Page 22 of 33
PE13.3 | Iodine Nutrition — SDL Guide
Learning Objectives
- State the RDA for iodine across paediatric age groups and identify the principal dietary sources in the Indian context
- Describe the role of iodine in thyroid hormone synthesis and explain how deficiency affects the hypothalamic-pituitary-thyroid axis
- Describe the full spectrum of iodine deficiency disorders (IDD), from subclinical cognitive impairment through goitre to cretinism, distinguishing their timing and severity
- Explain the Universal Salt Iodisation (USI) standard for iodine content in salt in India, and outline the components of the National Iodine Deficiency Disorders Control Programme (NIDDCP)
INSTRUCTIONS
Iodine deficiency disorders (IDD) constitute the single most common cause of preventable mental retardation and brain damage in the world. India has made remarkable progress through Universal Salt Iodisation, yet pockets of iodine deficiency persist in the sub-Himalayan belt, parts of the Gangetic plain, and several northeastern states. The consequences of iodine deficiency during fetal and early childhood development — deaf-mutism, cretinism, and irreversible intellectual disability — are entirely preventable. This module equips you to understand the spectrum of IDD, the biochemical basis of iodine's role in thyroid physiology, and India's programmatic response.
References
- Ghai Essential Pediatrics, 9th ed, Ch 8 — Nutrition (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 591 — Hypothyroidism (textbook)
- NIDDCP (National Iodine Deficiency Disorders Control Programme) Guidelines, MoHFW India (guideline)
- WHO/UNICEF/ICCIDD: Assessment of Iodine Deficiency Disorders and Monitoring their Elimination, 3rd ed (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are posted at a primary health centre in a sub-Himalayan district. A schoolteacher brings two children for evaluation: an 8-year-old boy with a visible swelling in the front of his neck and a 5-year-old girl who was born in the same village. The 5-year-old is deaf-mute, has difficulty walking (spastic gait), and her parents say she has never spoken. Her birth was uneventful but she 'has always been slow.' On examination, the boy has a palpable thyroid enlargement and serum TSH is elevated at 12 mIU/L with low-normal T4. The girl shows features consistent with neurological cretinism. A community survey reveals that fewer than 40% of households in this village use iodised salt. What single intervention, had it been implemented before the girl's conception, could have entirely prevented her condition — and what is the exact standard India mandates for this intervention?
WHY THIS MATTERS
Iodine deficiency is the world's most prevalent preventable cause of intellectual disability. Unlike most micronutrient deficiencies, its most devastating consequences — fetal brain damage, deaf-mutism, and cretinism — are entirely determined by the mother's iodine status during pregnancy, meaning the window for prevention is before conception. Universal salt iodisation is one of the most cost-effective public health interventions ever implemented, costing less than 5 cents per person per year. Yet in India, surveys continue to find households in endemic areas using non-iodised salt, and iodine deficiency disorders including goitre, subclinical hypothyroidism, and cognitive impairment persist. As a physician — in any setting — you will counsel families on salt iodisation, identify endemic goitre in schools and communities, and screen newborns for congenital hypothyroidism. Understanding IDD from its molecular basis to its programmatic control is fundamental to community paediatrics in India.
RECALL
Before you proceed, recall from Physiology:
• The hypothalamic-pituitary-thyroid (HPT) axis: TRH from the hypothalamus → TSH from the pituitary → thyroid hormone synthesis; T3/T4 exert negative feedback on both hypothalamus and pituitary.
• Thyroid hormones (T3/T4) contain iodine as a structural component — iodine is the only micronutrient incorporated into a hormone molecule. T4 (thyroxine) has 4 iodine atoms; T3 (triiodothyronine) has 3.
• Thyroid hormone effects: regulate basal metabolic rate, brain myelination and differentiation, skeletal maturation, cardiac output, and thermogenesis; critical for normal fetal brain development in the first trimester (before the fetal thyroid is functional).
• Negative feedback: low T3/T4 → high TSH → thyroid hyperplasia (goitre) — the mechanism by which iodine deficiency produces goitre.
Iodine and Thyroid Function: Clinical Relevance
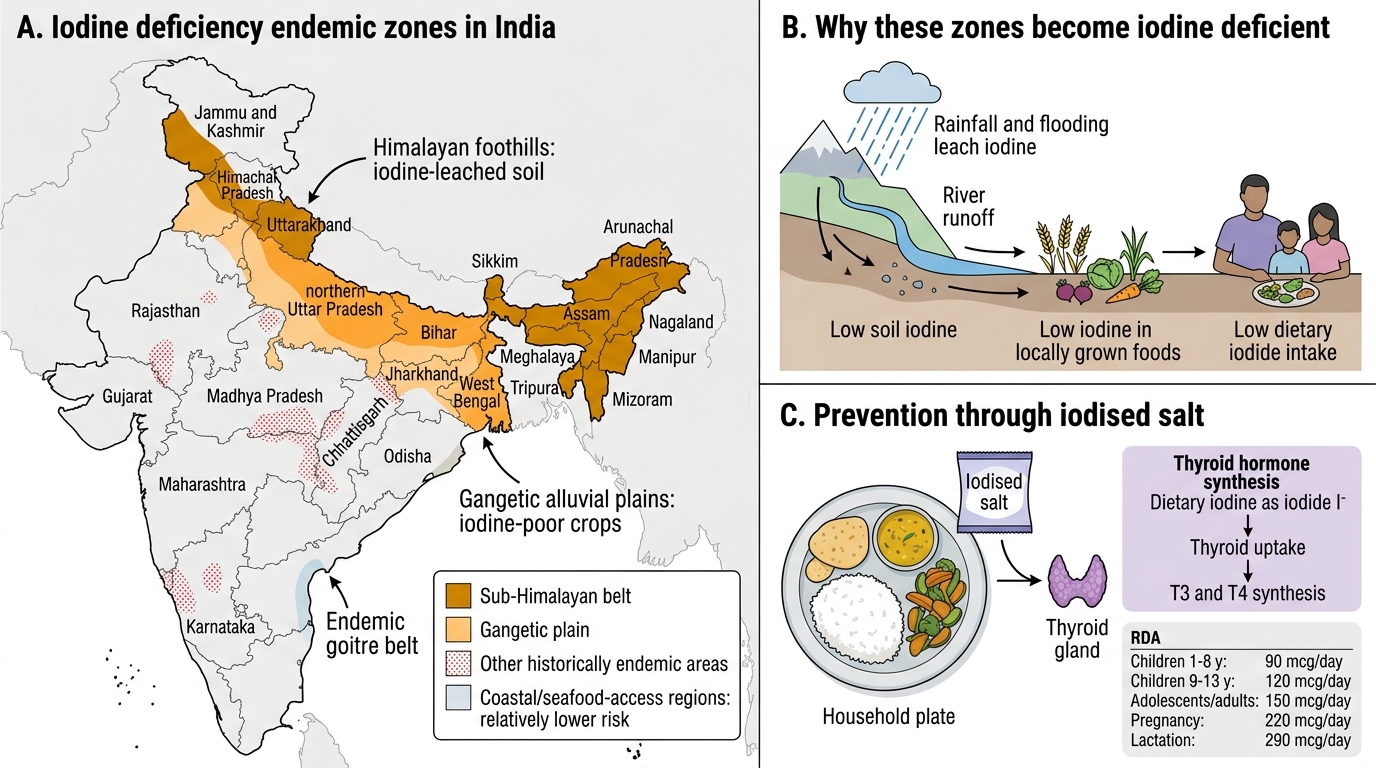
Iodine is a trace element with the unique biochemical distinction of being incorporated as a structural component into thyroid hormones — the only micronutrient that forms part of a hormone molecule. Without adequate iodine, the thyroid gland cannot synthesise sufficient T3 and T4, disrupting every organ system that depends on thyroid hormones for normal development and metabolic function. The consequences of iodine deficiency are collectively termed iodine deficiency disorders (IDD) and form a clinical spectrum ranging from mild subclinical cognitive impairment at the population level, through clinically apparent goitre, to the devastating neurological and developmental devastation of cretinism at the severe end. The WHO estimated that approximately 1.88 billion people globally were at risk of iodine deficiency before the global implementation of universal salt iodisation; India alone accounted for hundreds of millions. Despite substantial progress through the National Iodine Deficiency Disorders Control Programme (NIDDCP) and mandatory iodisation of salt for food use, IDD remains a public health concern in the sub-Himalayan belt, the Gangetic plains, parts of central India, and several northeastern states — areas where the soil is leached of iodine by glacial runoff and seasonal flooding, making the food grown locally naturally iodine-poor. The scale of IDD justifies the emphasis that Indian paediatric practice places on universal salt iodisation as a non-negotiable food safety standard.
Iodine Deficiency Endemic Zones in India
RDA, Dietary Sources, and Normal Iodine Physiology
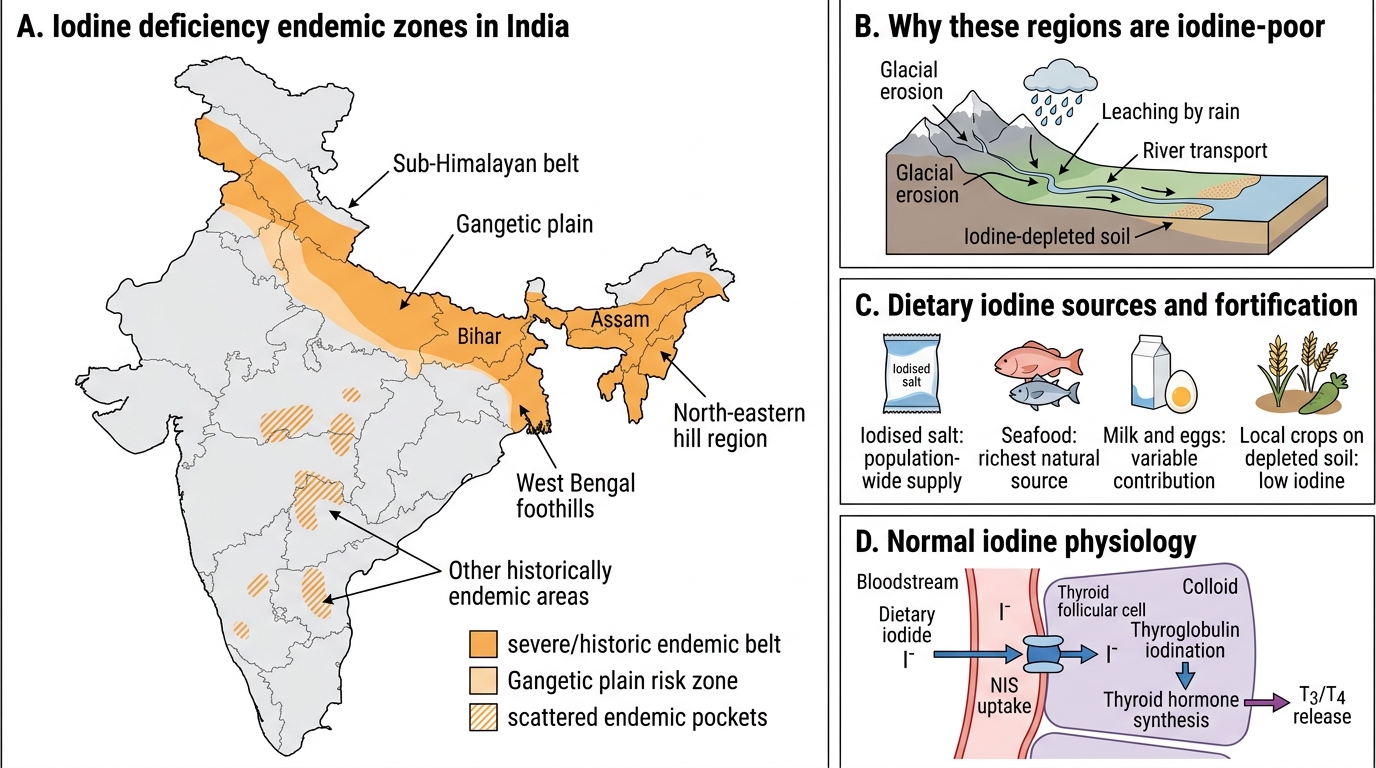
The Recommended Dietary Allowance (RDA) for iodine in India (ICMR/NIN 2020) is 90 mcg/day for children aged 1–8 years, 120 mcg/day for children aged 9–13 years, and 150 mcg/day for adolescents (14+ years) and adults. Requirements increase substantially in pregnancy (220 mcg/day) and lactation (290 mcg/day) because iodine must supply both mother and fetus or infant. The natural dietary sources of iodine are limited in most land-based food systems: seafood (saltwater fish, shellfish, seaweed) is the richest natural source, containing 50–200 mcg/100g; dairy products contribute variable amounts depending on the iodine content of cattle feed; eggs contain moderate amounts. Plant foods grown on iodine-depleted soil — as is characteristic of most of the Himalayan foothills and the Gangetic alluvial plains — are extremely poor in iodine, and populations depending on locally grown cereals and vegetables in these areas develop deficiency unless iodine is provided through supplementation or fortification. This is why iodised salt is the cornerstone of the iodine supply in India: salt is consumed daily by almost all households across all socioeconomic groups, making it the ideal vehicle for population-wide fortification.
Thyroid hormone synthesis — the role of iodine:
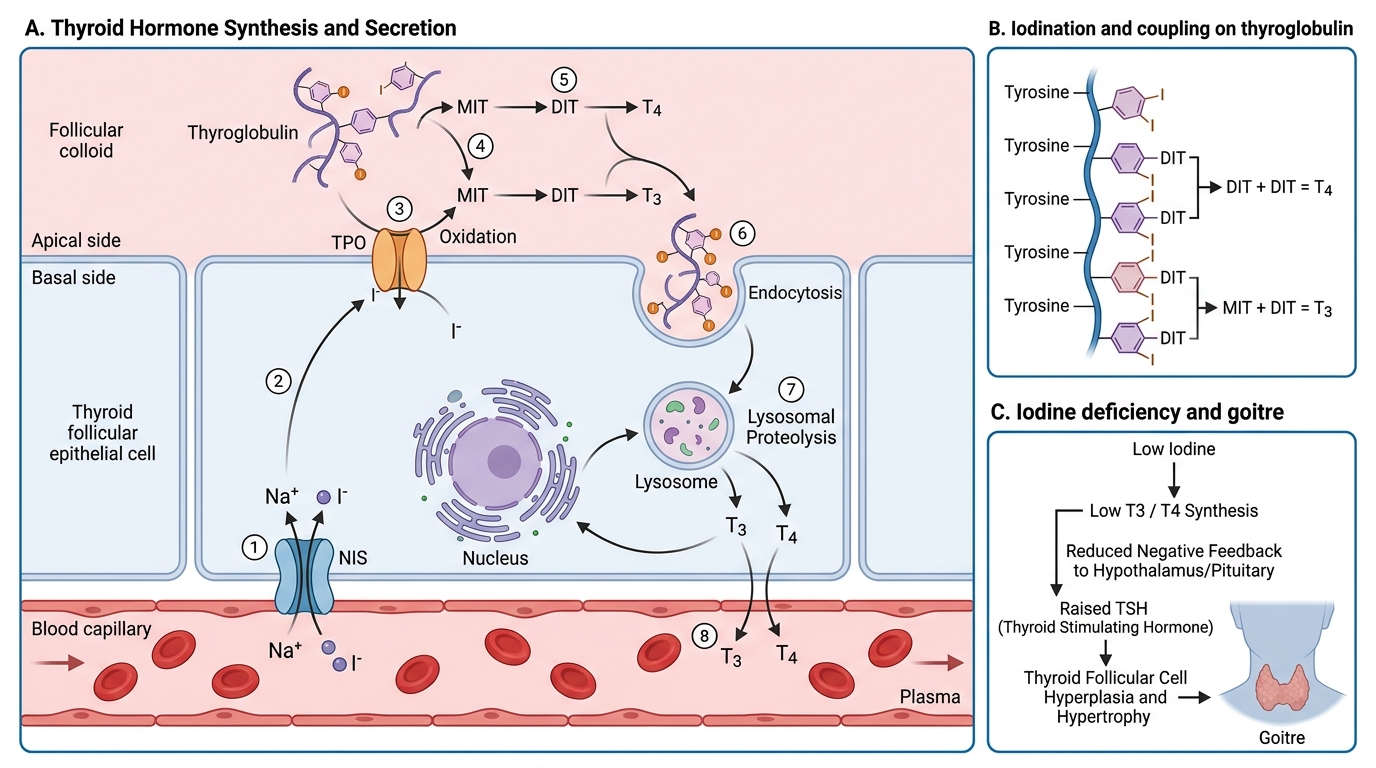
Dietary iodine is absorbed as iodide (I⁻) from the gut and transported to the thyroid gland, where it is actively concentrated by the sodium-iodide symporter (NIS) against a concentration gradient of 20–40 times the plasma level. Within thyroid follicular cells, thyroperoxidase (TPO) oxidises iodide to iodine (I₀ or I⁺), which then iodinates tyrosine residues on thyroglobulin (the iodine-storage glycoprotein in follicular colloid): one iodination produces monoiodotyrosine (MIT), two produce diiodotyrosine (DIT). TPO also catalyses the coupling of DIT+DIT → T4 (thyroxine, 4 iodine atoms) and DIT+MIT → T3 (triiodothyronine, 3 iodine atoms). T4 is the primary secretory product of the thyroid; most circulating T3 is produced by peripheral deiodination of T4 in liver and kidney by type 1 and type 2 deiodinases. T3 is 3–5 times more biologically active than T4 and is the principal hormone that binds nuclear thyroid hormone receptors to regulate gene expression. Iodine deficiency impairs every step from iodination of thyroglobulin onward; the TSH response to low T3/T4 drives thyroid hyperplasia, producing goitre.
Thyroid Hormone Synthesis and Iodine Deficiency Goitre
SELF-CHECK
Iodine deficiency leads to goitre through which sequence of events?
A. Low iodine → excess T4 → TSH suppression → thyroid atrophy
B. Low iodine → insufficient T3/T4 → raised TSH → thyroid follicular cell hyperplasia → goitre
C. Low iodine → direct stimulation of thyroid cells by iodide deficiency → autonomous growth
D. Low iodine → thyroperoxidase overactivation → toxic multinodular goitre
Reveal Answer
Answer: B. Low iodine → insufficient T3/T4 → raised TSH → thyroid follicular cell hyperplasia → goitre
Iodine is the substrate for thyroid hormone synthesis. Deficiency of iodine causes insufficient T3/T4 production. Low circulating T3/T4 removes the negative feedback on the hypothalamus and pituitary, resulting in elevated TRH and TSH. Chronically elevated TSH drives thyroid follicular cell hyperplasia and hypertrophy, producing an enlarged thyroid (goitre). TSH elevation is not suppressed in iodine deficiency — in fact, goitre TSH is typically elevated or high-normal. Option C (autonomous growth independent of TSH) describes toxic multinodular goitre, a different condition.
Mechanisms and Risk Groups for Iodine Deficiency
Iodine deficiency is fundamentally a geochemical problem before it is a dietary one: the iodine content of soil determines the iodine content of crops grown on it, and populations whose food systems are localised to iodine-poor soil are inherently at risk unless they access iodine through seafood, iodised salt, or supplementation. Several specific mechanisms and risk groups are relevant in Indian paediatric practice.
Geochemical causes are the primary determinant: heavy glacial runoff and annual flooding in the Himalayan foothills and sub-Himalayan plains leach iodine from the topsoil into rivers and ultimately the ocean. Regions historically identified as iodine-deficient in India include: Jammu & Kashmir, Himachal Pradesh, Uttarakhand, Uttar Pradesh (hills), Bihar, Jharkhand, Odisha, the northeastern states (Assam, Meghalaya, Arunachal Pradesh), and parts of West Bengal. However, sporadic iodine deficiency is not limited to these states — any community with restricted access to iodised salt or seafood is at risk.
Dietary mechanisms: Exclusive reliance on locally grown plant foods from iodine-depleted soil; low consumption of seafood or dairy; use of non-iodised salt (traditional rock salt, sea salt sold without fortification, or salt from local unregulated sources). Goitrogens (substances that interfere with iodine utilisation) are present in cruciferous vegetables (cabbage, cassava, millet) and are a contributing factor when iodine intake is already borderline — they inhibit thyroid iodine uptake or hormone synthesis.
Physiological vulnerability at critical periods:
• Fetal period: The fetal brain requires maternal T4 for normal myelination and neural migration from the first trimester, before the fetal thyroid is functional (until approximately 12 weeks' gestation). Severe iodine deficiency in the mother during this window causes irreversible fetal brain damage — the basis of cretinism — regardless of postnatal iodine correction.
• Neonatal period: Neonates have very high iodine requirements relative to body size; premature infants are particularly vulnerable.
• Infancy and early childhood: Rapid brain growth through age 3 makes this a critical window; even mild iodine deficiency can produce measurable reductions in IQ.
• Adolescence: Puberty increases thyroid hormone requirements; adolescent girls in endemic areas are at higher risk of goitre.
Iodine Deficiency Endemic Zones and Physiology in India