Page 4 of 8
PH2.1-8 | Autonomic & Peripheral Nervous system, Autacoids — Part 4
PH2.3: Skeletal Muscle Relaxants
Skeletal muscle relaxants encompass neuromuscular blocking agents (NMBs) used for surgical relaxation and centrally acting agents for spasticity.
Neuromuscular Blocking Agents
NMBs interfere with cholinergic transmission at the motor end-plate.
- Depolarizing NMB: Succinylcholine (suxamethonium) is two ACh molecules linked together. It initially depolarizes the end-plate causing fasciculations, then persists, leading to desensitization block (Phase I). It has rapid onset (30-60 sec) and short duration (5-10 min) due to hydrolysis by plasma pseudocholinesterase. Used for rapid sequence intubation and short procedures. Adverse effects: hyperkalemia (dangerous in burns, trauma, denervation, prolonged immobilization), malignant hyperthermia (rare, genetic, treated with dantrolene), bradycardia (especially in children, structurally similar to ACh), increased intraocular and intragastric pressure, myalgia. Prolonged apnea occurs with atypical pseudocholinesterase.
- Non-depolarizing (competitive) NMBs: these block the nicotinic receptor without depolarizing it. They are classified by duration and elimination.
- Long-acting: pancuronium (vagolytic, increases heart rate; renally eliminated).
- Intermediate-acting: atracurium (spontaneous Hofmann elimination, no dependence on organ function; can cause histamine release, hypotension), cisatracurium (less histamine), vecuronium (minimal cardiovascular effects, hepatic metabolism), rocuronium (rapid onset, stable cardiovascular, hepatic elimination).
- Short-acting: mivacurium (metabolized by pseudocholinesterase, histamine release).
Reversal of non-depolarizing block: traditionally, neostigmine (anticholinesterase) combined with an antimuscarinic (glycopyrrolate or atropine) to prevent muscarinic effects; sugammadex, a modified γ-cyclodextrin, directly encapsulates rocuronium and vecuronium in plasma, rapidly terminating block regardless of depth, and is a significant advance.
Directly Acting and Centrally Acting Muscle Relaxants
- Dantrolene: inhibits ryanodine receptors, reducing Ca2+ release from sarcoplasmic reticulum. Drug of choice for malignant hyperthermia and neuroleptic malignant syndrome.
- Centrally acting agents for spasticity:
- Baclofen: GABAB agonist, oral or intrathecal (for severe spasticity).
- Tizanidine: central α2 agonist, reduces spasticity with less muscle weakness.
- Diazepam: facilitates GABA action, useful in acute muscle spasm but sedating.
Drug Table: Neuromuscular Blocking Agents
| Drug | Type | Onset/Duration | Metabolism/Elimination | Key Adverse Effects |
|------|------|----------------|------------------------|---------------------|
| Succinylcholine | Depolarizing | Ultra-rapid (30-60s), short (5-10min) | Plasma pseudocholinesterase | Hyperkalemia, malignant hyperthermia, bradycardia, myalgia |
| Atracurium | Non-depolarizing, intermediate | 2-3 min, 20-35 min | Hofmann elimination, non-enzymatic | Histamine release, hypotension |
| Vecuronium | Non-depolarizing, intermediate | 2-3 min, 25-40 min | Hepatic metabolism, renal | Minimal cardiovascular effects |
| Rocuronium | Non-depolarizing, intermediate (rapid onset) | 1-2 min, 30-40 min | Hepatic elimination | Few; can be reversed by sugammadex |
| Pancuronium | Non-depolarizing, long | 3-5 min, 60-90 min | Renal elimination | Tachycardia, hypertension (vagolytic) |

PH2.4: Autacoids
Autacoids are locally acting substances (histamine, serotonin, prostaglandins, leukotrienes, kinins) with intense pharmacological activity. Their agonists and antagonists have broad therapeutic applications.
Histamine and Antihistamines
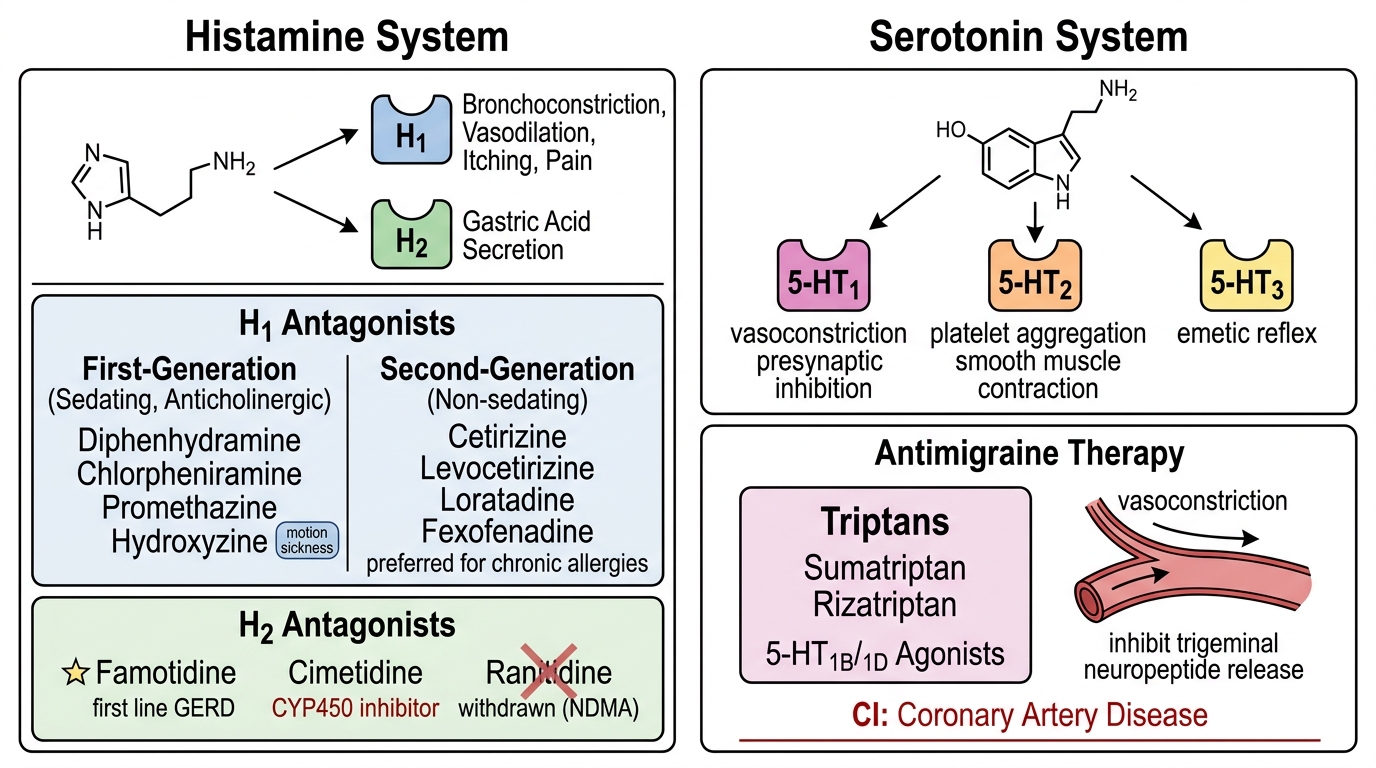
Histamine acts via H1 (bronchoconstriction, vasodilation, itching, pain) and H2 (gastric acid secretion) receptors. H1-receptor antagonists are subdivided into first-generation (sedating, anticholinergic: diphenhydramine, chlorpheniramine, promethazine, hydroxyzine) and second-generation (non-sedating: cetirizine, levocetirizine, loratadine, fexofenadine). Uses: allergic rhinitis, urticaria, pruritus, motion sickness (first-gen), as adjuvants in anaphylaxis. Second-gen agents are preferred for chronic allergies due to lack of sedation. H2 antagonists (ranitidine withdrawn due to NDMA contamination; famotidine, cimetidine) reduce gastric acid. Cimetidine inhibits CYP450, causing drug interactions; famotidine is first line for GERD and peptic ulcer disease.
Serotonin (5-HT) and Antimigraine Therapy
Serotonin is a neurotransmitter, local hormone, and precursor of melatonin. Key receptors: 5-HT1 (vasoconstriction, presynaptic inhibition), 5-HT2 (platelet aggregation, smooth muscle contraction), 5-HT3 (emetic reflex). Antimigraine drugs: acute attack treated with triptans (sumatriptan, rizatriptan) – 5-HT1B/1D agonists that constrict cranial vessels and inhibit trigeminal neuropeptide release. Contraindicated in coronary artery disease. Ergot alkaloids (ergotamine) are older, less selective, and cause more vasospasm. NSAIDs and antiemetics are added. Prophylaxis includes propranolol, flunarizine (calcium channel blocker; widely used in India for migraine prophylaxis and vertigo), valproate, topiramate, and amitriptyline. Antiemetic: ondansetron (5-HT3 antagonist) is highly effective for chemotherapy-induced vomiting.
Prostaglandins (PGs) and Leukotrienes
PGs are synthesized from arachidonic acid via COX-1 and COX-2 pathways. Misoprostol (PGE1 analogue) protects gastric mucosa and is used for NSAID-induced ulcers and medical abortion (in combination with mifepristone). Latanoprost (PGF2α analogue) increases uveoscleral outflow, a first-line glaucoma drug. Alprostadil (PGE1) is used for ductus arteriosus patency in neonates and erectile dysfunction. Carboprost (PGF2α) manages postpartum hemorrhage. NSAIDs block COX enzymes, reducing inflammation, pain, and fever. Leukotriene receptor antagonists (montelukast, zafirlukast) and 5-lipoxygenase inhibitor (zileuton) are used in asthma and allergic rhinitis.
Drug Table: Antihistamines
| Drug | Generation | Sedation | Anticholinergic | Primary Use |
|------|-----------|----------|----------------|-------------|
| Diphenhydramine | 1st | High | High | Allergic reactions, motion sickness |
| Chlorpheniramine | 1st | Moderate | Moderate | Allergic rhinitis, common cold |
| Cetirizine | 2nd | Low | Low | Allergic rhinitis, urticaria |
| Loratadine | 2nd | Minimal | Minimal | Allergic rhinitis, chronic urticaria |
| Fexofenadine | 2nd | Minimal | Minimal | Allergic rhinitis, minimal drug interactions |
SELF-CHECK
Self-Check
1. A 35-year-old woman with bronchial asthma and hypertension is prescribed a beta-blocker for migraine prophylaxis. Which of the following is most likely to precipitate an asthma exacerbation?
A. Atenolol 25 mg
B. Propranolol 40 mg
C. Bisoprolol 2.5 mg
D. Nebivolol 5 mg
Reveal Answer
Correct: B
2. A patient under general anesthesia received vecuronium. At the end of surgery, the anesthesiologist wishes to rapidly and completely reverse neuromuscular block. Which agent would specifically encapsulate vecuronium?
A. Sugammadex
B. Neostigmine
C. Edrophonium
D. Atropine
Reveal Answer
Correct: A
REFLECT
Reflect on a clinical encounter where ANS drugs played a pivotal role. Consider: Have you observed the use of salbutamol nebulization in acute asthma? How did you recognize potential adverse effects such as tremor or tachycardia? In patients on beta-blockers for heart failure, what monitoring parameters and counseling points are essential? When using topical timolol eye drops in an elderly patient with undiagnosed COPD, what symptoms might develop and how would you detect them? Contemplate the importance of drug choice in pregnancy and lactation for conditions like hypertension (e.g., methyldopa, labetalol). Write a short reflective note connecting pharmacological knowledge to your observation.
KEY TAKEAWAYS
Key Takeaways:
- Cholinergic agonists like pilocarpine and indirect agents like neostigmine are essential in glaucoma and myasthenia gravis.
- Antimuscarinics (atropine, ipratropium) block parasympathetic effects; atropine is life-saving in organophosphate poisoning.
- Adrenergic agonists (epinephrine, salbutamol) activate α/β receptors; epinephrine is the drug of choice in anaphylaxis.
- Beta-blockers reduce sympathetic activity; cardioselective agents are preferred in asthma but require caution.
- Depolarizing NMBs (succinylcholine) have a unique adverse profile; non-depolarizing agents are reversed by neostigmine or sugammadex.
- Autacoid antagonists (antihistamines, triptans, prostaglandin analogues) manage allergies, migraine, and glaucoma.
- Always consider receptor selectivity, dose-dependent effects, and drug interactions for safe prescribing.