Page 5 of 33
PE12.3 | Vitamin D — SDL Guide (Part 2)
Management of Nutritional Rickets
The treatment of nutritional rickets is highly effective and follows two approaches depending on clinical severity and the likelihood of treatment adherence. Both approaches use oral Vitamin D, which is safe, affordable, and available throughout India. Calcium supplementation is a critical co-component, particularly when dietary calcium intake is also inadequate, and dietary counselling should accompany medical treatment. The choice between stoss (single-dose megadose) and daily therapy is primarily a pragmatic decision: in resource-limited settings and in families with low health-seeking behaviour, stoss therapy ensures a reliable, once-only dose that does not depend on daily adherence — a significant advantage in a country where outpatient follow-up is uncertain. In contrast, daily therapy allows dose titration and is preferred for metabolic forms of rickets, infants under 3 months, and cases where stoss is not available. In all cases, treatment success is monitored by serial serum ALP measurements, which normalise over 3–6 months as bone mineralisation is restored.
Provided image
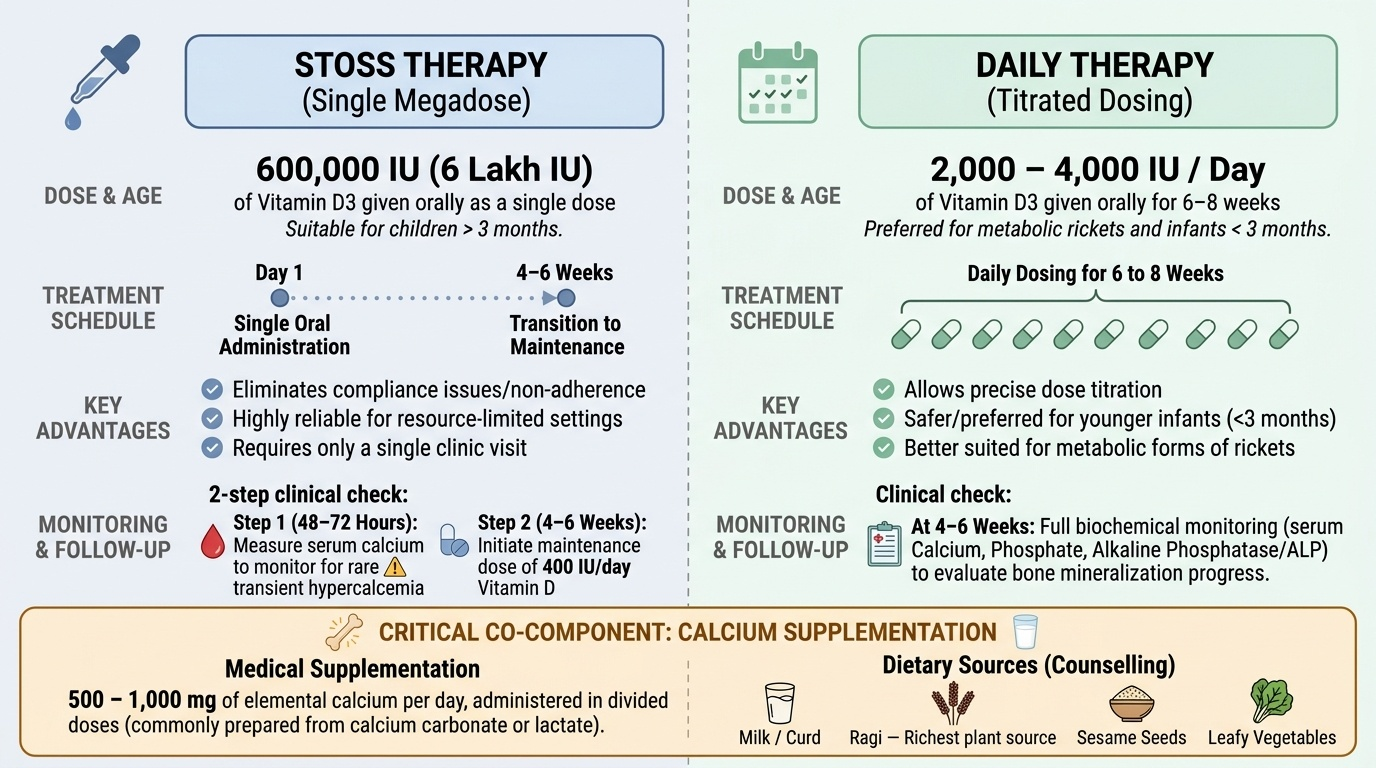
1. Stoss therapy (single-dose megadose regimen):
Stoss therapy, recommended by the IAP and detailed in Ghai's Essential Pediatrics, is the preferred approach for most cases of nutritional rickets in Indian practice because it eliminates the problem of treatment non-adherence:
• Dose: A single oral dose of 600,000 IU (6 lakh IU) of Vitamin D3
• Age: For children older than 3 months (some sources say 6 months; check local protocol)
• Advantages: single administration; reliable; eliminates adherence issues
• Monitoring: serum calcium measured at 48–72 hours post-dose to check for transient hypercalcaemia (rare)
• Maintenance: follow with 400 IU/day of Vitamin D after 4–6 weeks
2. Daily therapy:
• Dose: 2,000–4,000 IU/day of Vitamin D3 orally for 6–8 weeks
• Used when stoss is not feasible or in metabolic forms of rickets requiring titrated dosing
• Monitor biochemistry at 4–6 weeks
Calcium supplementation:
Always co-administer calcium, particularly if serum calcium is low or if calcium-deficiency rickets is suspected:
• 500–1,000 mg of elemental calcium per day in divided doses (from calcium carbonate or lactate)
• Dietary sources: dairy (milk, curd), sesame seeds, ragi (finger millet — the richest plant source), leafy vegetables
Prophylaxis (primary prevention):
This is the single most important public health intervention:
• All breastfed infants: begin Vitamin D supplementation within the first few days of life
• Prophylactic dose: 400 IU/day of Vitamin D3 (IAP recommendation; AAP concurs)
• Continue until the child has adequate dietary sources (fortified formula, fortified foods) and sun exposure
• Encourage safe sun exposure: 30 minutes of sunlight exposure to face and limbs daily where feasible
Vitamin D Toxicity (Hypervitaminosis D)
Vitamin D toxicity results from excessive intake, typically from supplemental sources rather than dietary or sun-derived Vitamin D, since sun exposure triggers an auto-regulatory mechanism that prevents cutaneous over-production of previtamin D3. Because Vitamin D3 is fat-soluble and stored in adipose tissue and liver, accumulation occurs with prolonged overconsumption, and the body cannot rapidly eliminate the excess via renal excretion the way it does with water-soluble vitamins. This is a critically important distinction to communicate to parents who, concerned about their child's bone health, may independently increase the dose of Vitamin D drops well beyond the recommended 400 IU/day. The principal mechanism of toxicity is hypercalcaemia mediated by excessive calcitriol production, which drives increased intestinal calcium absorption and skeletal calcium resorption. The clinical consequences flow directly from this hypercalcaemia — affecting the kidneys, gastrointestinal tract, cardiovascular system, and nervous system. Unlike the subtle early presentation of deficiency, severe Vitamin D toxicity is a medical emergency requiring prompt intervention.
Provided image
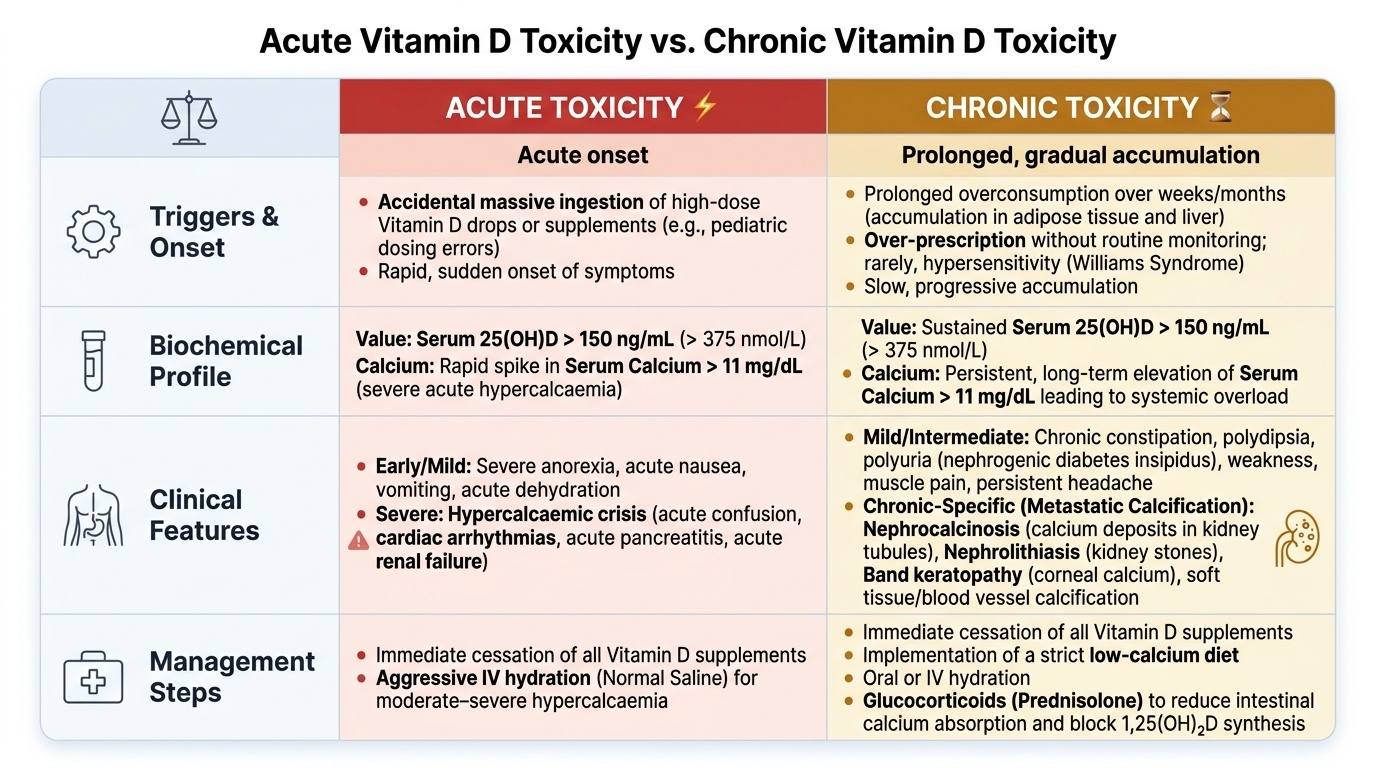
Causes of hypervitaminosis D in children:
• Accidental ingestion of high-dose Vitamin D supplements or fortified products
• Over-prescription of therapeutic doses without monitoring
• Rarely, Williams syndrome (hypersensitivity to Vitamin D causing hypercalcaemia at normal doses)
Biochemical threshold for toxicity: serum 25(OH)D >150 ng/mL (>375 nmol/L), combined with hypercalcaemia (serum calcium >11 mg/dL)
Clinical features of hypercalcaemia (the common pathway):
• Early (mild): anorexia, nausea, vomiting, constipation, polydipsia, polyuria (nephrogenic diabetes insipidus)
• Intermediate: weakness, muscle pain, headache, irritability
• Severe: hypercalcaemic crisis — confusion, cardiac arrhythmias, pancreatitis, renal failure
• Chronic: nephrocalcinosis (calcium deposition in renal tubules), nephrolithiasis, band keratopathy
• Metastatic calcification: in soft tissues, blood vessels, kidneys
Management:
• Immediate cessation of all Vitamin D supplements
• Low-calcium diet
• Hydration (IV normal saline for moderate–severe hypercalcaemia)
• Glucocorticoids (prednisolone) reduce intestinal calcium absorption and 1,25(OH)2D synthesis — useful in moderate-severe cases
• Loop diuretics (furosemide) to promote calciuresis in severe cases
• Monitor serum calcium frequently until normalisation
Key distinction: Vitamin D toxicity from supplementation is dose-dependent (25(OH)D >150 ng/mL); it does NOT occur from sun exposure alone (skin photoconversion of previtamin D is self-limiting). β-carotene analogy does not apply — Vitamin D has no analogous dietary safety escape valve.
SELF-CHECK
A 6-month-old infant was started on Vitamin D drops by her parents at 4 times the recommended dose 'to ensure good bones.' She now presents with vomiting, polydipsia, and polyuria. Serum calcium is 12.8 mg/dL and serum 25(OH)D is 210 ng/mL. What is the most important immediate management step?
A. Stop all Vitamin D supplementation immediately and hydrate with IV normal saline
B. Administer a single stoss dose of 600,000 IU to correct bone disease
C. Start oral calcium supplementation to correct the metabolic imbalance
D. Give thiazide diuretics to increase renal calcium reabsorption
Reveal Answer
Answer: A. Stop all Vitamin D supplementation immediately and hydrate with IV normal saline
This is hypervitaminosis D causing hypercalcaemia. The first step is to remove the causative agent — stop all Vitamin D immediately. IV hydration with normal saline corrects the volume depletion from polyuria and dilutes serum calcium. Stoss therapy would worsen the hypercalcaemia. Calcium supplementation is contraindicated. Thiazide diuretics increase calcium reabsorption (worsening hypercalcaemia); a loop diuretic (furosemide) is used to promote calcium excretion, not thiazides.
Self-Assessment
Returning to the opening case: the 14-month-old boy with bow legs, wrist widening, elevated ALP (980 U/L), low calcium (7.2 mg/dL) and low phosphate (2.8 mg/dL) has classic nutritional rickets. The risk factors — exclusive breastfeeding without supplementation, vegetarian diet, limited outdoor exposure — are the Indian high-risk triad. His younger sibling, born last month, should start 400 IU/day of Vitamin D from within the first few days of life — simple and effective prevention.
Treatment for the presenting child:
Administer stoss therapy: 600,000 IU of Vitamin D3 orally as a single dose (per IAP guidelines and Ghai). Co-administer calcium 500–1,000 mg/day. Arrange follow-up at 4–6 weeks to check ALP and serum calcium. Start maintenance 400 IU/day after the stoss response is confirmed.
Key examination recall points:
• Nutritional rickets peak age: 6 months–3 years
• Biochemical hallmark: markedly elevated ALP
• Most characteristic radiological sign: cupping, fraying, splaying of the metaphysis
• Stoss therapy dose: 600,000 IU single oral dose (>3 months age)
• Daily prophylaxis dose: 400 IU/day from first days of life for all breastfed infants
• Hypervitaminosis D threshold: 25(OH)D >150 ng/mL; manifestation = hypercalcaemia
• Vitamin D toxicity treatment: stop supplement, hydrate, glucocorticoids if moderate-severe
• Breast milk Vitamin D content is very low (~15–50 IU/L) regardless of maternal status
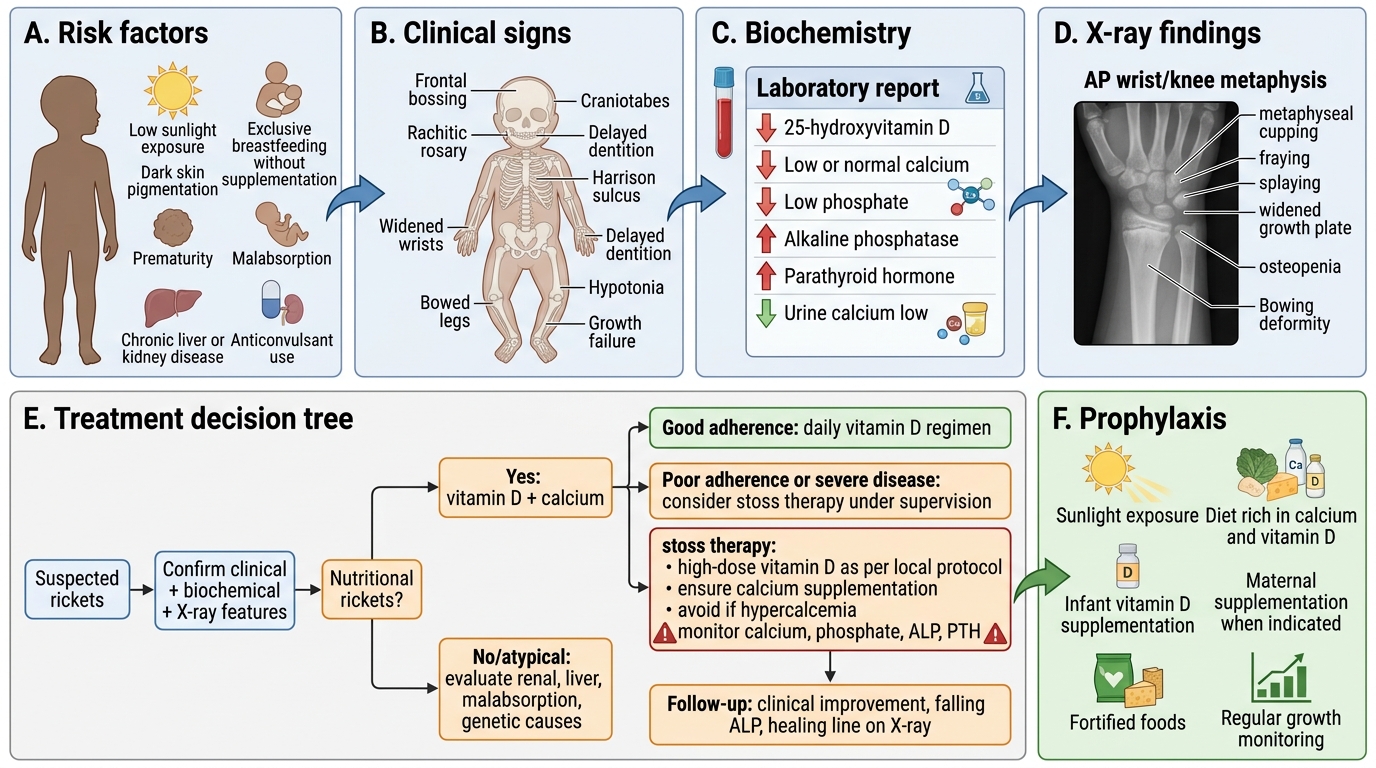
Rickets Diagnosis and Treatment Pathway