Page 2 of 21
PE7.{4-5,7} | Breastfeeding Technique and Support Systems — SDL Guide (Part 2)
Distinguishing Correct from Incorrect Technique
The ability to reliably distinguish correct from incorrect breastfeeding technique is the core clinical skill of PE7.4, and it requires systematic, structured observation rather than relying on the mother's reported experience alone. Pain is not a normal part of breastfeeding; perceived insufficient milk is almost never a real insufficiency in the first week; frequent feeding is normal and not a sign of 'weak' milk. These misconceptions drive premature supplementation and abandonment — and correcting them begins with accurate technique assessment.
Provided image
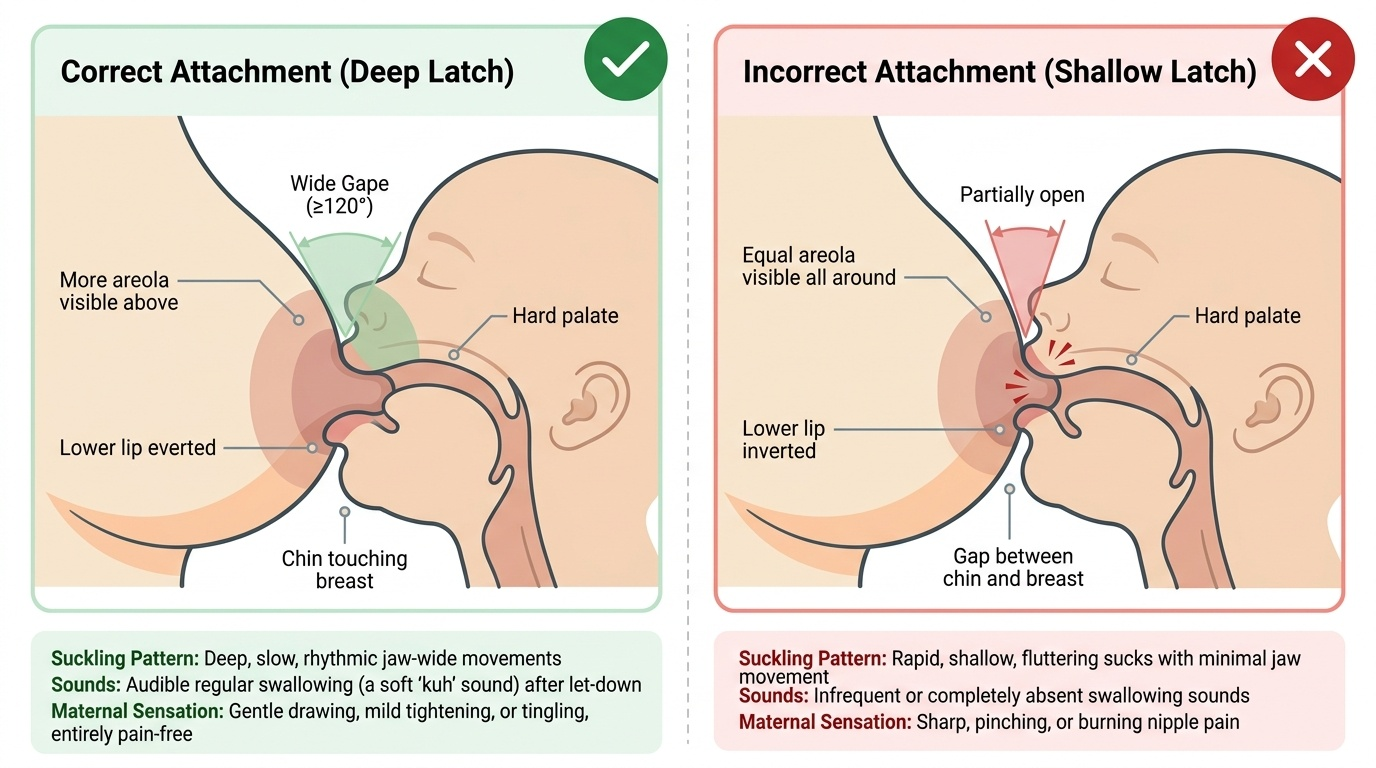
Effective vs ineffective suckling patterns: Effective suckling has a characteristic rhythm of deep, slow, jaw-wide suck-swallow-breathe cycles after the initial let-down phase. The jaw drops visibly with each suck, and audible swallowing (a soft 'kuh' sound) is heard regularly. The mother reports a drawing or tingling sensation but not sharp pain. Ineffective suckling, by contrast, is characterised by rapid, shallow sucks with minimal jaw movement, infrequent or absent audible swallowing, and feed-associated nipple pain. The infant may appear to be suckling vigorously but is primarily compressing the nipple tip rather than expressing milk from the sinuses.
Key comparison — correct vs incorrect attachment signs (apply the four signs systematically):
| Sign | Correct | Incorrect |
|---|---|---|
| Mouth opening | Wide gape (≥120°) | Partly or barely open |
| Lower lip position | Everted (turned outward) | Inverted (tucked inward) |
| Areola visibility | More areola visible above upper lip | Equal areola visible all around |
| Chin contact | Chin touching breast | Gap between chin and breast |
| Suckling sound | Audible swallowing heard | No swallowing sounds |
| Maternal sensation | Drawing/mild tightening | Sharp nipple pain |
Common problems and their technique-based causes:
| Problem | Most Likely Cause | Corrective Action |
|---|---|---|
| Cracked/bleeding nipples | Shallow latch — infant compressing nipple tip | Correct attachment; express a few drops of hind milk on nipple after feed (natural healing agent) |
| Breast engorgement | Infrequent feeding, inadequate drainage | Increase feeding frequency (8–12/day); hand expression or feeding to soften before latch if areola too tense |
| Perceived insufficient milk | Supply-demand mismatch from infrequent feeds or poor transfer | Increase frequency; confirm adequate wet nappies (6–8/day = adequate intake); avoid formula supplementation |
| Mastitis | Milk stasis from incomplete drainage ± skin entry by S. aureus | Continue breastfeeding from affected side; appropriate antibiotics (flucloxacillin or amoxicillin-clavulanate) if infective |
| Inverted or flat nipples | Nipple does not protrude at rest | Cross-cradle hold; nipple stimulation before latching; rarely requires intervention |
An important clinical rule: rule out technique before attributing breastfeeding problems to anatomy or hormones. The vast majority of breastfeeding difficulties in the first two weeks are technique-correctable. When technique has been optimised and problems persist, escalate to a trained lactation counsellor or assess for ankyloglossia (tongue-tie), maternal thyroid dysfunction, or other structural causes.
SELF-CHECK
A mother is breastfeeding and the intern observes: infant's mouth is wide open, lower lip is turned outward, chin is touching the breast, and audible swallowing is heard. However, the mother reports mild breast engorgement in the other breast. Which statement is most accurate?
A. The attachment shown is incorrect because engorgement means the baby is not draining adequately
B. The attachment shown is correct; engorgement of the opposite breast is expected and managed by offering both breasts per feed
C. The mother should switch to formula until the engorgement resolves
D. Audible swallowing alone confirms correct attachment regardless of other signs
Reveal Answer
Answer: B. The attachment shown is correct; engorgement of the opposite breast is expected and managed by offering both breasts per feed
All four signs of correct attachment are present (mouth wide, lower lip everted, chin touching, audible swallowing), indicating the observed feed is correctly attached. Engorgement of the contralateral breast is a separate issue — it occurs when that breast has not been drained recently. The management is to offer both breasts at each feed and increase feeding frequency, not to switch to formula. Answer A is wrong because engorgement of the OTHER breast does not relate to the attachment of the currently feeding side. Answer D is wrong because audible swallowing alone is one sign; all four attachment signs together confirm correct latch.
CLINICAL PEARL
The 'breast sandwich' technique is useful when engorgement makes the areola too firm for the infant to latch. Before latching, the mother compresses the breast with a C-hold or U-hold parallel to the infant's mouth (C-hold if the infant approaches from below, U-hold if from the side), briefly expressing a small amount of milk to soften the areola. This makes the areola more pliable and allows the infant to achieve a deep latch even when engorgement is at its worst. The technique is especially helpful in the first 3–5 days postpartum — precisely when engorgement peaks (milk 'coming in') and latching difficulties are most common. Teaching this one technique at the right moment can prevent premature supplementation in a large proportion of postnatal ward encounters.
Night feeds are non-negotiable in the first weeks. Prolactin levels are highest between 02:00 and 06:00. A mother who consistently skips night feeds will see her milk supply decline within days, regardless of daytime feeding frequency. Counsel every mother on this explicitly — 'your body produces the most milk at night and your baby signals hunger regardless of clock time.'
BFHI, Ten Steps, BPNI and World Breastfeeding Week
Beyond the bedside encounter with an individual mother, breastfeeding is a public health programme requiring institutional commitment, policy change, and community advocacy. The three intersecting structures the NMC competencies require you to know are BFHI, BPNI, and WBW.
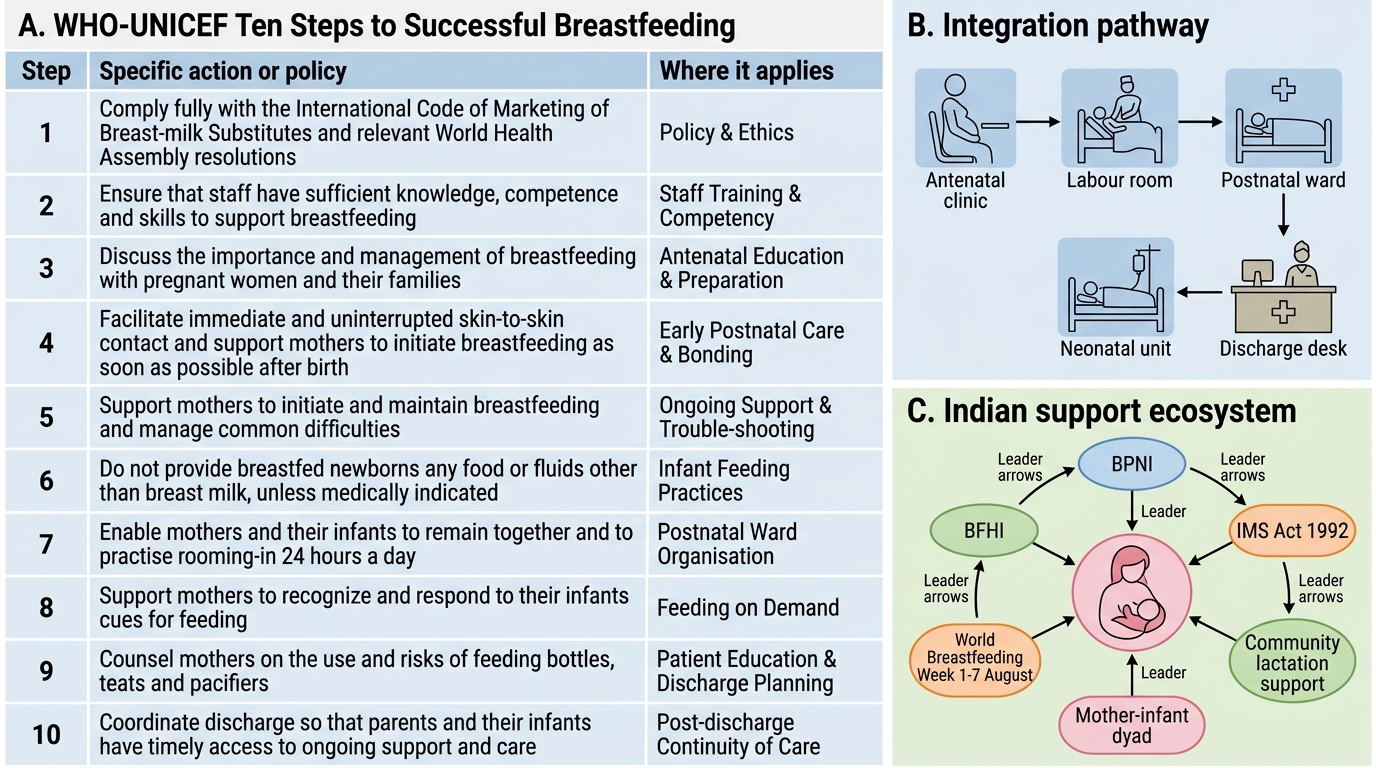
Baby-Friendly Hospital Initiative (BFHI) was launched jointly by WHO and UNICEF in 1991 as a global programme to encourage maternity services worldwide to implement the Ten Steps to Successful Breastfeeding. A hospital becomes 'Baby-Friendly Certified' only after external assessment and accreditation demonstrating sustained compliance with all ten steps. In India, BFHI accreditation is coordinated through the Ministry of Health and Family Welfare and is a quality indicator for government maternity facilities.
The Ten Steps to Successful Breastfeeding (WHO-UNICEF, revised 2018):
The ten steps are divided into critical management procedures (institutional/policy level) and key clinical practices (individual care level):
Critical management procedures:
1. Comply fully with the International Code of Marketing of Breast-milk Substitutes and relevant World Health Assembly resolutions
2. Have a written infant feeding policy that is routinely communicated to staff and parents
3. Establish ongoing monitoring and data-management systems
4. Ensure that staff have sufficient knowledge, competence and skills to support breastfeeding
Key clinical practices:
5. Discuss the importance and management of breastfeeding with pregnant women and their families
6. Facilitate immediate and uninterrupted skin-to-skin contact and support mothers to initiate breastfeeding as soon as possible after birth
7. Support mothers to initiate and maintain breastfeeding and manage common difficulties
8. Do not provide breastfed newborns any food or fluids other than breast milk, unless medically indicated
9. Enable mothers and their infants to remain together and to practise rooming-in 24 hours a day
10. Support mothers to recognise and respond to their infants' cues for feeding
Two additional provisions (from the revised 2018 implementation guidance) address: (a) counselling mothers about the use of pacifiers and artificial nipples; (b) creating an environment that enables breastfeeding in outpatient and community settings.
WHO-UNICEF Ten Steps to Successful Breastfeeding
BPNI (Breastfeeding Promotion Network of India) is a national non-governmental organisation established in 1991 — the same year as BFHI. BPNI works toward universal adoption of BFHI in Indian hospitals, trains health workers in lactation counselling, produces India-specific advocacy materials, and monitors compliance with the Infant Milk Substitutes, Feeding Bottles and Infant Foods (Regulation of Production, Supply and Distribution) Act, 1992 (IMS Act) — India's national implementation of the WHO International Code. Understanding BPNI's role helps the intern appreciate the institutional ecosystem that supports the bedside skills: the counselling you provide is supported by national policy, hospital accreditation standards, and an organised advocacy network.
World Breastfeeding Week (WBW) is observed annually from 1 to 7 August each year, coordinated by the World Alliance for Breastfeeding Action (WABA) in collaboration with WHO and UNICEF. Each year carries a specific theme announced by WABA. In hospitals and medical colleges, WBW is observed through awareness campaigns, counselling rallies, poster competitions, street plays, and faculty-supervised counselling sessions in postnatal wards. PE7.7 requires the student to participate in WBW celebrations at their institution — this means active involvement, not passive attendance. As an intern you may be asked to: deliver a brief health talk to mothers in the postnatal ward, facilitate a demonstration of correct breastfeeding technique to a group of nursing students or mothers, assist in a community outreach session, or contribute to a poster or mural display on breastfeeding benefits.
The counselling framework for a postnatal breastfeeding session uses a structured approach: ask (how is feeding going?), look (observe a complete feed), listen (what concerns does the mother have?), teach (demonstrate or reinforce correct technique), praise (acknowledge what is already going well — this is as important as correction), and refer (escalate if technique correction fails within 24–48 hours). This 'ALLTPR' or equivalent structured counselling loop is the observed/supervised practice expected at PE7.7 level — you participate alongside a senior, not independently.
SELF-CHECK
Which of the following statements about the Baby-Friendly Hospital Initiative (BFHI) Ten Steps is INCORRECT?
A. Step 6 includes immediate skin-to-skin contact after birth
B. Step 9 requires rooming-in 24 hours a day
C. Step 8 prohibits giving any supplemental food or fluid to breastfed newborns except on medical indication
D. The Ten Steps were originally developed in 1975 by UNICEF alone
Reveal Answer
Answer: D. The Ten Steps were originally developed in 1975 by UNICEF alone
The BFHI and its Ten Steps were jointly launched by WHO and UNICEF in 1991, not in 1975, and not by UNICEF alone. The Ten Steps were revised most recently in 2018. Answers A, B, and C are all correct statements: Step 6 mandates immediate skin-to-skin contact; Step 9 requires rooming-in 24 hours a day; Step 8 prohibits non-medically-indicated supplements for breastfed newborns.
Self-Assessment: Breastfeeding Technique and Support
Use the following structured self-check to consolidate the observational, analytical, and advocacy skills covered in this module. These questions mirror the types of OSCE stations and AETCOM reflective assessments you will encounter in your final-year postings. Approaching them systematically — formulating your answer independently before comparing with peers — is far more effective for long-term retention than passive re-reading. Each question is designed to integrate multiple arc steps: technique observation requires the physiology knowledge from step 2 to explain why a problem is happening, not just that it is happening. The public-health questions (BFHI steps, WBW activities) test programmatic knowledge that is frequently examined because it differentiates interns who understand the health-system context of clinical care from those who know only the bedside skill in isolation. Set aside 20 minutes and attempt all five questions before checking against the model answers in the debrief session.
Self-check questions:
- Technique identification: You observe a mother breastfeeding. The infant's mouth is half-open, lower lip is tucked inward, equal amounts of areola are visible above and below the mouth, and the chin is 1 cm from the breast. The mother reports nipple pain. Identify which of the four attachment signs are incorrect, explain the likely consequence, and describe step-by-step what correction you would suggest.
- Physiology application: A mother asks why her milk supply seemed to decrease after she started giving one formula top-up at night to 'let herself sleep'. Using the prolactin-supply-demand mechanism, explain what has happened and what she should do to restore supply.
- BFHI knowledge: Name any five of the WHO-UNICEF Ten Steps to Successful Breastfeeding. For each, state whether it is a critical management procedure (institutional/policy) or a key clinical practice (individual care).
- WBW participation: Your college is planning World Breastfeeding Week activities. As an intern, list three specific activities you could participate in, and for each, describe briefly what your role would involve.
- Problem-solving: A mother on day 4 postpartum is experiencing bilateral breast engorgement. Her infant is not latching because the areola is too firm. Describe the technique you would teach her to soften the areola before latching, and state which BFHI step relates to supporting mothers with common breastfeeding difficulties.
Answers are discussed in the next session — form your responses independently first. Compare with peers and faculty during the debrief.