Page 9 of 20
PE16.{3-4,6} | IMNCI Child Assessment — SDL Guide (Part 2)
Step 2: Assessing Cough and Breathing
After confirming the absence of danger signs (or classifying Pink if present), the IMNCI algorithm proceeds to assess primary symptoms in the order they appear on the chart booklet. Cough and breathing difficulty are assessed first among the symptom-specific domains because respiratory tract infections — particularly pneumonia — are the leading single infectious cause of death in children under 5, and because the key diagnostic sign of fast breathing can be measured objectively at the bedside without any equipment other than a watch. The assessment of cough and breathing in the IMNCI algorithm has three components: counting the respiratory rate to detect fast breathing, observing the chest wall for indrawing, and listening for stridor. Each component yields a progressively more severe classification if present, and they interact by upgrade — the most severe component found determines the classification for this domain. If the child does not have cough or breathing difficulty, skip this domain and proceed to diarrhoea. If the child has cough or breathing difficulty (including noisy breathing), the assessment proceeds as follows.
Respiratory rate count (60 seconds, watch mandatory): Count for a full 60 seconds using a watch. Apply the age-appropriate threshold:
• 2–11 months: fast breathing = ≥50 breaths/minute
• 12–59 months: fast breathing = ≥40 breaths/minute
If fast breathing is found, count a second time to confirm (as in the young-infant algorithm).
Chest indrawing: Look for inward movement of the lower chest wall (bony thorax) on inspiration. In children 2 months to 5 years (unlike young infants), ANY lower-chest-wall indrawing is a danger sign classifying as severe pneumonia — classified PINK. In this age group the chest wall is firmer than in neonates, so visible chest indrawing represents significantly increased respiratory effort.
Stridor: Listen or observe for stridor (a harsh, high-pitched inspiratory noise due to upper airway obstruction). Stridor at rest in a calm child = severe pneumonia sign = Pink.
IMNCI pneumonia classification:
• Severe pneumonia or very severe disease (Pink): any danger sign OR chest indrawing OR stridor. Refer urgently. Give first dose of antibiotic if available (amoxicillin or appropriate per current NHM guideline).
• Pneumonia (Yellow): fast breathing WITHOUT chest indrawing or danger sign. Treat with oral amoxicillin for 5 days; advise mother on follow-up and danger signs.
• No pneumonia (Green): no fast breathing, no chest indrawing, no danger sign. Treat cough with a soothing remedy; counsel on home care.
Important subtlety: If a child has both fast breathing AND chest indrawing, classify as severe pneumonia (Pink), NOT as ordinary pneumonia (Yellow). The additional sign of chest indrawing upgrades the classification regardless of respiratory rate.
SELF-CHECK
A 10-month-old child has a 2-day history of cough. Respiratory rate is 53/min on a 60-second count. She has lower chest wall indrawing. She is alert and drinking normally. What is the IMNCI classification and action?
A. Pneumonia (Yellow) — treat with oral amoxicillin because she is alert and drinking
B. No pneumonia (Green) — fast breathing alone at 53/min is borderline for this age
C. Severe pneumonia (Pink) — chest indrawing at this age = severe pneumonia regardless of alertness; refer urgently
D. Very severe disease (Pink) — she has a danger sign of inability to drink
Reveal Answer
Answer: C. Severe pneumonia (Pink) — chest indrawing at this age = severe pneumonia regardless of alertness; refer urgently
In children 2 months to 5 years, ANY lower chest wall indrawing classifies as severe pneumonia (Pink) — regardless of respiratory rate, alertness, or hydration status. Chest indrawing in this age group indicates significantly increased work of breathing and predicts a high risk of rapid deterioration. The fact that she is alert and drinking well is reassuring but does NOT downgrade the classification. Action: refer urgently; give first dose of appropriate antibiotic before transfer. Option A (Yellow) would be correct if only fast breathing were present without chest indrawing.
Step 3: Assessing Diarrhoea and Dehydration
Diarrhoeal disease is the second leading infectious cause of death in children under 5, and the key determinant of mortality is the speed and severity of dehydration. The IMNCI algorithm uses three observable clinical signs to classify dehydration into three tiers — no dehydration, some dehydration, and severe dehydration — each with a specific treatment plan. This system was validated in field studies across multiple countries and correctly stratifies the majority of children who need IV fluids versus those who can safely receive oral rehydration.
If the child has diarrhoea, first ask: How long? (≥14 days = persistent diarrhoea; classified separately). Is there blood in the stool? (Dysentery = blood = classified Yellow, treat with ciprofloxacin or appropriate antibiotic per NHM guideline).
Then assess dehydration using THREE clinical signs:
Sign 1 — General condition:
• Normal (active, alert) = no or some dehydration
• Restless and irritable = some dehydration
• Lethargic or unconscious = severe dehydration (= a general danger sign = PINK)
Sign 2 — Eyes:
• Normal = no dehydration
• Sunken = some or severe dehydration
• Very sunken and dry = severe dehydration
Sign 3 — Skin turgor (abdominal pinch test):
• Skin goes back quickly (immediately) = no dehydration
• Skin goes back slowly (takes 1–2 seconds) = some dehydration
• Skin goes back very slowly (takes >2 seconds) = severe dehydration
IMNCI dehydration classification:
• Severe dehydration (Pink): two or more signs from the 'severe' column (lethargic/unconscious + very sunken eyes + skin fold >2 sec). Treat with Plan C (IV rehydration) — refer urgently if IV not available at facility.
• Some dehydration (Yellow): two or more signs from the 'some' column. Treat with Plan B (ORS 75 mL/kg over 4 hours, given under observation).
• No dehydration (Green): insufficient signs for either category. Treat with Plan A (home ORS, continue feeding, return if worse).
ORS Plans (reduced-osmolarity ORS = 245 mOsm/L):
| Plan | Dehydration | Setting | Volume | Route |
|---|---|---|---|---|
| Plan A | None | Home | After each loose stool: <2 yr = 50–100 mL; 2–10 yr = 100–200 mL | Oral |
| Plan B | Some | Facility, observe | 75 mL/kg over 4 h | Oral |
| Plan C | Severe | Facility / refer | IV Ringer's lactate 100 mL/kg (30 mL/kg fast, then 70 mL/kg in 2.5 h) | IV |
Zinc supplementation: give in ALL children with diarrhoea:
• 6 months to 5 years: 20 mg/day for 14 days
• 2–6 months: 10 mg/day for 14 days
Zinc reduces diarrhoea duration, severity, and the risk of recurrence over the following 2–3 months — this is an evidence-based addition to the IMNCI protocol based on CHOICE and subsequent trials.
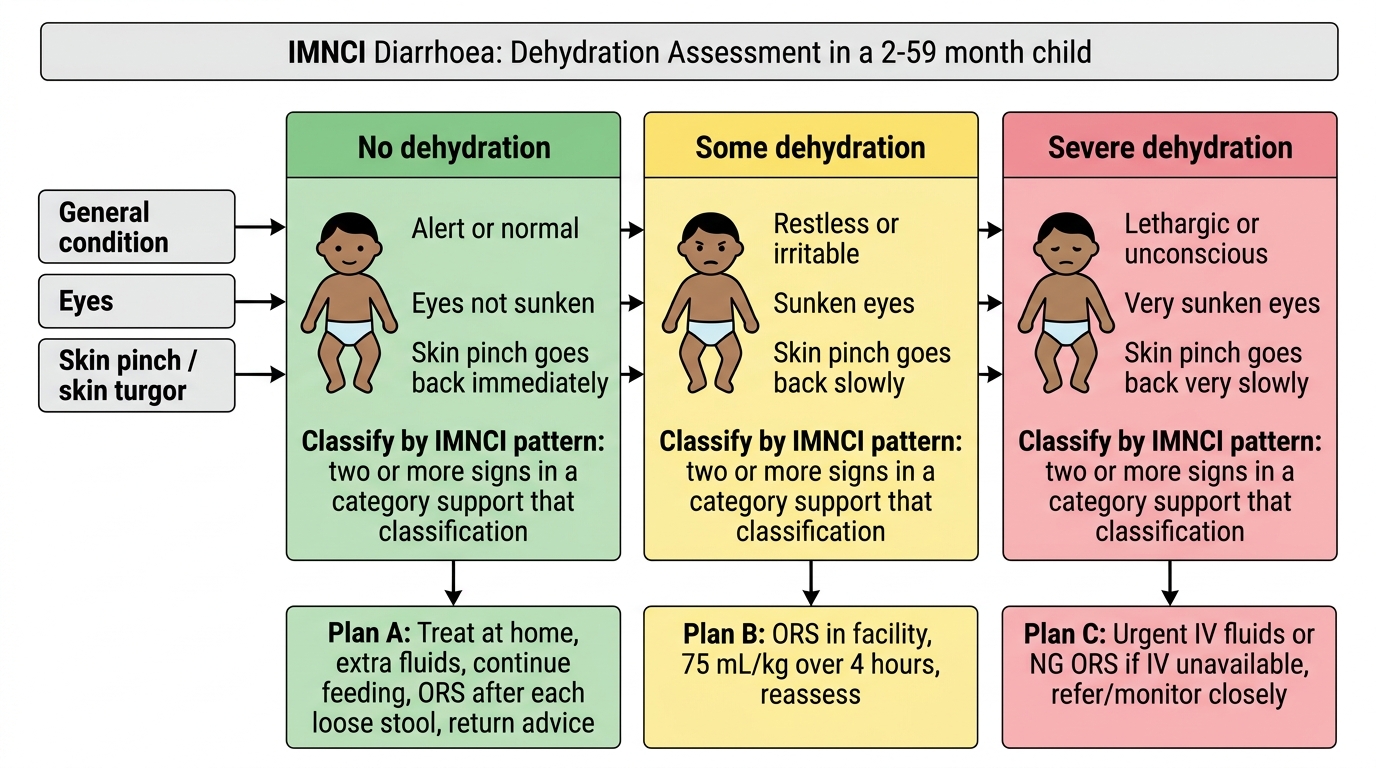
IMNCI Dehydration Assessment and ORS Plans
Step 4: Assessing Fever and Step 5: Ear Problems
After completing the cough/breathing and diarrhoea assessments, the IMNCI algorithm moves sequentially to evaluate fever and ear problems — two very common causes of illness in the 2–59 month age group that require their own risk-stratification logic independent of the earlier assessments. Fever is particularly important in the Indian context because it must trigger a reflex assessment for malaria in endemic areas, and because fever with specific co-features (rash, stiff neck, bulging fontanelle) signals conditions that require urgent referral regardless of whether the child has already been classified for a respiratory or gastrointestinal condition. Ear problems, though rarely life-threatening in isolation, are among the most common causes of antibiotic prescribing in primary care; IMNCI's structured ear assessment ensures that mastoiditis — a potentially serious complication of otitis media — is not missed as a simple earache, and that chronic ear discharge receives appropriate follow-up rather than repeated courses of antibiotics without ENT review. Both assessments illustrate the breadth of the IMNCI approach: it simultaneously covers the major causes of preventable child morbidity in a single consultation.
FEVER ASSESSMENT:
If the child has fever (≥37.5°C axillary or feels hot), assess for three conditions:
- Malaria risk: in malaria-endemic areas (India — most of rural India, especially tribal areas and northeastern states), any fever in a child warrants a malaria rapid diagnostic test (mRDT) or microscopy. IMNCI classifies: fever + positive mRDT = Malaria (Yellow) — treat with artemisinin-based combination therapy (ACT) per NVBDCP guidelines; fever + negative test with no other severe feature = Fever, no malaria (Yellow/Green depending on severity and duration).
- Measles: ask about rash with fever. If fever + generalised rash = classify for measles. If measles present for ≥3 days OR with complications (eye discharge, mouth sores, pneumonia) = refer (Pink or Yellow by severity). Current vaccination status is relevant — if the child has received MR vaccine this risk is reduced.
- Meningitis/severe febrile illness: stiff neck, photophobia, bulging fontanelle (in younger children), very high fever (≥39°C) = very severe febrile disease (Pink). Fever for ≥7 days without a source = classify as Unknown Fever, refer.
EAR PROBLEMS ASSESSMENT:
Ask about ear pain or ear discharge. Then:
• Look for pus draining from the ear
• Feel for tender swelling behind the ear (mastoiditis)
Classifications:
• Mastoiditis (Pink): tender swelling behind the ear. Refer urgently.
• Acute ear infection (Yellow): ear pain OR pus in the ear canal for <14 days. Treat with oral amoxicillin and dry mopping.
• Chronic ear infection (Yellow): ear discharge ≥14 days. Treat with dry mopping; refer to ENT if not improving.
• No ear problem (Green): no ear pain, no discharge.
Combined note on fever + malnutrition: a febrile SAM child is ALWAYS managed differently from a well-nourished febrile child — SAM suppresses fever response (may have normal temperature despite serious infection) and impairs immune response. A SAM child with ANY fever or even hypothermia must be classified and managed with a lower threshold for referral.
CLINICAL PEARL
The skin turgor test must be performed at the abdomen — not the forearm. A common examination error is to pinch the skin over the forearm or hand. In these locations, skin turgor is influenced by subcutaneous fat distribution and may give a falsely normal result in a dehydrated child or a falsely slow return in an obese child. The IMNCI-validated technique is a gentle pinch of the skin over the lateral abdomen — pick up a fold of skin between thumb and index finger, hold for 1 second, release, and observe. The 'goes back slowly' threshold (1–2 seconds) corresponds to approximately 5–9% dehydration; '>2 seconds' corresponds to ≥10% dehydration. If you time-threshold is missed in a busy clinical environment, err toward the more severe classification — the risk of undertreating severe dehydration is far greater than the risk of over-treating some dehydration.