Page 1 of 21
PE7.{4-5,7} | Breastfeeding Technique and Support Systems — SDL Guide
Learning Objectives
- Observe a breastfeeding session and identify whether attachment and positioning are correct or incorrect (PE7.4 — S/P level)
- Enumerate the WHO-UNICEF Baby-Friendly Hospital Initiative (BFHI) and the Ten Steps to Successful Breastfeeding (PE7.5)
- Describe the role of BPNI (Breastfeeding Promotion Network of India) and explain how to participate in World Breastfeeding Week advocacy at your institution (PE7.7)
INSTRUCTIONS
Breastfeeding is the single most effective preventive intervention in neonatal and infant health. Despite universal awareness of its benefits, breastfeeding failure in India most often results from a correctable skills gap — poor attachment technique — rather than an inherent inability to lactate. As a final-year intern you will counsel mothers at the bedside, reinforce correct latch, identify technique problems before they become abandonment, and participate in institutional and community advocacy through BFHI certification and World Breastfeeding Week. This module builds the knowledge and observational skills you need to do all of that from Day 1 of your posting.
References
- Ghai Essential Pediatrics, 9th ed., Ch 8 (Feeding and Nutrition) (textbook)
- WHO/UNICEF: Protecting, Promoting and Supporting Breastfeeding in Health Facilities Providing Maternity and Newborn Services (2017 — Ten Steps) (guideline)
- IAP Guidelines on Infant and Young Child Feeding (IYCF), 2022 (guideline)
- BPNI (Breastfeeding Promotion Network of India) — www.bpni.org (resource)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are on your first day of the newborn nursery posting. A primigravida mother in the postnatal ward is in tears: her three-day-old infant has not fed well since birth, her nipples are cracked and bleeding, and the baby has lost more than 10% of birth weight. The midwife suggests formula supplementation. Before you reach for a feeding bottle, you ask to watch the mother attempt a feed. You observe that the infant's mouth is barely open, the lower lip is tucked inward, and the chin is not touching the breast. No audible swallowing is heard. Within five minutes of repositioning the infant and correcting the latch — mouth wide, lower lip out, chin to breast — the baby settles into rhythmic, audible suck-swallow cycles and feeds contentedly for 15 minutes. The mother's tears turn to relief. The 'formula problem' was a technique problem all along.
WHY THIS MATTERS
India bears one of the world's highest burdens of preventable neonatal and infant mortality, and poor breastfeeding practices are a major contributor. The Lancet Breastfeeding Series (2016) estimated that scaled-up breastfeeding could prevent approximately 820,000 child deaths annually worldwide. In India, the National Family Health Survey (NFHS-5, 2019–21) shows that only about 63.7% of infants under 6 months are exclusively breastfed — well below the WHO recommendation of exclusive breastfeeding for the first 6 months. The gap between intent and practice is almost always bridged by skilled counselling and early technique correction, not by lactation biology alone. As an intern in postnatal wards, well-baby clinics, SNCU, and IMNCI settings, you will be among the first health workers a mother encounters. Your ability to observe a feed, identify a latch problem, and counsel confidently is a direct determinant of whether a mother breastfeeds successfully. This module covers the technique knowledge (PE7.4) and the public-health infrastructure (PE7.5, PE7.7) that together make that counselling effective.
RECALL
Before we build new knowledge, recall what you already know from your Year-1 pharmacology and physiology postings and from the broader PE7 cluster:
- Suckling and rooting reflexes (from PY AN Year 1): the neonate's rooting reflex turns the head toward tactile stimulation of the cheek; the suckling reflex is triggered by contact with the palate — both are present from 34 weeks gestation and are necessary prerequisites for effective breastfeeding.
- Exclusive breastfeeding definition and benefits (PE7.1–PE7.3): breast milk is the only feed — no water, formula, or other liquids — for the first 6 months; benefits include passive immunity (secretory IgA, lysozyme, lactoferrin), optimal nutrition, reduced diarrhoea and pneumonia, and reduced SIDS risk.
- OG17 link (Obstetrics): If you have attended the OG17 module on lactation, you will have seen the hormonal basis of milk secretion and ejection from the obstetric perspective. We revisit that basis here with a clinical emphasis on its implications for technique.
- IMNCI danger signs (from PE-skills IMNCI module): an infant who is not breastfeeding at all in the first days of life is a 'not able to breastfeed' danger sign requiring urgent assessment — technique correction is the first step before escalation.
Clinical Importance of Breastfeeding Support
The clinical case for active, skilled breastfeeding support is stronger than any pharmacological or surgical intervention in the early neonatal period. Breast milk delivers passive immunity in the form of secretory IgA, which coats the intestinal mucosa and resists colonisation by enteropathogens; lactoferrin, which sequesters iron from bacterial pathogens; lysozyme and oligosaccharides that selectively promote the growth of beneficial Lactobacillus and Bifidobacterium species. These biological properties are not replicated by any formula, regardless of marketing claims. Beyond infection protection, breastfeeding provides optimal macronutrient composition that changes dynamically across feeds and across weeks — colostrum is high in protein and immunoglobulins; mature milk shifts toward a higher fat content in the hindmilk that drives satiety and energy intake. At the population level, every one-percentage-point increase in exclusive breastfeeding rates in a community translates to measurable reductions in hospitalisation for diarrhoea and pneumonia — the two leading killers of Indian children under 5.
For the intern and house officer, the clinical indication for breastfeeding support is any one of the following presentations encountered in the postnatal ward, newborn nursery, or outpatient well-baby clinic: (a) a mother reporting pain or cracked nipples (almost always a latch problem, not a skin problem); (b) a baby who feeds for very short bursts and then cries again within minutes (suggestive of ineffective milk transfer due to poor attachment); (c) a neonatal weight loss exceeding 7–10% of birth weight by day 3–4 without an organic cause; (d) a primigravida mother expressing anxiety about 'insufficient milk' in the first 72 hours (almost always perception, not reality, when technique is correct); (e) any mother who has not fed her infant in the previous 3 hours in a postnatal ward — a missed feeding window that needs assessment, not assumption.
The rationale for the skills arc in this module is precise: PE7.4 is coded S/P (Skill / Participate), meaning the student should be able to observe a breastfeeding session and distinguish correct from incorrect technique — this is an observational and counselling skill, not a performance skill. You are not independently counselling a mother as a primary clinician in your intern year; you are participating under supervision, reinforcing the correct messages, and identifying when to escalate to a lactation counsellor or senior colleague.
Prolactin-Oxytocin Axis in Breastfeeding
Lactation Physiology and Governing Principles
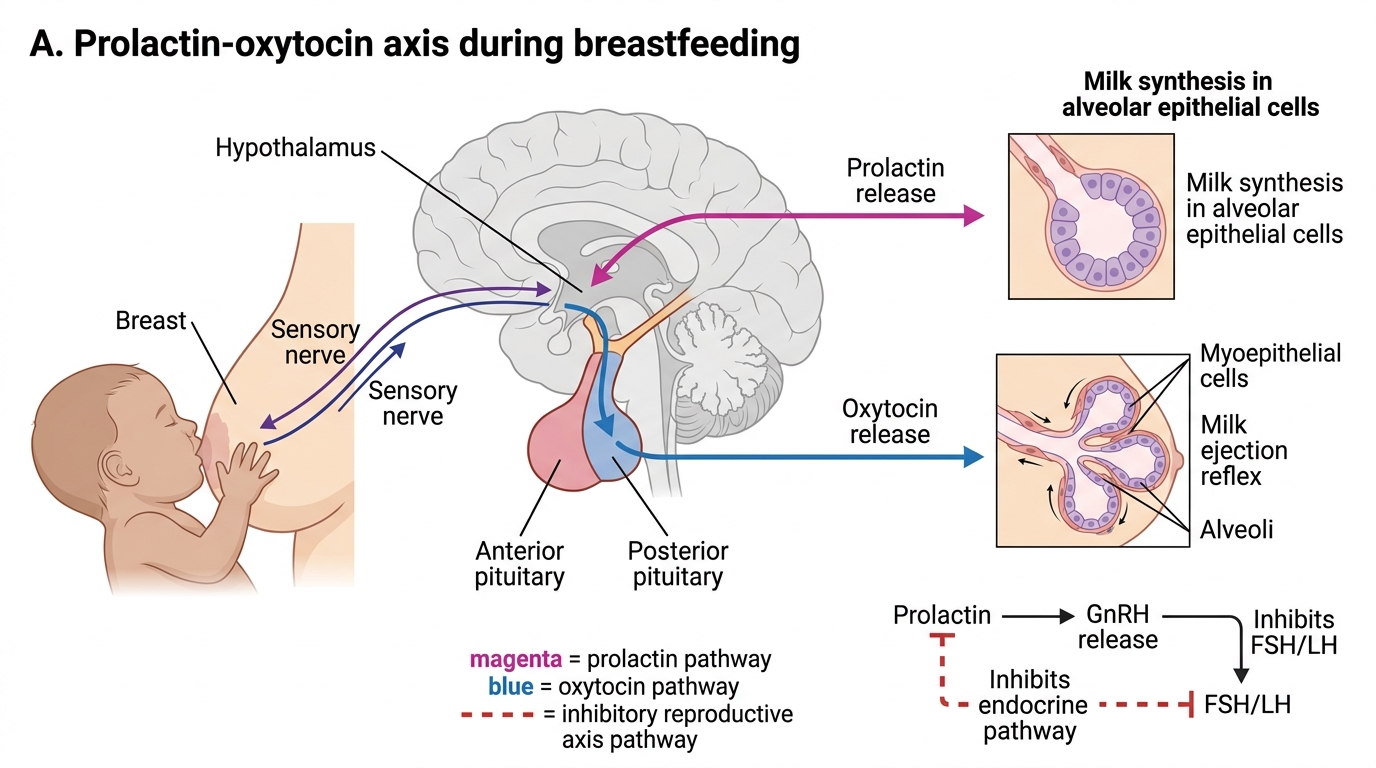
A thorough understanding of the hormonal basis of lactation is not merely academic — it directly explains why the technique matters and what happens physiologically when technique is wrong. The two key hormones are prolactin and oxytocin, and they serve completely different but complementary functions in breastfeeding.
Prolactin is secreted by the anterior pituitary gland in response to nipple stimulation by the suckling infant. Prolactin drives lactogenesis — the synthesis of milk within the alveolar epithelial cells of the breast. Crucially, prolactin operates on a supply-demand principle: the more frequently and effectively the infant suckles, the more prolactin is released, and the more milk is synthesised. This is why the prescription for perceived low milk supply is almost always increased feeding frequency, not supplementation. During pregnancy, high levels of oestrogen and progesterone suppress prolactin activity at the breast level despite adequate prolactin secretion — this is why colostrum is only released after placental delivery (the fall in progesterone removes this block, a process called lactogenesis II). Prolactin levels are highest at night, which is why night feeds are disproportionately important for establishing and maintaining milk supply in the first weeks.
Oxytocin is secreted by the posterior pituitary and is responsible for the milk ejection reflex (MER), colloquially called the 'let-down'. Oxytocin causes contraction of the myoepithelial cells surrounding the alveoli, which propels synthesised milk into the lactiferous sinuses and ducts, making it available at the nipple. The MER can be conditioned — a mother may experience let-down at the sound of her baby's cry or even when thinking about feeding — and it can be inhibited by pain, stress, and anxiety, which is why a calm, private, comfortable feeding environment is not a luxury but a physiological requirement. When the MER is inhibited (e.g., due to cracked nipples causing feed-associated pain), the infant may suckle vigorously but receive very little milk — a cycle that worsens nipple trauma and eventually leads to abandonment.
The anatomical basis of attachment is equally important. The nipple alone contains approximately 15–20 lactiferous ducts that converge near the surface; the areola overlies the lactiferous sinuses that serve as milk reservoirs. For effective milk transfer, the infant must take a mouthful of both nipple and a generous portion of areola — not just the nipple tip. When only the nipple is in the mouth (shallow latch), the infant compresses the nipple tip without reaching the sinuses, milk transfer is minimal, and nipple trauma is inevitable. The physics of effective breastfeeding therefore requires the infant to (a) open the mouth wide (gape ≥120°), (b) take the breast deeply, (c) form a teat from nipple plus areola tissue, and (d) use the tongue in a wave-like peristaltic motion against the teat to extract milk.
The four key signs of correct attachment as defined by IAP/WHO are:
1. Mouth wide open (large gape)
2. Lower lip turned outward (everted, not tucked)
3. More areola visible above the upper lip than below the lower lip
4. Chin touching the breast (not a gap between chin and breast)
All four signs should be present simultaneously. Absence of any one suggests incorrect attachment, even if the other three appear correct. These four signs are the clinical checklist you apply when observing every breastfeeding session.
SELF-CHECK
A new mother reports that her baby feeds for only 5–10 minutes and then cries again within 30 minutes, repeatedly. Her nipples are sore. On observation, the infant's mouth is partly open, the lower lip is tucked inward, and the chin is 1 cm away from the breast. What is the most likely primary cause of this problem?
A. Insufficient milk production due to low prolactin levels
B. Shallow latch with the infant compressing only the nipple tip
C. Neonatal hypoglycaemia causing excessive crying
D. Tongue-tie (ankyloglossia) causing inability to suckle
Reveal Answer
Answer: B. Shallow latch with the infant compressing only the nipple tip
The history and observation describe a classic shallow-latch presentation: sore nipples (nipple trauma from compression), short and unsatisfying feeds (poor milk transfer), and the three attachment signs are wrong (mouth not wide open, lower lip tucked, chin not touching breast). Shallow latch is the most common cause and is correctable by positioning and re-latching. Low prolactin is not the diagnosis when technique has not been assessed. Hypoglycaemia is a systemic sign requiring blood glucose measurement, not suggested by this history alone. Tongue-tie is a differential for recurrent latch failure despite correct technique, but the question specifically shows correctable technique signs — rule out technique first.
Breastfeeding Positions and Attachment Technique
Correct breastfeeding technique involves two interdependent components: the position of the mother-infant dyad and the attachment of the infant to the breast. These must be optimised simultaneously — a correct position does not guarantee good attachment, and a good latch cannot be sustained in an uncomfortable position. The overarching goal of positioning is to allow the infant's face to be brought directly to the breast without straining, twisting, or compensating with abnormal jaw mechanics. When a mother and infant are positioned well, the act of latching-on becomes biomechanically natural; when position is suboptimal, the infant must compensate with jaw and tongue adjustments that inevitably produce a shallow, painful seal. There is also a physiological dimension: a mother who is hunched over, tense, or unsupported activates sympathetic tone that inhibits the oxytocin-driven milk ejection reflex, reducing milk transfer even when attachment is technically correct. Optimal positioning is therefore simultaneously a mechanical and a physiological intervention, and the first step in every breastfeeding support encounter is to assess and correct position before evaluating latch.
Positioning principles apply regardless of which hold is used. The CHINS pneumonic (used in counselling) captures the key elements:
- Chest to chest (the infant's body faces the mother's body, not the ceiling)
- Head in line with body (the infant's head is not rotated or twisted — a baby cannot swallow comfortably with a twisted neck, just as you cannot swallow with your head turned sideways)
- In close (the mother brings the baby to her breast, not her breast to the baby — which causes back pain and positional instability)
- Nose to nipple (the nose opposite the nipple at the start, so the infant reaches up and gapes to take a deep mouthful, rather than starting with the mouth already at nipple level)
- Supported (the whole of the infant's body is supported, not just the head — a dangling body weight strains the neck and breaks the seal)
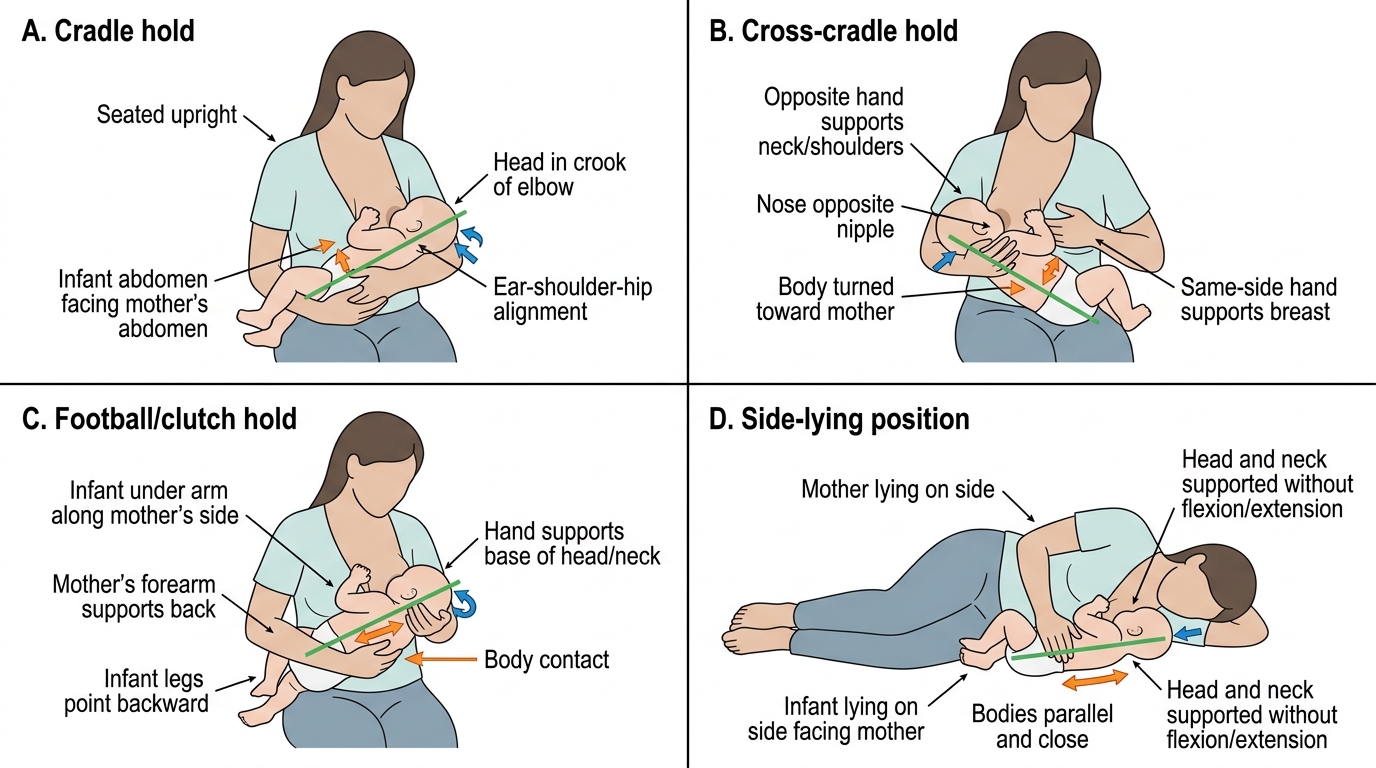
The four main holds are:
- Cradle hold: The infant's head rests in the crook of the mother's arm (on the same side as the feeding breast), body cradled along the forearm. Most natural for mothers after the first few days. Less control over the infant's head than cross-cradle.
- Cross-cradle hold: The mother's opposite arm (to the feeding breast) supports the infant's body; the same-side hand is free to support the breast ('C-hold' or 'U-hold'). Gives more control over head position — preferred in the first days and for small or premature infants.
- Football/clutch hold: The infant's body is tucked under the mother's arm on the same side as the feeding breast, legs pointing behind the mother. Useful after caesarean section (avoids wound pressure), for large breasts, for preterm twins, or for any mother with a strong MER who needs better milk-flow control.
- Side-lying hold: Mother and infant lie face-to-face. Preferred for postnatal fatigue, after perineal repair, or for night feeds. Requires care to ensure the mother does not fall asleep with the infant in the adult bed (safe sleep precautions).
Attachment (latching-on) process — step by step:
1. Position the infant CHINS (above), nose opposite nipple.
2. The mother supports her breast with four fingers below and thumb above (C-hold), keeping fingers well away from the areola.
3. The nipple gently strokes the infant's upper lip to trigger the rooting reflex and encourage a wide gape.
4. When the mouth opens widely, the mother brings the infant quickly and firmly onto the breast — moving the infant, not the breast.
5. Confirm all four signs of correct attachment (mouth wide, lower lip out, more areola above, chin touching).
6. If attachment is incorrect, break the seal gently with a clean finger inserted at the corner of the mouth, and re-latch.
Assessing a feed in progress: A correctly attached infant demonstrates rhythmic suck-swallow breathing cycles. In the first few minutes, rapid, short sucks stimulate the MER; once let-down occurs, the pattern shifts to deeper, slower sucks with visible jaw movement and audible swallowing. The mother should feel a drawing sensation (not pain); the breast should soften as the feed progresses; the infant should appear satisfied at the end and release the breast spontaneously.
Correct Breastfeeding Positions