Page 3 of 8
PH2.1-8 | Autonomic & Peripheral Nervous system, Autacoids — Part 3
PH2.1: Cholinergic Pharmacology
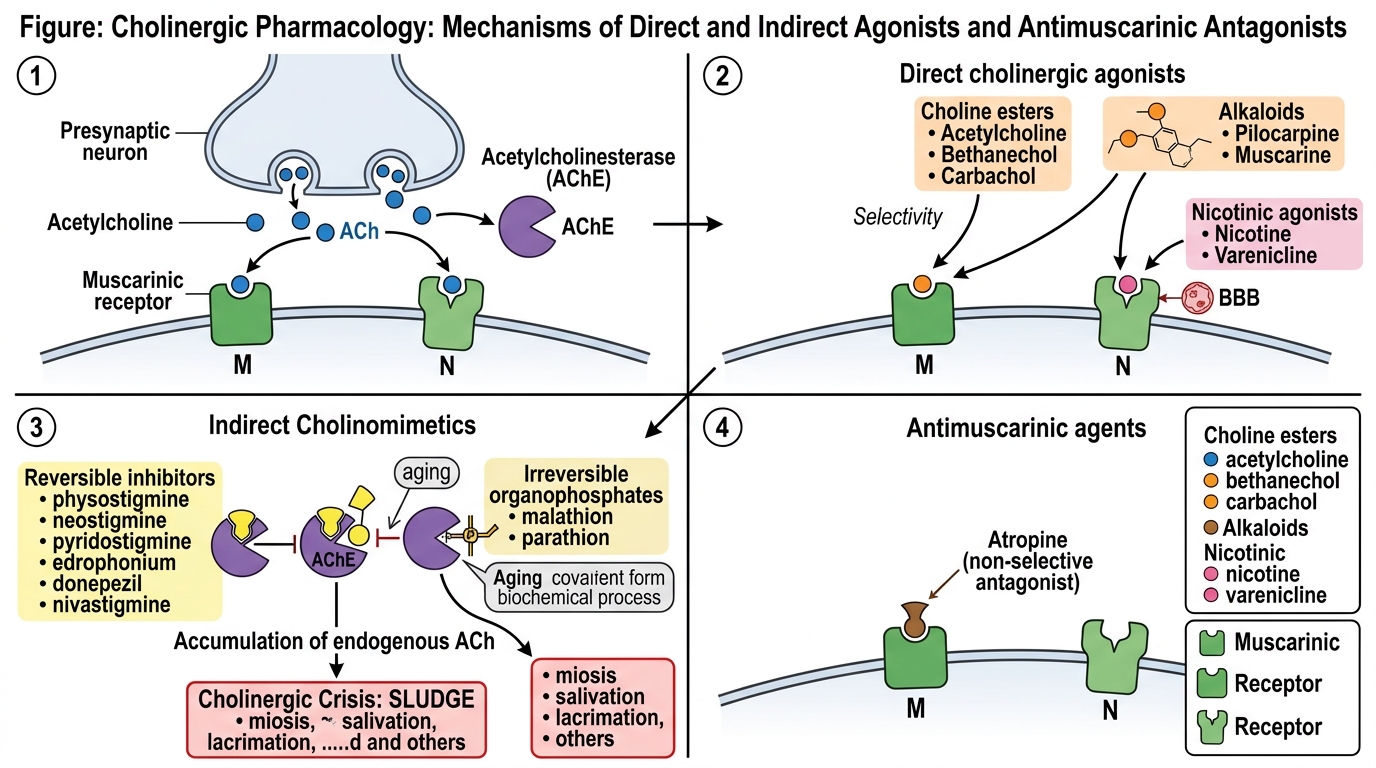
Cholinergic drugs act by either directly stimulating muscarinic and/or nicotinic receptors or indirectly by inhibiting acetylcholinesterase (AChE), thereby potentiating endogenous ACh.
Direct Cholinergic Agonists (Cholinomimetics)
Choline esters include acetylcholine (non-selective, rapidly hydrolyzed, no clinical use), bethanechol (muscarinic selective, resistant to AChE, used for postoperative urinary retention), and carbachol (muscarinic and nicotinic, used topically for glaucoma). Alkaloids like pilocarpine (muscarinic, crosses blood-brain barrier, used in glaucoma and xerostomia) and muscarine (toxic). Nicotinic agonists (nicotine, varenicline) are used in smoking cessation.
Indirect Cholinomimetics (Anticholinesterases)
Reversible agents include physostigmine (tertiary amine, crosses BBB, used in atropine overdose and glaucoma), neostigmine and pyridostigmine (quaternary amines, peripherally acting, mainstay of myasthenia gravis treatment), edrophonium (short-acting, diagnostic), and donepezil, rivastigmine (Alzheimer's disease). Irreversible organophosphates (malathion, parathion, nerve gases) phosphorylate AChE, causing aging of the enzyme; recovery requires synthesis of new enzyme. The cholinergic crisis manifests as miosis, salivation, lacrimation, urination, defecation, GI cramps, emesis (SLUDGE), plus bradycardia, bronchospasm, and neuromuscular paralysis.
Antimuscarinic Agents
Atropine is a non-selective competitive antagonist at muscarinic receptors. It increases heart rate (blocks M2), reduces secretions, relaxes smooth muscle, and causes mydriasis. Used for bradycardia, preanesthetic medication, organophosphate poisoning (large doses), and as antispasmodic. Adverse effects: dry mouth, tachycardia, blurred vision, urinary retention, hyperthermia. Scopolamine (hyoscine) depresses CNS, used for motion sickness. Ipratropium and tiotropium (quaternary) are inhaled M1/M3 antagonists for COPD and asthma. Pirenzepine is M1 selective, once used for peptic ulcer. Oxybutynin, tolterodine, solifenacin target M3 in bladder for overactive bladder. Tropicamide and cyclopentolate are short-acting mydriatics for fundoscopy.
Drug Table: Cholinergic Agonists and Antagonists
| Drug | Receptor / Action | Primary Use | Key Adverse Effects |
|------|-------------------|-------------|---------------------|
| Bethanechol | M3 agonist | Postoperative urinary retention | Abdominal cramps, diarrhea, flushing |
| Pilocarpine | M3 agonist | Glaucoma (topical) | Miosis, blurred vision, brow ache |
| Neostigmine | Reversible AChE inhibitor (peripheral) | Myasthenia gravis, reversal of NMBs | Salivation, muscle cramps, bradycardia |
| Physostigmine | Reversible AChE inhibitor (central+peripheral) | Atropine overdose, glaucoma | Seizures, bradycardia, hypotension |
| Atropine | Non-selective muscarinic antagonist | Bradycardia, organophosphate poisoning, preanesthetic | Dry mouth, tachycardia, urinary retention, hyperthermia |
| Ipratropium | M1/M3 antagonist (inhaled) | COPD, asthma | Dry mouth, cough, headache |
| Tiotropium | Long-acting M1/M3 antagonist (inhaled) | COPD maintenance | Dry mouth, pharyngitis |
| Oxybutynin | M3 antagonist | Overactive bladder | Dry mouth, constipation, blurred vision |
CLINICAL PEARL
Organophosphate poisoning is a major public health issue in agrarian India. Management centers on atropinization: administer atropine boluses (1–5 mg IV every 5–15 min) until tachycardia, dry skin, and dilated pupils appear—indicating competitive muscarinic blockade. Concomitantly, give pralidoxime (2-PAM, 1–2 g IV) within 24–48 hours to reactivate acetylcholinesterase before ‘aging’ of the enzyme-phosphate bond. In resource-limited settings, the absence of mechanical ventilation makes rapid atropinization life-saving. Always ensure decontamination (remove clothing, wash skin) to limit ongoing absorption. Avoid pralidoxime in carbamate poisoning. Awareness and availability of antidotes in primary health centers remain a challenge; simulation-based training can improve outcomes.
PH2.2: Adrenergic Pharmacology
Adrenoceptor agonists (sympathomimetics) are classified as direct-acting (catecholamines and non-catecholamines), indirect-acting (enhancing NE release or inhibiting reuptake), or mixed. They differ in receptor affinity, efficacy, and pharmacokinetics, shaping their therapeutic utility and adverse effect profile.
Direct Agonists
- Epinephrine (α1, α2, β1, β2): high affinity, given parenterally. In anaphylaxis, it reverses bronchospasm (β2), vasodilatation, and hypotension (α1 vasoconstriction); in cardiac arrest, it enhances myocardial contractility and heart rate (β1). Adverse: tachycardia, hypertension, arrhythmias, fear.
- Norepinephrine (α1, α2, β1): potent vasopressor, first-line in septic shock to maintain perfusion pressure. Extravasation causes tissue necrosis (α1).
- Dopamine (D1, β1, α): low dose dilates renal vessels (D1), moderate increases cardiac output (β1), high dose vasoconstriction (α). Uses: cardiogenic shock; controversy over renal protection.
- Dobutamine (β1 > β2): inotropic support in acute heart failure; less tachycardic than dopamine.
- Isoprenaline (β1=β2): bronchodilator, historically for asthma but replaced by selective β2 agents; used in bradyarrhythmias.
- Selective β2 agonists: salbutamol, terbutaline, formoterol (long-acting) – via inhalation for asthma and COPD, tocolysis. Adverse: tremor, palpitations, hypokalemia at high doses.
- α1 agonists: phenylephrine (nasal decongestant, vasopressor), oxymetazoline (nasal drops). Systemic absorption can cause hypertension and reflex bradycardia.
- Central α2 agonists: clonidine, methyldopa (prodrug) – reduce sympathetic outflow; used for hypertension (especially pregnancy). Side effects: sedation, dry mouth, rebound hypertension on abrupt withdrawal.
Indirect and Mixed
Amphetamines promote NE release, used in ADHD and narcolepsy. Cocaine blocks reuptake of catecholamines, leading to intense vasoconstriction and arrhythmias. Ephedrine (α, β, indirect) is used as vasopressor in obstetrics.
Adrenoceptor Antagonists
- α-blockers: non-selective (phenoxybenzamine, irreversible, used in pheochromocytoma) vs selective α1 (prazosin, terazosin, doxazosin, tamsulosin). α1 blockers reduce peripheral resistance and treat hypertension and BPH. Tamsulosin is uroselective (α1A), minimizing orthostatic hypotension. First-dose syncope is a concern.
- β-blockers: competitive antagonists at β receptors. Non-selective (propranolol, nadolol) block β1 and β2; cardioselective (atenolol, metoprolol, bisoprolol) preferentially block β1 at low doses. Intrinsic sympathomimetic activity (ISA) is seen with pindolol and acebutolol, causing less bradycardia. Additional properties: membrane stabilizing activity (local anesthetic effect, propranolol).
- Uses: hypertension, angina, myocardial infarction (secondary prevention), heart failure (carvedilol, metoprolol, bisoprolol – start low, go slow), arrhythmias, migraine prophylaxis, essential tremor, glaucoma (timolol).
- Adverse effects: bradycardia, heart failure, bronchospasm (β2 blockade), fatigue, cold extremities, nightmares (lipophilic drugs like propranolol), carbohydrate intolerance. Withdrawal syndrome: rebound angina, MI.
- Mixed α/β blockers: labetalol, carvedilol – useful in hypertensive emergencies and heart failure.
Drug Table: Adrenoceptor Agonists and Antagonists
| Drug | Receptor Selectivity | Clinical Use | Key Adverse Effects |
|------|----------------------|--------------|-------------------|
| Epinephrine | α1, α2, β1, β2 | Anaphylaxis, cardiac arrest | Tachycardia, hypertension, arrhythmias |
| Norepinephrine | α1, α2, β1 | Septic shock | Vasoconstriction, tissue necrosis |
| Salbutamol | β2 (inhaled) | Acute asthma, tocolysis | Tremor, palpitations, hypokalemia |
| Prazosin | α1 blocker | Hypertension, BPH | Postural hypotension, nasal stuffiness |
| Propranolol | β1, β2 blocker | Hypertension, migraine prophylaxis | Bronchospasm, bradycardia, fatigue |
| Atenolol | β1 selective blocker | Hypertension, angina | Bradycardia, less bronchospasm |
| Carvedilol | α1, β1, β2 blocker | Heart failure, hypertension | Dizziness, bradycardia, hypotension |
CLINICAL PEARL
Selecting a beta-blocker in an asthmatic patient with ischemic heart disease requires caution. Non-selective agents (propranolol, nadolol, timolol) are contraindicated because β2 blockade can precipitate severe bronchospasm. Even cardioselective beta1-blockers (atenolol, metoprolol, bisoprolol) lose selectivity at higher doses. In such patients, start with the lowest dose of a cardioselective agent, monitor peak expiratory flow rate, and ensure availability of rescue inhaled β2-agonists. If beta-blockers are contraindicated, consider alternative antianginal therapy like calcium channel blockers. Ophthalmic beta-blockers (timolol) used for glaucoma can be absorbed systemically and cause severe bronchospasm, a frequently overlooked cause of acute exacerbation in elderly Indian COPD patients. Always ask about eye drops.