Page 10 of 20
PE16.{3-4,6} | IMNCI Child Assessment — SDL Guide (Part 3)
Step 6: Nutritional Status — Undernutrition, MUAC, and SAM Identification
Nutritional assessment is the final major domain in the IMNCI child algorithm, and it is the domain most frequently omitted in real-world practice. Malnutrition both increases the severity of every other illness assessed in the algorithm (pneumonia in a SAM child carries a case fatality rate 10× higher than in a well-nourished child) and is itself a referral-triggering condition independent of any acute illness. PE16.4 specifically requires you to identify children with undernutrition per IMNCI criteria and plan appropriate referral.
The IMNCI nutritional assessment has three components:
Component 1 — MUAC (Mid-Upper Arm Circumference):
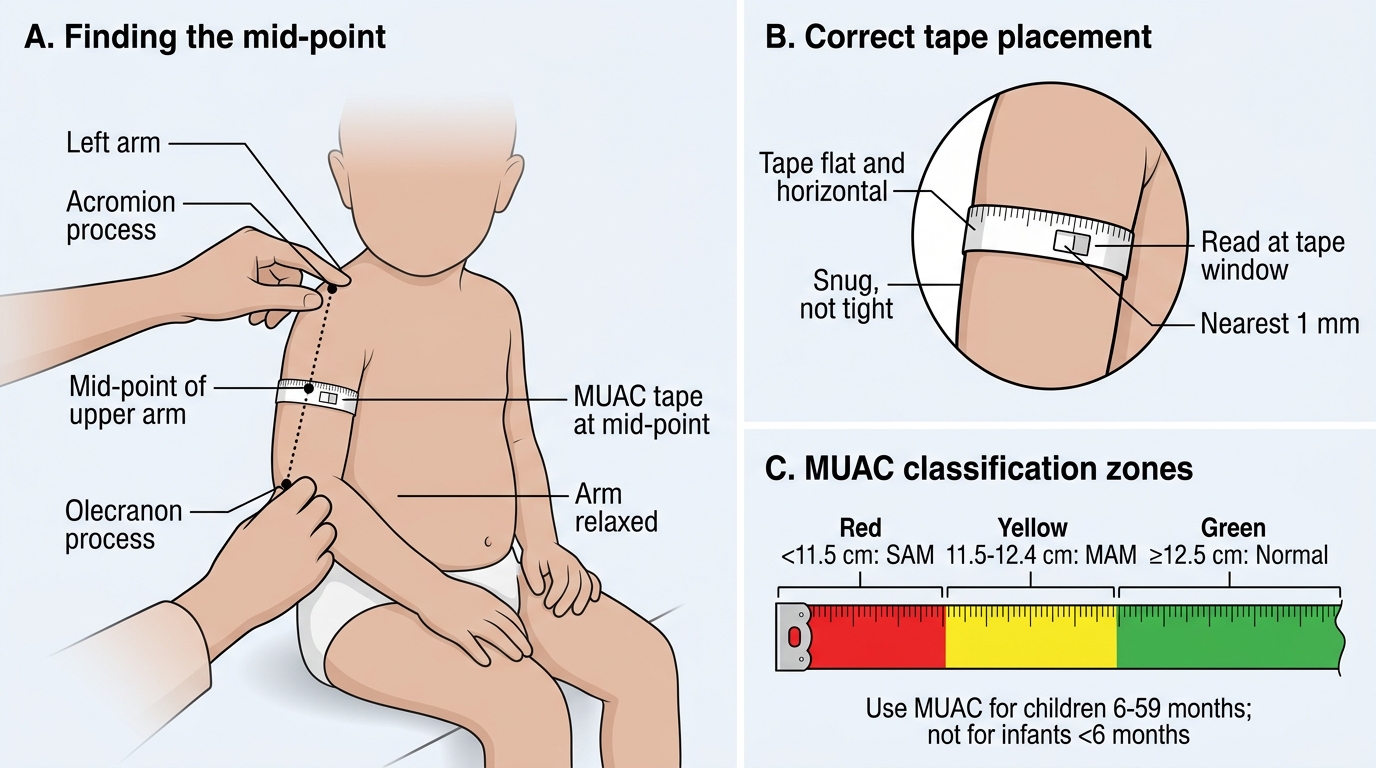
MUAC is measured on the left arm, at the mid-point between the tip of the shoulder (acromion) and the tip of the elbow (olecranon), with the arm hanging relaxed. The MUAC tape is applied snugly but without compressing the tissue. The measurement is read to the nearest 1 mm at the window in the tape. MUAC is validated for children 6–59 months; it is NOT used below 6 months.
Classification by MUAC:
• <11.5 cm = Severe Acute Malnutrition (SAM) — PINK: refer urgently to a Nutritional Rehabilitation Centre (NRC) or paediatric ward for therapeutic feeding. SAM children require specialised Ready-to-Use Therapeutic Food (RUTF), treatment of infections (universal antibiotic prophylaxis per NHM protocol), and correction of micronutrient deficiencies — management that cannot safely be provided at home.
• 11.5–12.4 cm = Moderate Acute Malnutrition (MAM) — YELLOW: refer to NRC outpatient programme or supplementary feeding programme. Supplement with RUTSF or equivalent. Advise increased dietary diversity and frequency.
• ≥12.5 cm = Normal nutrition (Green): counsel on adequate feeding, age-appropriate diet, continued breastfeeding.
Component 2 — Bilateral pedal oedema:
Press the dorsum of the foot with a thumb for 3 seconds — if a pit remains after release (pitting oedema), and it is present on BOTH feet, classify as oedematous malnutrition (Kwashiorkor) = PINK regardless of MUAC. Bilateral oedema is a sign of severe protein deficiency and carries high mortality risk.
Component 3 — Visual assessment:
Look for severe wasting — visible loss of muscle bulk and subcutaneous fat from the buttocks, thighs, and upper arms (the 'baggy pants' or 'old man' appearance). If severe wasting is visible, classify as SAM even if the MUAC measurement is borderline.
Correct MUAC Measurement and Classification
Risk Stratification and Final Classification
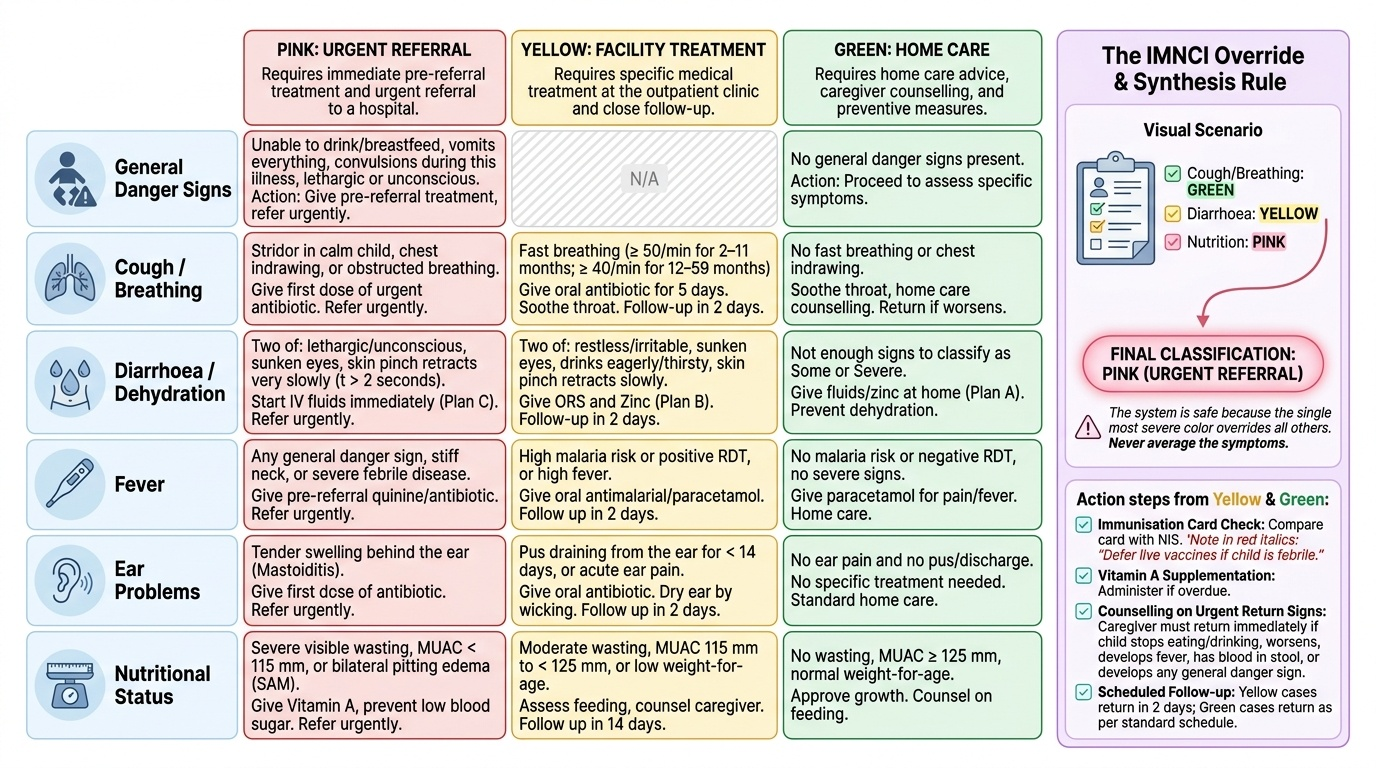
After completing all six assessment steps — danger signs, cough/breathing, diarrhoea/dehydration, fever, ear problems, and nutritional status — the IMNCI algorithm requires the health worker to compile the findings into a final classification that drives the management action. This synthesis step is where the 'integrated' in IMNCI is operationalised: multiple conditions assessed across multiple domains are reduced to a single, actionable decision. The final classification is always the MOST SEVERE colour found across all domains — this is the override rule that makes the system safe. Without the override rule, a health worker might correctly classify each domain individually but then average them — treating a child with Yellow for pneumonia and Yellow for dehydration at home, while missing a concurrent Pink finding for SAM. The IMNCI override rule eliminates this averaging error by requiring that the single most severe classification determines the action. Understanding this synthesis step is essential for the final-year student, because clinical examinations routinely present co-morbid cases where multiple domain classifications must be integrated into one coherent action plan.
Provided image
The final classification process in practice:
1. List all conditions assessed and their colours.
2. If any domain is Pink → overall action = PINK (urgent referral), regardless of other domains.
3. If no Pink, but one or more Yellow → overall action = YELLOW (facility treatment), addressing all Yellow conditions in the treatment plan.
4. If all domains Green → overall action = GREEN (home treatment with counselling).
For Yellow and Green cases, the health worker must also complete:
• Immunisation review: check the child's immunisation card against the NIS. Give any overdue vaccines if the child is not acutely ill. A febrile child should NOT receive live vaccines — defer.
• Vitamin A supplementation: give if overdue (6-monthly from 9 months per NIS).
• Counselling on return signs: instruct the caregiver to return immediately if any of these warning signs develop:
- Child stops eating or drinking
- Child worsens or develops fast breathing or chest indrawing
- Fever develops or recurs
- Blood in stool
- Child develops any general danger sign
• Follow-up visit: schedule based on severity — Yellow cases should return in 2 days; Green cases in 5 days or sooner if warning signs occur.
For Pink cases: write a complete referral note (age, weight, all findings, classification, any pre-referral treatment given) and accompany the caregiver to the referral transport if possible.
SELF-CHECK
An 18-month-old child is brought with diarrhoea for 3 days. On assessment: alert and restless, eyes sunken, skin turgor goes back slowly (1-2 seconds). MUAC measures 11.3 cm. No fast breathing. No danger signs. What is the final IMNCI classification and action?
A. Yellow — some dehydration; give ORS Plan B at facility and send home after 4 hours; follow up in 2 days
B. Pink — SAM (MUAC <11.5 cm) triggers urgent referral regardless of the dehydration severity
C. Yellow — treat some dehydration with Plan B AND refer for SAM management; both conditions require action
D. Green — the child is restless but not lethargic; dehydration is not severe
Reveal Answer
Answer: B. Pink — SAM (MUAC <11.5 cm) triggers urgent referral regardless of the dehydration severity
MUAC of 11.3 cm classifies as SAM (<11.5 cm) — this is a PINK classification requiring urgent referral to a Nutritional Rehabilitation Centre, regardless of other findings. The override rule means that even though the dehydration is 'some' (Yellow), the SAM classification (Pink) takes precedence and the final action is PINK. At the referral facility, both the dehydration (ORS/IV per severity) and the SAM (RUTF, antibiotic prophylaxis) will be managed together. Sending this child home after ORS Plan B (Option A) would address the dehydration but miss the life-threatening undernutrition — a classic single-domain error that IMNCI is specifically designed to prevent.
Applied Practice: Case-Based Classification Scenarios
Working through integrated case scenarios is the most effective way to consolidate IMNCI child assessment skill before a clinical posting. Applied practice closes the gap between knowing the algorithm theoretically and executing it fluently under the time pressure and emotional complexity of a real clinical encounter — a gap that cannot be bridged by re-reading the chart booklet alone. The following three scenarios are structured to mirror the OSPE format and include co-morbid findings that require the override rule. Each scenario is presented in the clinical encounter format: brief history, then findings in assessment order (danger signs → cough/breathing → diarrhoea → fever → ear → nutrition), then classification domain by domain, then the final action. Work through each scenario independently — classify each domain before reading the classification — then verify your answer against the model. Pay particular attention to scenarios where a single Pink-category finding changes the entire management from what a single-domain assessment would have recommended, as this is the canonical pattern tested in IMNCI examinations.
Case 1 — Child with cough and diarrhoea, 14 months:
Presentation: 2-day cough, 5-day diarrhoea. Fever 38.2°C. Weight 8 kg.
Assessment findings: Alert, drinking well, no danger signs. RR 52/min (confirmed). No chest indrawing. Eyes: moderately sunken. Skin turgor: goes back slowly (2 seconds). MUAC 13.0 cm.
Classification:
• Cough/breathing: RR 52/min at 14 months > 40/min threshold = fast breathing = Pneumonia (Yellow)
• Diarrhoea: restless/sunken eyes/slow skin turgor (two 'some' signs) = Some dehydration (Yellow)
• Nutrition: MUAC 13.0 cm = Normal (Green)
• Final action: YELLOW — treat pneumonia with oral amoxicillin 5 days; treat some dehydration with ORS Plan B (75 mL/kg over 4 hours at facility); give zinc 20 mg/day for 14 days; follow up in 2 days; counsel on danger signs.
Case 2 — Child with severe malnutrition, 2 years:
Presentation: brought for 'general weakness' and reduced eating for 2 weeks.
Assessment findings: Lethargic (danger sign present). RR 44/min. Eyes slightly sunken. Skin turgor goes back slowly. MUAC 10.8 cm. Bilateral pedal oedema present (pitting, both feet).
Classification:
• Danger sign: Lethargic = PINK immediately (general danger sign)
• Nutrition: MUAC 10.8 cm AND bilateral oedema = SAM = PINK (confirmed)
• Final action: PINK — urgent referral. Pre-referral: if lethargic and not drinking, give IV glucose (check blood glucose if available — SAM children are prone to hypoglycaemia). Referral note must document SAM with oedema + danger sign + vitals.
Case 3 — Febrile child with ear discharge, 3 years:
Presentation: fever 3 days, ear discharge from right ear for 3 weeks. No cough, no diarrhoea.
Assessment findings: Alert, drinking well. No danger signs. RR 32/min. No chest indrawing. No dehydration signs. MUAC 12.8 cm. Right ear: pus visible in canal, discharge for 3 weeks (>14 days). Behind ear: no swelling or tenderness. Fever 38.0°C, no rash, not in high-malaria zone.
Classification:
• Fever: low-grade, <7 days, no rash, no malaria zone = No malaria, no measles = fever without local cause (Yellow — give antipyretic; advise to return if fever persists >7 days)
• Ear: discharge ≥14 days = Chronic ear infection (Yellow — dry mopping + refer to ENT)
• Nutrition: MUAC 12.8 cm = Normal (Green)
• Final action: YELLOW (two Yellow conditions). Treat both; follow up in 2 days.
SELF-CHECK
During the nutritional assessment of a 3-year-old, the health worker measures MUAC over the right forearm because the child resisted having the left arm measured. The reading is 13.2 cm. What is the problem with this assessment?
A. No problem — MUAC can be measured on either arm as long as the same technique is used
B. MUAC must be measured on the LEFT arm at the mid-point; right-arm or wrong-site measurement invalidates the result and must be repeated
C. The problem is that 13.2 cm is in the MAM range — re-measure is needed only if the child resists
D. The forearm site is acceptable for children over 2 years when the upper arm is inaccessible
Reveal Answer
Answer: B. MUAC must be measured on the LEFT arm at the mid-point; right-arm or wrong-site measurement invalidates the result and must be repeated
IMNCI mandates MUAC measurement specifically on the LEFT upper arm at the mid-point between the shoulder tip and the elbow — this standardised site and side is the basis on which the cut-off values (<11.5 cm, 11.5–12.4 cm) were validated. Measuring on the right arm, or at the forearm, gives a different value (forearm circumference is smaller than upper-arm circumference) and cannot be interpreted against the validated cut-offs. The measurement must be repeated correctly on the left upper arm mid-point, even if the child resists — a second attempt with a caregiver's help is always appropriate.
Self-Assessment
The IMNCI child assessment algorithm is best tested through integrated case questions that require applying multiple steps simultaneously — because in clinical practice, danger signs, cough, dehydration, and malnutrition appear together, not one at a time. The following questions are structured to reflect the OSPE and short-answer formats used at NMC exit level. Work through each question fully before checking against the classification criteria in the earlier sections. Remember that the override rule is the single most commonly tested IMNCI principle in examination settings — any question that includes a Pink-level finding should prompt you to classify Pink regardless of how many Yellow or Green findings accompany it. Questions 4 and 5 specifically test PE16.6 (diarrhoeal dehydration) and PE16.4 (undernutrition identification and referral), both of which are demonstrated skill competencies at SH level.
- A 2-year-old child arrives with fever, fast breathing (42/min), and sunken eyes with slow skin turgor. No chest indrawing. Alert. MUAC 11.8 cm. List all IMNCI classifications, state the final action, and name the two treatments to give before/at the PHC.
- What is the IMNCI 'override rule'? Give a clinical example from paediatric practice where applying the override rule changes the action from what a single-symptom assessment would have done.
- A 15-month-old child has diarrhoea for 10 days, no blood in stool, no dehydration signs. What IMNCI classification does the 10-day duration trigger, and what additional assessment is needed?
- Describe the correct technique for MUAC measurement and state the three classification categories with their cut-off values and recommended actions.
- A febrile 4-year-old has a stiff neck, high temperature (39.5°C), and no source of fever on examination. What IMNCI classification does this attract and why?