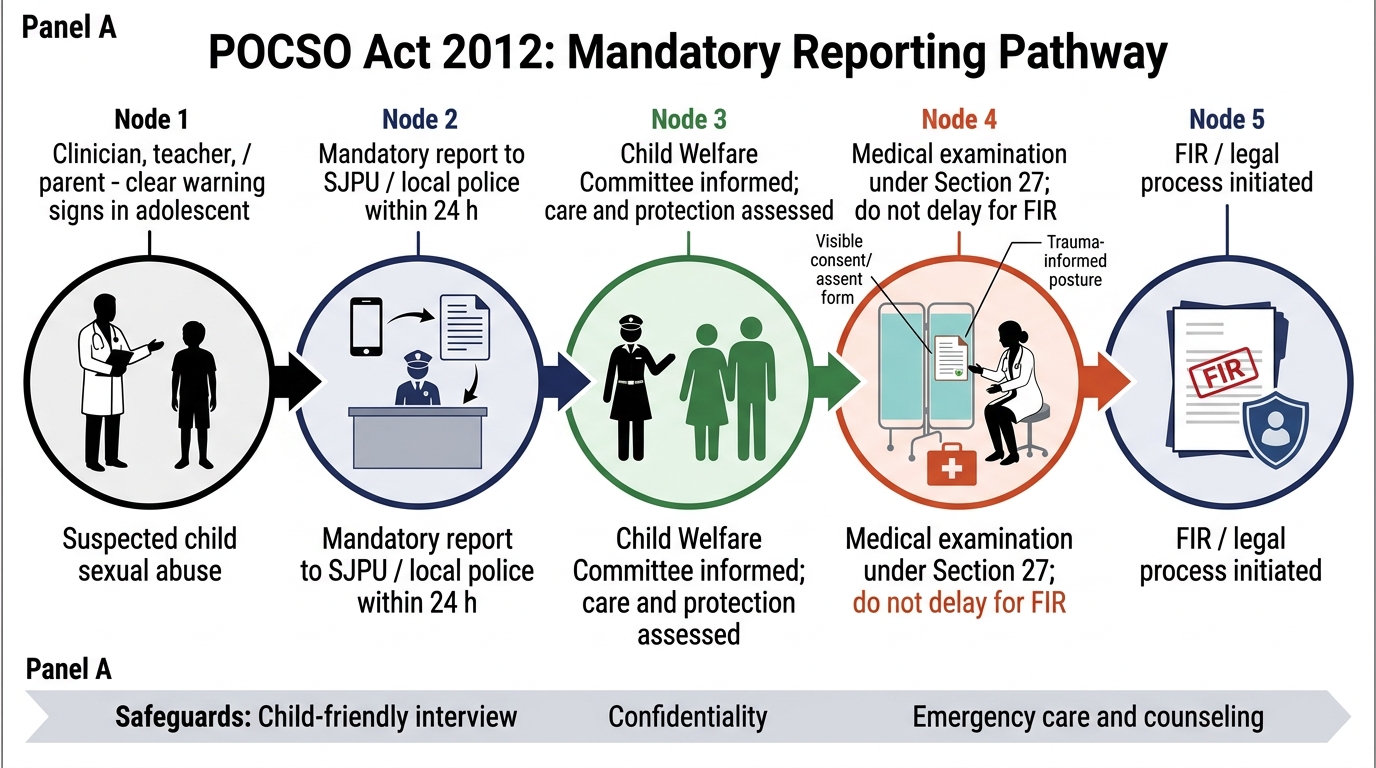
POCSO Act Mandatory Reporting Pathway
Drug Abuse in Adolescents — Prevalence and Recognition
Substance use in adolescence follows a well-documented sequential initiation pattern that begins during the school years and escalates through mid-adolescence if not interrupted. Understanding the pattern, the prevalence data, and the brief screening tools is essential for any clinician seeing adolescents.
Prevalence in India: the Global School-Based Student Health Survey and various state-level studies consistently document that tobacco use (cigarettes, bidis, smokeless tobacco — gutka/pan masala) is the most common entry-point substance, with initiation rates of 15–25% among secondary-school adolescents in some states. Inhalant abuse — sniffing whitener, petrol, typewriter correction fluid, adhesive solvents — is particularly prevalent among street-based, out-of-school, and homeless adolescents; it carries the risk of sudden sniffing death syndrome (ventricular fibrillation from cardiac sensitisation by volatile hydrocarbons). Alcohol is the second most commonly used substance; cannabis (marijuana/ganja/charas) follows in late adolescence. Use of sedative-hypnotics, opioids, and stimulants occurs but is less common in this age group.
Risk factors for adolescent substance use include: peer substance use (the strongest predictor), family history of substance use disorder, mental health comorbidities (especially depression and anxiety), history of trauma or abuse, academic failure, low parental monitoring, and access to substances. The HEEADSSS D (Drugs) domain probes these domains directly in the clinical encounter.
The CRAFFT screening tool is a validated 6-item brief screening instrument specifically designed and validated for adolescent substance use. The acronym encodes the key questions:
| Letter | Question |
|---|---|
| C | Have you ever ridden in a CAR driven by someone (or yourself) who was high or had been using alcohol/drugs? |
| R | Do you ever use alcohol or drugs to RELAX, feel better about yourself, or fit in? |
| A | Do you ever use alcohol/drugs while you are by yourself, ALONE? |
| F | Do your family or FRIENDS ever tell you that you should cut down on your drinking or drug use? |
| F | Do you ever FORGET things you did while using alcohol or drugs? |
| T | Have you ever gotten into TROUBLE while using alcohol or drugs? |
A score of 2 or more is a positive screen, indicating the need for a brief intervention or referral. The CRAFFT is non-judgmental in phrasing, quick to administer, and can follow naturally from the HEEADSSS D domain questions.
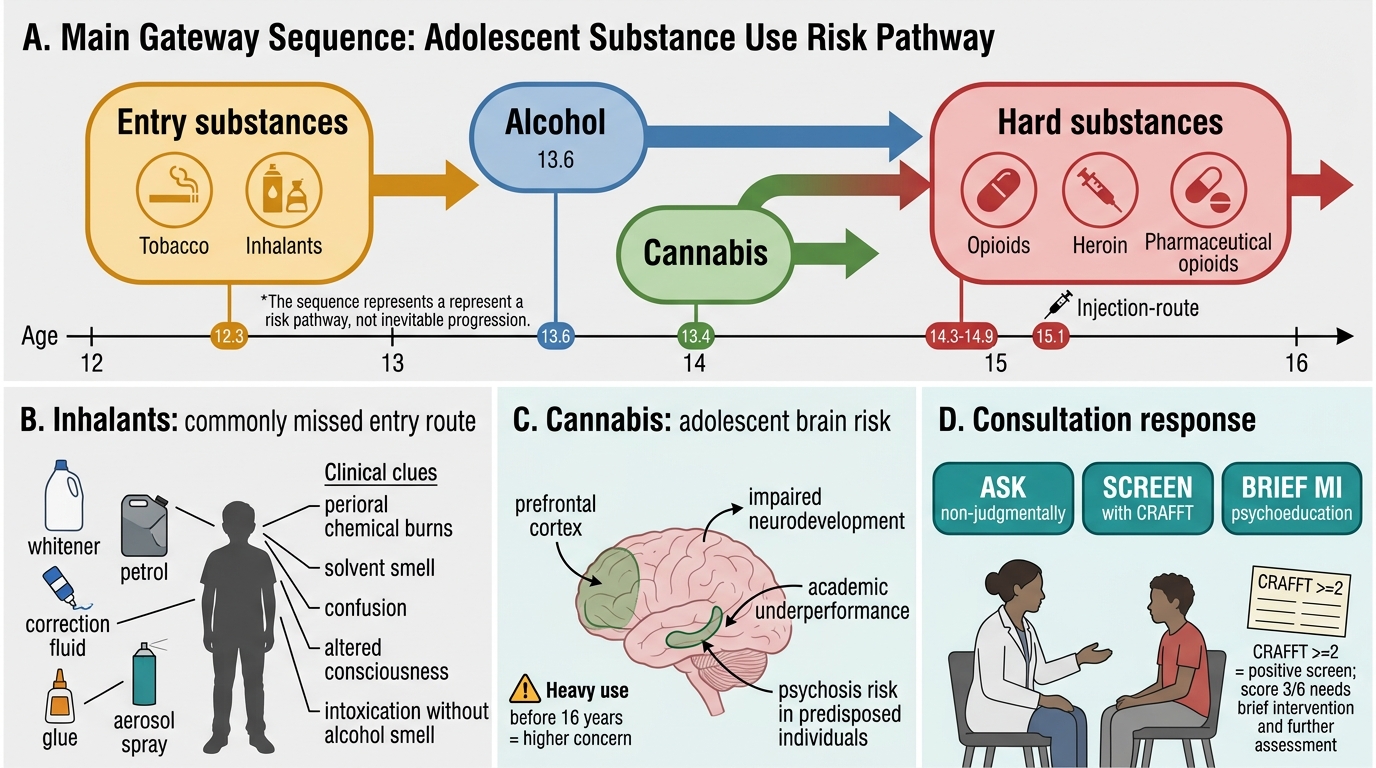
Gateway Sequence of Adolescent Substance Use in India
CLINICAL PEARL
Two clinical traps in adolescent substance consultation: (1) Inhalant abuse is often missed because caregivers and clinicians do not think to ask, and the substances (whitener, petrol, correction fluid) are household items. Clues include: perioral or perinasal chemical burns or dermatitis, a persistent solvent smell on breath or clothing, unexplained altered consciousness or confusion, frequent mild intoxication with no alcohol smell. Street children and out-of-school adolescents are at highest risk. (2) Cannabis is perceived as harmless by many adolescents and families — but regular cannabis use during adolescence (especially heavy use before age 16) is associated with impaired neurodevelopment, earlier onset of psychotic disorders in genetically predisposed individuals, and academic underperformance. Brief non-judgmental psychoeducation about this risk, delivered in a motivational-interviewing style, is more effective than moralising.
SELF-CHECK
A 15-year-old boy is brought to you by his school counsellor who suspects drug use. The boy admits to occasional alcohol use but denies all other substance use. On CRAFFT screening, he scores 3/6. What does this score indicate?
A. CRAFFT score 3/6 is below the positive threshold of 5 — no intervention needed
B. CRAFFT score ≥2 is a positive screen indicating the need for brief intervention or referral to substance use services
C. CRAFFT is only valid for adults aged 18 and above — do not interpret in adolescents
D. A score of 3 means the patient has a formal substance use disorder and requires residential treatment
Reveal Answer
Answer: B. CRAFFT score ≥2 is a positive screen indicating the need for brief intervention or referral to substance use services
The CRAFFT (Car, Relax, Alone, Forget, Friends, Trouble) is a validated 6-item screening tool specifically designed for adolescents. A score of 2 or more is the positive threshold indicating the need for brief motivational intervention and, if indicated, referral to adolescent substance use services. It does NOT diagnose a substance use disorder — that requires fuller assessment. CRAFFT was originally validated for adolescents and is the recommended tool in this age group; it is not an adult tool. A score of 3 is above the threshold and warrants brief intervention at minimum.
Confidentiality in Adolescent Care — Ethics and Practice
Confidentiality is not simply a courtesy extended to adolescent patients — it is a clinically necessary condition for adolescents to disclose sensitive health concerns. Studies consistently show that adolescents who believe their disclosures will be shared with parents without their consent are less likely to seek care for sexual health, substance use, and mental health concerns. The clinician who cannot guarantee confidentiality will therefore systematically miss the problems they most need to detect.
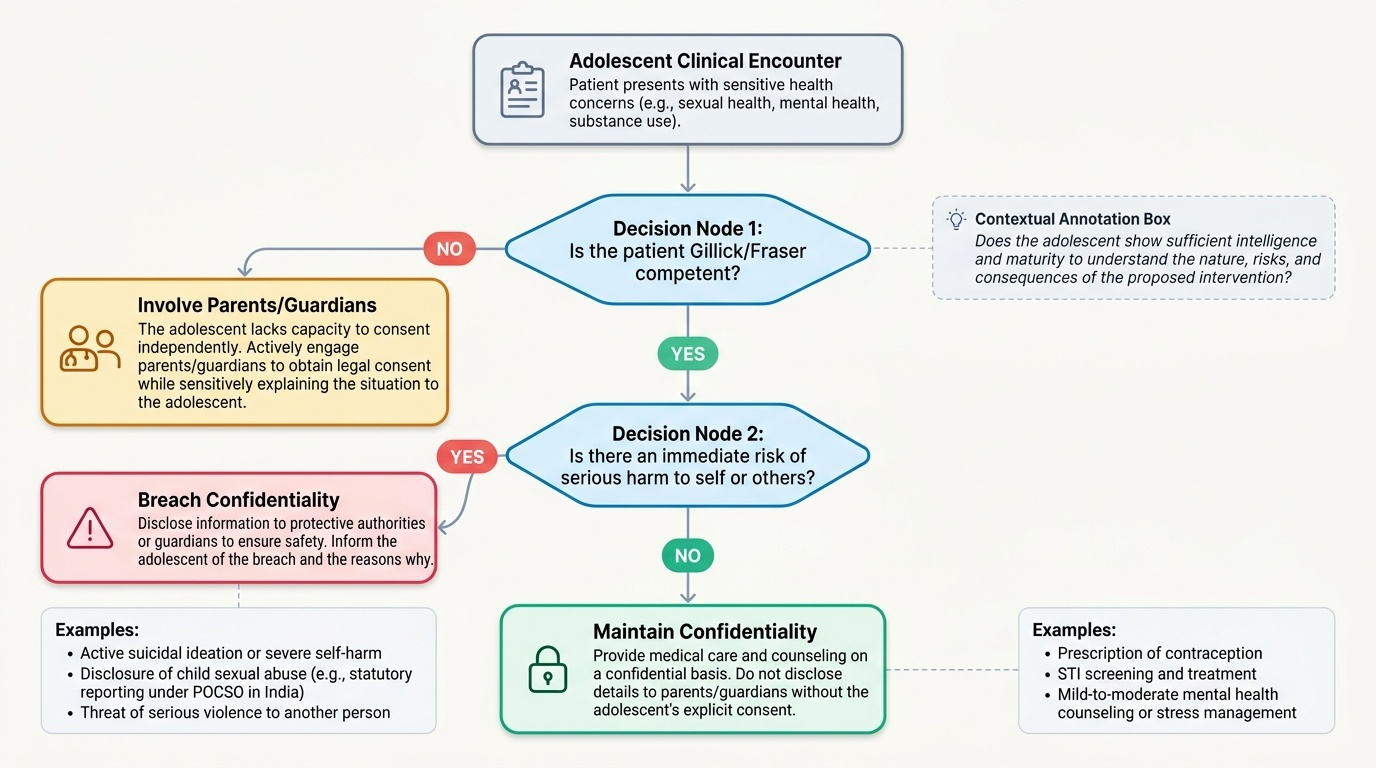
Provided image
The ethical and legal framework for adolescent confidentiality in India draws on two principles. First, the principle of evolving capacity (reflected in the UNCRC): as adolescents mature, they acquire increasing capacity to make autonomous healthcare decisions, and the law should respect this growing competence. Second, the Gillick/Fraser competence principle (widely applied internationally and increasingly influential in Indian medical ethics): an adolescent who can demonstrate sufficient intelligence and maturity to understand the nature and consequences of a proposed intervention has the competence to consent to that intervention without parental involvement, even if they are under 18. In Indian practice, while there is no single statute governing adolescent consent across all healthcare domains, the general principle is that a clinician may provide care to a Gillick-competent adolescent (typically mid-to-late adolescence) on a confidential basis for issues such as contraception, STI treatment, and mental health counselling.
The LIMITS of confidentiality are critical and must be communicated to the adolescent at the start of every consultation. Confidentiality CAN be breached — and in some cases MUST be breached — when:
1. The patient discloses imminent risk of harm to themselves (suicidal ideation with plan/intent, self-harm at dangerous severity)
2. The patient discloses being a victim of sexual abuse — the POCSO Act 2012 mandates reporting regardless of the adolescent's wishes; the duty is non-negotiable
3. The patient poses a risk of serious harm to another person
The clinician's opening statement should set this framework honestly: "What you share with me today is private — I won't tell your parents without your permission. However, if I am worried that you are in serious danger, I may need to involve others to keep you safe. Is that OK?"
Practical consultation approach for confidential adolescent encounters:
1. Separate the adolescent from the parent for at least part of the consultation
2. State the confidentiality agreement and its limits clearly at the outset
3. Use HEEADSSS to structure the psychosocial screen systematically
4. Ask open, non-judgmental questions — avoid clinical language that creates shame
5. Document findings appropriately; in cases of suspected abuse, document thoroughly and contemporaneously