Page 8 of 20
PE16.{3-4,6} | IMNCI Child Assessment — SDL Guide
Learning Objectives
- Apply the IMNCI stepwise assessment algorithm to a child aged 2 months to 5 years
- Identify and respond to general danger signs as the mandatory first step
- Classify cough and breathing, diarrhoea with dehydration, fever, and ear problems using IMNCI colour-coded triage
- Measure MUAC correctly and identify children with severe acute malnutrition (SAM) and moderate acute malnutrition (MAM) per IMNCI criteria
- Apply IMNCI guidelines to risk-stratify diarrhoeal dehydration and plan appropriate referral or ORS treatment
- Counsel the caregiver on danger signs requiring immediate return and immunisation status
INSTRUCTIONS
Children aged 2 months to 5 years present to India's primary health system with an enormous variety of overlapping illnesses — pneumonia, diarrhoea, malaria, undernutrition, and ear infections often co-exist in the same child. The IMNCI child assessment algorithm is the tool that transforms a potentially chaotic clinical encounter into a structured, systematic appraisal that catches all these conditions simultaneously. It also enforces a critical safety rule: danger signs are checked first, so a child with lethargy or inability to drink is never inadvertently sent home with a prescription for a cough syrup. This SDL teaches you to apply the algorithm fluidly, in the correct order, with the correct thresholds.
References
- Ghai Essential Pediatrics, 9th edition, Ch 5 (Child Survival) and Ch 8 (Malnutrition) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 56 (Malnutrition) and Ch 337 (Acute Gastroenteritis) (textbook)
- MoHFW India — IMNCI Training Module 2: Management of the Sick Child (guideline)
- WHO — IMCI Chart Booklet, 2014 (guideline)
- IAP Guidelines on Management of Acute Diarrhea, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the duty MO at a PHC in rural Maharashtra. In 20 minutes, three children arrive in the waiting area. Child 1 is a 14-month-old boy with a three-day history of cough — he is breathing fast (48/min), his chest moves inward on the lower ribs when he breathes, his eyes are sunken, and his mother says he has had diarrhoea for five days. Child 2 is a 3-year-old girl with fever for six days — her mother mentions she had a rash three days ago. Child 3 is an 18-month-old whose right ear has been discharging pus for two weeks and whose arm, when measured, shows a MUAC tape landing in the red zone. Without the IMNCI algorithm, you might treat each for their primary complaint and miss: Child 1's severe dehydration (sunken eyes, fast breathing with chest indrawing = severe pneumonia, plus possible severe dehydration — both pink); Child 2's complicated measles risk (fever + rash > 3 days = refer); Child 3's SAM (MUAC red = <11.5 cm) which changes the entire management of the ear infection.
WHY THIS MATTERS
Pneumonia and diarrhoea together account for approximately 30% of under-5 deaths globally, and malnutrition is the underlying contributing factor in nearly half of all child deaths in low-income countries including India. The IMNCI child assessment algorithm was specifically engineered to detect these conditions in combination — something no single-disease clinical approach achieves. For you as a final-year MBBS student, three competencies converge in this SDL: PE16.3 (assess 2–59 month children and stratify risk), PE16.4 (identify undernutrition and plan referral), and PE16.6 (apply IMNCI to diarrhoeal dehydration). These are all SH-level skills — meaning you must be able to perform the assessment, not just describe it. This SDL equips you with the procedural knowledge; your ward and OPD postings will provide the hands-on practice.
RECALL
Before engaging with the procedure, activate the following prior knowledge:
- Age-specific physiology (PY): respiratory rate decreases with age as the airways widen and lung volumes increase. A 2-month-old normally breathes at 40–50/min; a 4-year-old at 20–30/min. This is why IMNCI uses age-specific cut-offs for fast breathing rather than a single threshold.
- Dehydration physiology (PY): water comprises approximately 75% of body weight in infants and 65% in toddlers. Children lose proportionally more water per kilogram during diarrhoea than adults, hence faster deterioration. Sunken eyes and reduced skin turgor reflect interstitial and intravascular volume loss.
- Malnutrition classification (PE earlier sessions): SAM = MUAC <11.5 cm (6–59 months) OR weight-for-height <−3 SD OR bilateral pedal oedema. These are hard thresholds — know them exactly.
- National Immunization Schedule (NIS): IMNCI mandates checking immunisation at every sick-child visit. Know the key vaccines and their ages: BCG/OPV-0/Hep-B at birth; pentavalent/OPV/IPV/rotavirus at 6/10/14 weeks; MR at 9–12 months; boosters at 16–24 months.
- ORS composition: reduced-osmolarity ORS = 245 mOsm/L (75 mmol/L sodium, 75 mmol/L glucose) — this is the WHO/UNICEF standard used in India, NOT the older high-osmolarity formulation.
Clinical Indication: The Child 2 Months to 5 Years — Why a Structured Assessment Matters
The IMNCI child algorithm (2 months to 5 years) addresses an age group characterised by three clinical realities that make unstructured assessment unreliable. First, multiple simultaneous illnesses are common — a malnourished child with pneumonia almost invariably has some degree of diarrhoea, and a febrile child with malaria may concurrently have moderate dehydration. Treating one without addressing the others is the most common source of preventable child deaths at primary care level. Second, severity is non-linear with symptoms — a child with fast breathing at 52/min who is feeding reasonably and alert is classified differently from a child with fast breathing at 52/min who also has sunken eyes and a skin-turgor test that comes back slowly. Identifying co-existing dehydration escalates the classification from pneumonia to a possible co-morbid emergency. Third, preventive opportunities are missed without a structured prompt — every sick-child visit is an opportunity to update immunisation, supplement vitamin A, screen for malnutrition, and counsel on breastfeeding. These preventive checks are built into the IMNCI algorithm as mandatory steps, not optional additions.
The clinical indication for applying the full IMNCI child assessment algorithm is any child aged 2 months to 5 years presenting to a PHC, sub-centre, community health centre, or ASHA visit with ANY complaint — illness or well-child visit. The algorithm must be completed in full, in sequence. Shortcuts based on the presenting complaint are the algorithm's single most common mode of failure.
PE16.3 requires you to assess children in this age group and stratify risk — a demonstrated skill (SH level). PE16.4 adds the ability to identify and plan referral for undernutrition. PE16.6 specifically requires applying the IMNCI algorithm to children with diarrhoeal dehydration — the most common reason for child death in this age band in India.
Governing Principles: Age-Specific Thresholds and the Assess-All Logic
Two physiological principles underpin the design of the IMNCI child assessment thresholds and explain why they must be applied precisely rather than approximately.
Provided image
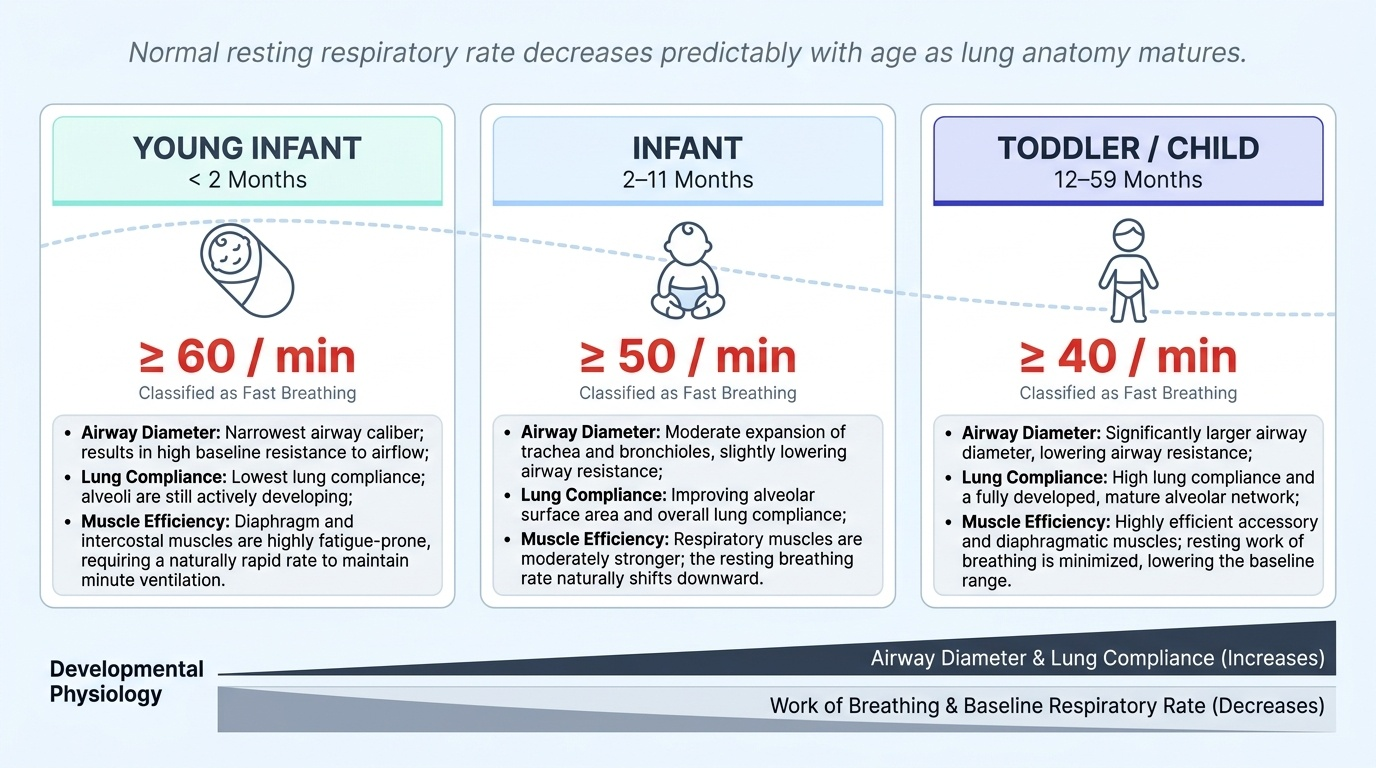
Principle 1 — Respiratory rate decreases predictably with age. As the child grows, airway diameter increases, lung compliance increases, and respiratory muscles become more efficient — all of which reduce the work of breathing and the resting respiratory rate. The IMNCI fast-breathing thresholds reflect age-specific normal distributions: at 2–11 months, a rate of 50/min or above falls outside the normal distribution for that age and predicts pneumonia with validated sensitivity; at 12–59 months, the threshold shifts down to 40/min for the same reason. Applying the wrong age-band threshold causes misclassification — a 13-month-old at 42/min is correctly classified as 'fast breathing' (threshold 40/min) but would be missed if the health worker applied the 2–11 month threshold (50/min) by mistake.
Principle 2 — Dehydration signs reflect fluid-compartment physiology. The three clinical dehydration signs used by IMNCI (general condition, eye sunkenness, skin turgor) reflect three sequential stages of volume loss. Eye sunkenness reflects interorbital fat and connective-tissue dehydration — it is visible and easily assessed. Skin turgor (the pinch test at the abdomen) reflects interstitial fluid volume — a turgor that returns in >2 seconds indicates >10% dehydration. General condition (lethargy vs restlessness) reflects cerebral and cardiovascular compensation — a lethargic, floppy child has moved from compensated to decompensated dehydration. IMNCI deliberately avoids the continuous urine-output or weight-loss methods that require laboratory equipment, using only these three bedside signs as surrogates.
Step 1: Checking General Danger Signs
The IMNCI algorithm mandates checking the four general danger signs as the absolute first step of every child assessment. This sequence is non-negotiable: before you ask about cough, before you count the respiratory rate, before you examine the ears — you check for danger signs. The rationale is that a child with ANY danger sign is immediately classified as Pink (urgent referral) regardless of all subsequent findings, so completing the rest of the algorithm first wastes time and delays life-saving transfer. The danger signs represent the minimum physiological threshold below which the child's compensatory mechanisms are failing — they are not subtle findings that require clinical experience to detect, but rather clear, observable, elicitable signs that any trained health worker can identify with a brief, targeted history and observation. The critical safety principle is that they can only protect the child if they are checked proactively at the start of every encounter, not retrospectively after the chief complaint has been addressed. A health worker who diagnoses 'pneumonia' and prescribes amoxicillin for a child who was also lethargic has failed the safety check that IMNCI was designed to enforce.
The four general danger signs in children 2 months to 5 years are:
- Unable to drink or breastfeed — the child cannot take fluid by mouth. Distinguish from 'not drinking much' (reduced intake, not a danger sign) — the danger sign is complete inability to drink. Test by offering a cup of water or letting the mother attempt breastfeeding.
- Vomits everything — the child vomits every time food or fluid is swallowed. This is NOT the same as occasional vomiting — it means complete inability to retain any oral intake, which prevents treatment with oral medicines, ORS, or feeding.
- Convulsions (current or during this illness) — active convulsion or a history of convulsions during the current illness episode. Ask specifically: 'Has the child had any fits, shaking, or jerking of arms/legs?' Parents often do not volunteer this information.
- Lethargic or unconscious — lethargic means the child is difficult to wake or does not respond normally to stimulation (calling by name, gentle touch). Test by calling the child's name and watching for eye-opening, movement, or response. An unconscious child does not respond to any stimulation.
If ANY one of these four danger signs is present, the child is classified as having a very severe disease — PINK — and must be referred urgently. Give any available pre-referral treatment (first dose of antibiotic, antipyretic if severely febrile, glucose if hypoglycaemic) and transfer immediately.
Important: many health workers do not elicit danger signs because the presenting complaint seems 'routine'. IMNCI prevents this by placing danger signs at the START of the algorithm — before any symptom-specific assessment begins.