Page 23 of 33
PE13.3 | Iodine Nutrition — SDL Guide (Part 2)
Iodine Deficiency Disorders (IDD): Clinical Spectrum and Diagnosis
The term 'iodine deficiency disorders' explicitly acknowledges that iodine deficiency is not a single disease but a spectrum of conditions whose expression depends on the severity of deficiency, the timing relative to developmental windows, and the population group affected. This spectrum is wider than simply goitre — the most visible manifestation — and much of the iceberg lies beneath the surface as subclinical cognitive impairment affecting millions.
1. Subclinical cognitive impairment (mild–moderate iodine deficiency):
The most common but least clinically apparent consequence. Population-level iodine deficiency produces a 10–15 point reduction in median IQ scores — a measurable intellectual impairment at the community level detectable only through cohort studies, not individual clinical assessment. This manifests as reduced school performance, decreased learning capacity, and lower socioeconomic productivity at the population scale.
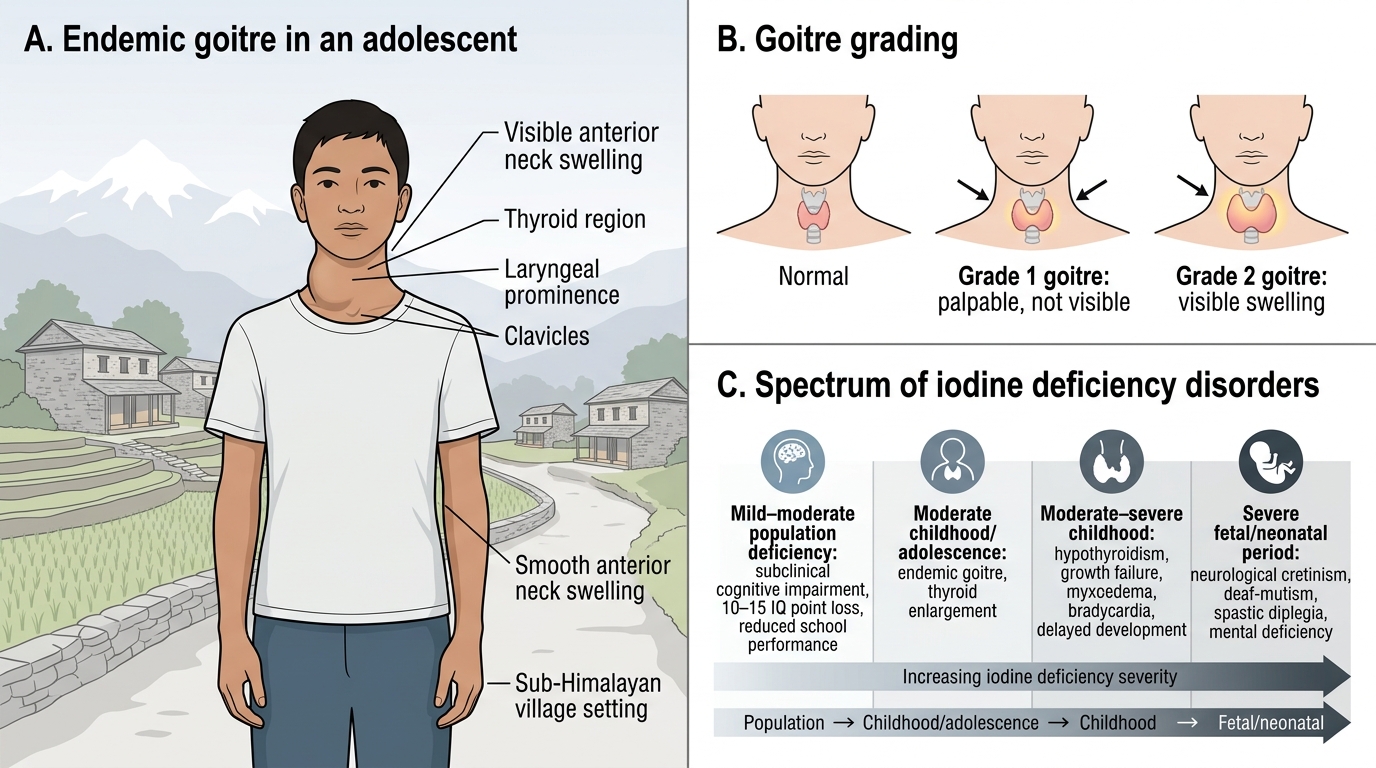
2. Endemic goitre (moderate iodine deficiency):
The thyroid gland enlarges under chronic TSH stimulation. Grading uses WHO criteria: Grade 0 = no goitre; Grade 1 = goitre palpable but not visible; Grade 2 = goitre visible and palpable. Population prevalence >10% in school-age children defines endemic goitre. Children and adolescents in endemic areas commonly present with Grade 1 or 2 goitre on school health screening. Goitre itself is not immediately harmful but reflects inadequate iodine intake and is a marker for the population's risk of more severe IDD.
3. Hypothyroidism (moderate–severe iodine deficiency):
Overt hypothyroidism occurs when iodine deficiency is severe enough that T4 synthesis is critically impaired despite TSH stimulation. Children present with growth retardation, delayed bone age, constipation, cool dry skin, bradycardia, myxoedema (non-pitting oedema), lethargy, and delayed developmental milestones. In adolescents, hypothyroidism delays pubertal development.
4. Cretinism (severe iodine deficiency during fetal/neonatal period):
The most devastating consequence, caused by severe iodine deficiency during fetal brain development. Two distinct types exist:
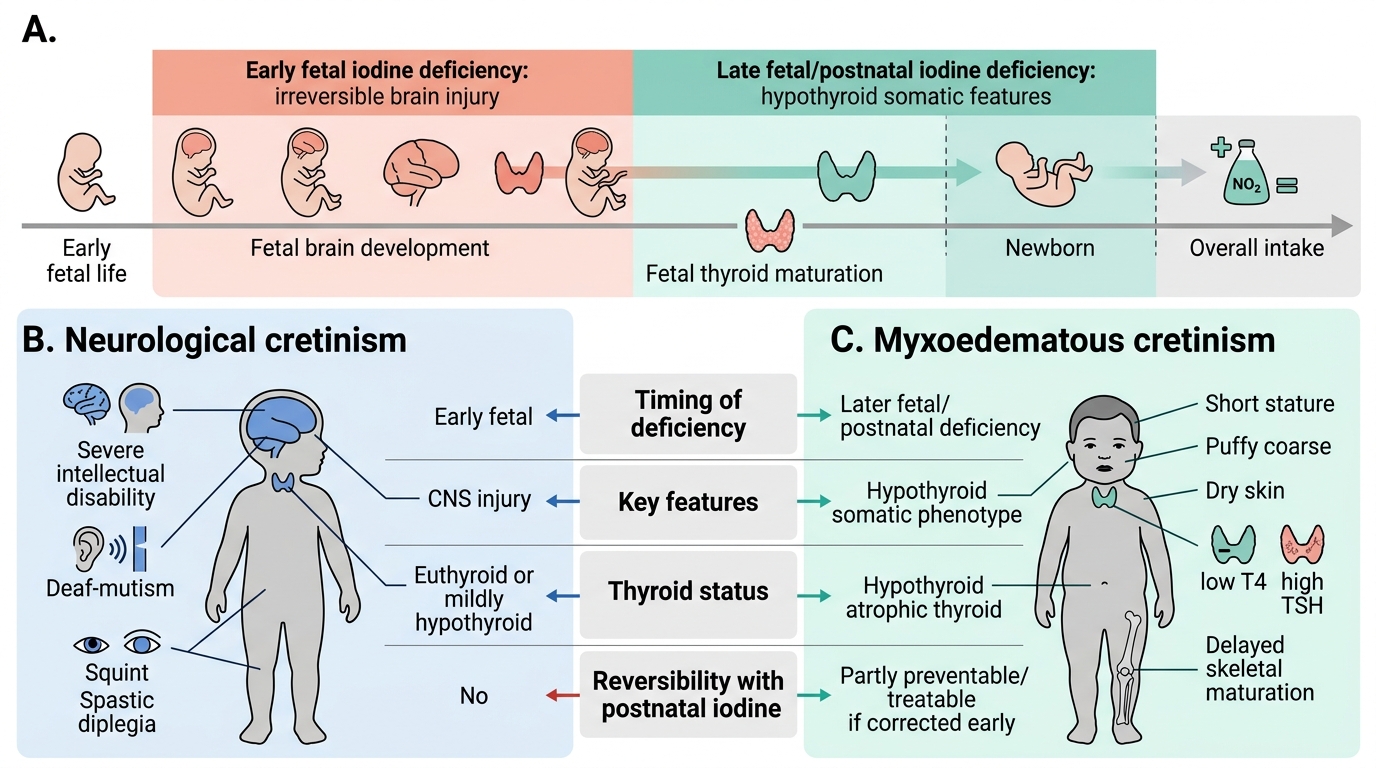
Neurological cretinism (commoner where deficiency is very severe): results from maternal iodine deficiency in the first trimester when the fetal thyroid is not yet functional; presents with deaf-mutism, spastic diplegia (lower-limb spasticity), mental deficiency, squint, and gait abnormalities. The thyroid may be normal or goitrous in the child.
Myxoedematous cretinism (more prevalent where deficiency begins perinatally): results from thyroid atrophy due to severe iodine deficiency at/after birth; presents with growth failure, puffy facies, dry skin, umbilical hernia, hypothermia, constipation, and intellectual disability but without the neurological features (no deaf-mutism, no spastic diplegia).
Diagnosis: Goitre grading on physical examination; serum TSH (elevated), serum T4 (low); urinary iodine concentration (UIC) < 100 mcg/L = iodine deficiency at population level; neonatal TSH screening on day 3–5 filter paper test.
Endemic Goitre and Iodine Deficiency Disorders
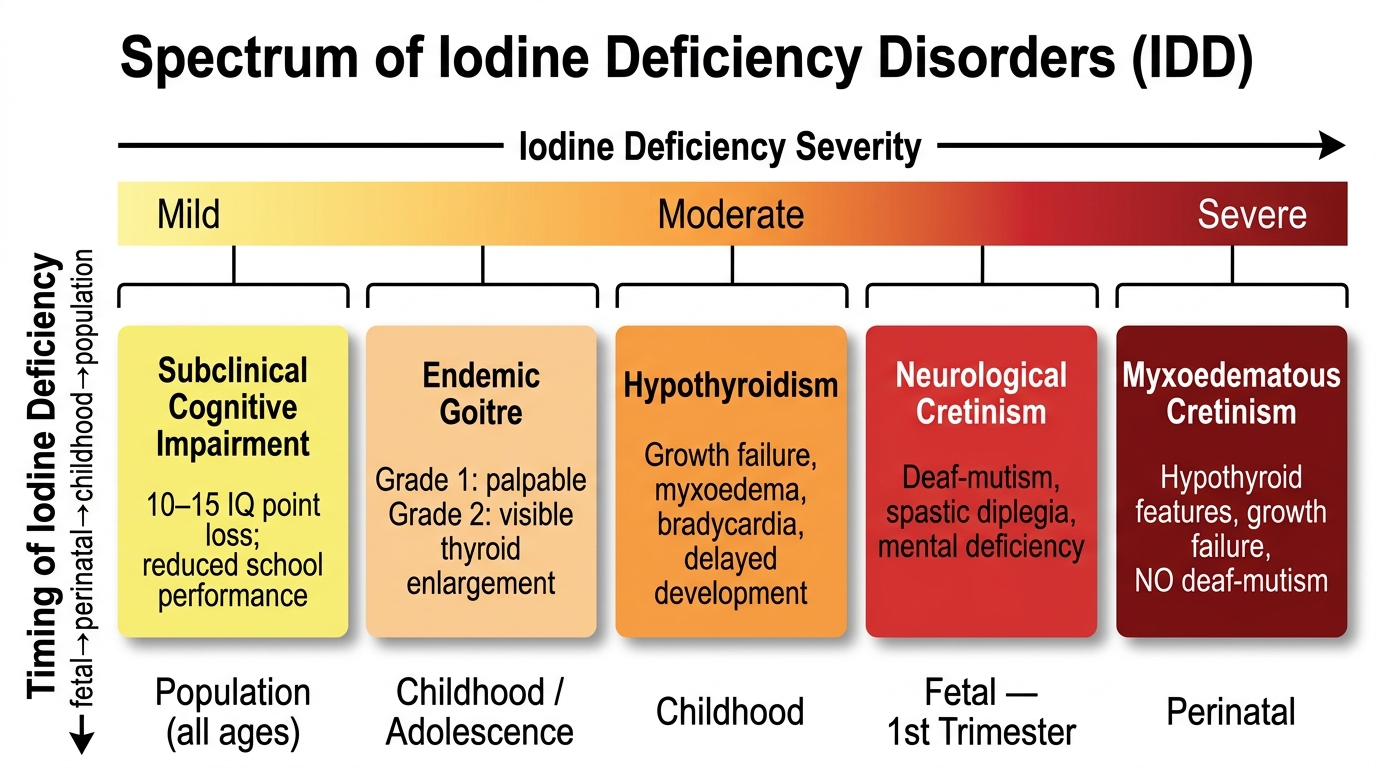
Spectrum of Iodine Deficiency Disorders by Severity and Timing
| Severity/Timing | Disorder | Key features |
|---|---|---|
| Mild–moderate, population | Subclinical cognitive impairment | 10–15 IQ point loss; reduced school performance |
| Moderate, childhood/adolescence | Endemic goitre | Thyroid enlargement; Grade 1 (palpable) or 2 (visible) |
| Moderate–severe, childhood | Hypothyroidism | Growth failure, myxoedema, bradycardia, delayed development |
| Severe, fetal (first trimester) | Neurological cretinism | Deaf-mutism, spastic diplegia, mental deficiency |
| Severe, perinatal | Myxoedematous cretinism | Hypothyroid features, growth failure, NO deaf-mutism |
CLINICAL PEARL
Two IDD clinical distinctions that are high-yield in examinations:
1. Neurological cretinism vs myxoedematous cretinism: Neurological cretinism results from maternal iodine deficiency in the FIRST TRIMESTER (before the fetal thyroid is functional) — the child has deaf-mutism and spastic diplegia but may have normal-sized thyroid and even normal T4 at birth. Myxoedematous cretinism results from iodine deficiency AT or AFTER birth — the child has hypothyroid features (puffy facies, growth failure, dry skin) but NO deaf-mutism and NO spastic diplegia. The timing of deficiency determines the type.
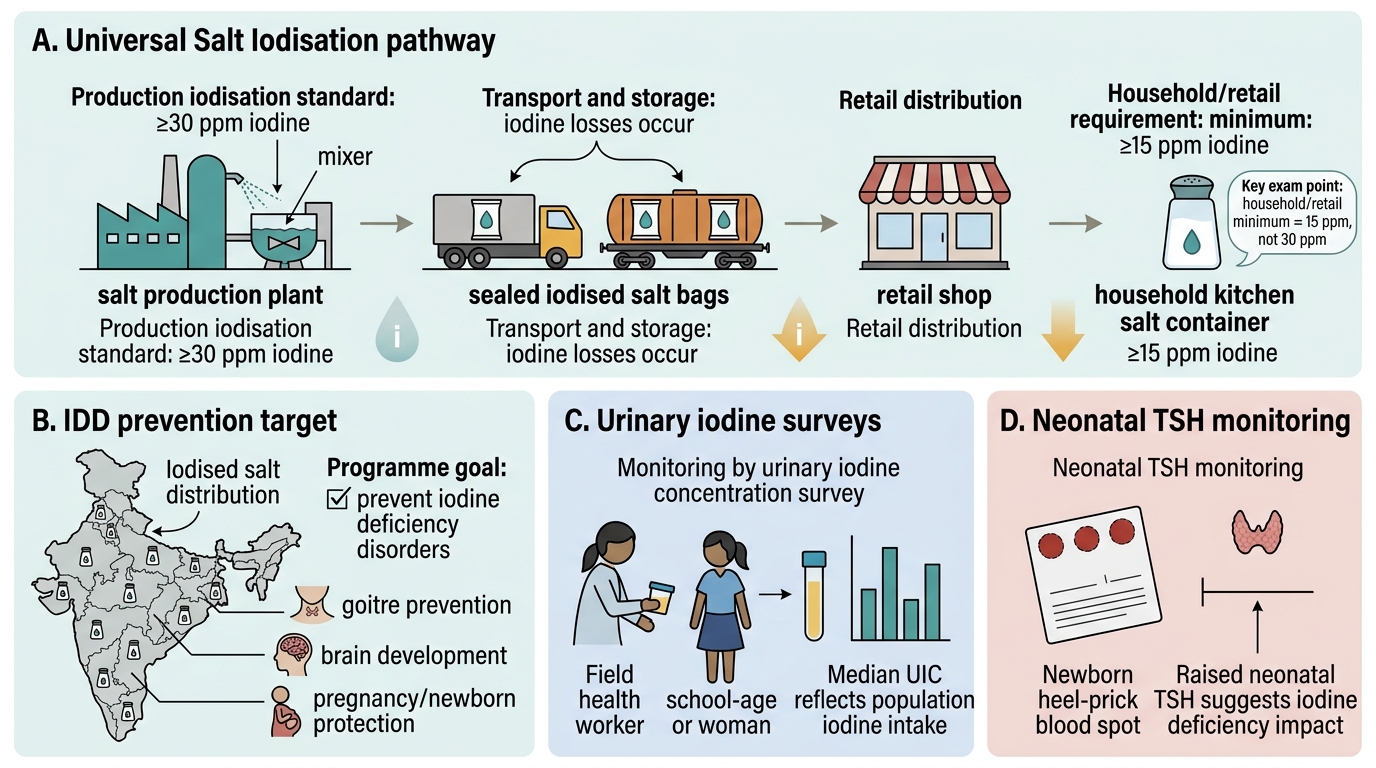
2. USI target — iodine content at household level is ≥15 ppm, NOT at production. Salt iodine content at the production/factory level must be ≥30 ppm to ensure that, after transport and storage losses (iodine evaporates from salt, especially in heat and humidity), the salt reaching the household still contains ≥15 ppm. This distinction appears in examinations — the question may ask for either level; know both.
Goitre Control Programme: Universal Salt Iodisation and NIDDCP
India's strategy to eliminate iodine deficiency disorders is built on Universal Salt Iodisation (USI) — the mandatory fortification of all salt for human consumption with potassium iodate. Salt is the chosen vehicle because it is consumed in relatively consistent quantities (approximately 10 g/day per person) across all socioeconomic groups regardless of income, region, or dietary habit; it is produced by a relatively concentrated industry (making point-of-production quality control highly feasible); and it is one of the only foods universally consumed across all regions and seasons of the year.
Legislative mandate and USI standard:
India enacted the Prevention of Food Adulteration (PFA) Act and subsequently the Food Safety and Standards (FSS) Act requirements mandating that all salt sold for human consumption must contain iodine. The standard under Indian food safety law is:
• Iodine content at the production/wholesale level: ≥30 ppm (mg/kg)
• Iodine content at the retail/household level: ≥15 ppm (mg/kg)
The higher production standard accounts for losses during transport, storage (humidity, heat, exposure to light accelerate iodine loss from salt), and cooking. Potassium iodate (KIO₃) is the preferred iodising agent in India rather than potassium iodide (KI) because iodate is more stable in the tropical climate.
National Iodine Deficiency Disorders Control Programme (NIDDCP):
Launched in 1962 (originally as Goitre Control Programme, renamed NIDDCP in 1992), the programme operates through the Ministry of Health and Family Welfare and state health departments. Key components:
• Salt iodisation and regulatory enforcement: quality testing at production, distribution, and household levels.
• Surveillance: national surveys of urinary iodine concentration (UIC) in school-age children (target: median UIC 100–199 mcg/L); neonatal TSH filter-paper screening as a population-level indicator.
• Goitre surveys: school-age surveys using WHO grading criteria to map endemic areas and monitor progress.
• Communication and community education: promotion of iodised salt use; addressing myths about taste and safety of iodised salt; training of ASHAs and Anganwadi workers.
• Emergency iodine supplementation: iodised oil capsules in severely deficient areas during outbreak control.
Programme achievements and gaps: USI implementation has dramatically reduced IDD in most parts of India; endemic cretinism is now rare in areas with consistent iodised salt coverage. However, surveys continue to identify pockets where >50% of households use non-iodised salt, particularly in remote areas, areas served by informal salt markets, and communities using traditional rock or mineral salts for religious or cultural reasons.
Universal Salt Iodisation in India
SELF-CHECK
What is the minimum iodine content of iodised salt at the household/retail level under Indian food safety standards?
A. 5 ppm (mg/kg)
B. 15 ppm (mg/kg)
C. 30 ppm (mg/kg)
D. 50 ppm (mg/kg)
Reveal Answer
Answer: B. 15 ppm (mg/kg)
Indian food safety standards (Food Safety and Standards Authority of India) require iodised salt to contain a minimum of 15 ppm (mg/kg) of iodine at the retail/household level. At the production level, the standard is ≥30 ppm to account for iodine losses during transport, storage, and cooking. Both thresholds need to be known: the 30 ppm production standard and the 15 ppm household standard. The 30 ppm figure is not the household standard — iodine is lost between production and household use, so the production level must be higher.
Self-Assessment
Iodine deficiency disorders require clinical reasoning across three dimensions: recognition of the clinical syndrome (which part of the IDD spectrum is this?), understanding the mechanism and timing (when did the deficiency occur?), and programme knowledge (what is the USI standard, and what does the NIDDCP do?). These vignettes test all three. For each scenario, first identify which disorder on the IDD spectrum is most likely, then reason through the mechanism — and identify what prevention strategy should have been in place.
Vignette 1: During a school survey in a sub-Himalayan district, 15 out of 85 school-age children (aged 7–14 years) are found to have Grade 2 visible goitre. The area receives drinking water from glacial rivers. A household survey finds that 55% of homes use non-iodised rock salt.
• What is the public-health classification of this population's iodine status?
• What is the biological mechanism of goitre in these children?
• What immediate programme intervention would you recommend?
• What is the WHO criterion for endemic goitre (threshold for 'endemic')?
Vignette 2: A 4-year-old child is brought with profound intellectual disability, inability to speak, and spastic legs. The mother gives a history of living in a mountain village during the pregnancy without access to iodised salt or healthcare. She did not take any supplementation. The child's thyroid is normal-sized and T4 is low-normal.
• What type of cretinism does this child have — neurological or myxoedematous? Explain your reasoning.
• At what gestational period did the critical iodine deficiency occur?
• Could postnatal iodine supplementation have reversed this child's neurological damage? Explain.
Neurological vs Myxoedematous Cretinism