Page 1 of 9
PY5.1-16 | Cardiovascular Physiology — SDL Guide
Learning Objectives
- Describe the functional anatomy of the heart as a pump, including the properties of cardiac muscle and the cardiac cycle (PY5.1)
- Describe the events of the cardiac cycle — atrial, ventricular systole and diastole — and correlate with heart sounds, pressure changes, volume changes, and ECG (PY5.2)
- Describe and discuss the origin, conduction, and spread of cardiac impulse through the heart's conduction system (PY5.3)
- Describe the normal electrocardiogram (ECG) — the genesis of each wave, normal values, and the standard leads (PY5.4)
- Describe the properties of cardiac muscle — automaticity, rhythmicity, conductivity, excitability, and contractility (PY5.5)
- Describe and discuss cardiac output, its regulation, and measurement methods including Fick's principle (PY5.6)
- Describe the factors affecting heart rate — neural, hormonal, and intrinsic (PY5.7)
- Describe the regulation of blood pressure — short-term (baroreceptors) and long-term (renal) mechanisms (PY5.8)
- Describe arterial blood pressure — systolic, diastolic, mean, pulse pressure — and the factors affecting them (PY5.9)
- Describe the arterial pulse — its genesis, characteristics, and clinical examination (PY5.10)
- Describe venous blood pressure, JVP waveform, and factors aiding venous return (PY5.11)
- Describe the microcirculation — capillary exchange, Starling forces, and oedema formation (PY5.12)
- Describe the regional circulation — coronary, cerebral, and splanchnic circulations (PY5.13)
- Describe the cardiovascular responses to exercise and changes in posture (PY5.14)
- Describe the pathophysiology of shock — types, compensatory mechanisms, and stages (PY5.15)
- Describe the pathophysiology of heart failure — causes, compensatory mechanisms, and clinical features (PY5.16)
INSTRUCTIONS
This module covers cardiovascular physiology — how the heart pumps blood, how blood pressure is regulated, what the ECG tells you, and what happens when the system fails. You will learn why the heart beats without being told to, how a 300-gram muscle pumps 7,000 litres of blood every day, and why a fall in blood pressure triggers an immediate rescue response.
Parallel connections: In Anatomy, you have just studied the heart and pericardium (AN22) — the chambers, valves, and coronary arteries. Now we see that structure in ACTION. In Biochemistry, lipid metabolism (BI4) explains how atherosclerosis blocks the coronary arteries — the number one killer worldwide.
References
- Guyton and Hall Textbook of Medical Physiology, 14th ed., Unit IV: The Circulation (textbook)
- Ganong's Review of Medical Physiology, 26th ed., Section V: Cardiovascular Physiology (textbook)
- OpenStax Anatomy and Physiology 2e, Chapter 19-20: Cardiovascular System (CC BY 4.0) (textbook (CC BY 4.0))
- B.D. Chaurasia's Human Anatomy, Vol. 1 — Heart and Pericardium (for structural reference) (atlas)
Version 2.0 | NMC CBUC 2024, Adapted from OpenStax A&P 2e (CC BY 4.0)
CLINICAL SCENARIO
Your heart pumps 7,000 litres of blood per day — enough to fill a small tanker truck. It beats about 100,000 times a day, 3 billion times in a lifetime, and it never takes a holiday. How does a fist-sized muscle do this? The answer lies in an elegant cycle of filling and emptying that repeats every 0.8 seconds — the cardiac cycle. By the end of this section, you'll understand every phase of that cycle, why you hear 'lub-dub' with a stethoscope, and how the heart adjusts its output from 5 L/min at rest to 25 L/min during a sprint.
WHY THIS MATTERS
As a doctor, the cardiac cycle is not abstract physiology — it's what you hear every time you place a stethoscope on a patient's chest. Understanding the cycle tells you what each heart sound means, why murmurs occur at specific times, what cardiac output means for tissue perfusion, and why heart failure is fundamentally a failure of the pump. Every decision in cardiology, anaesthesia, surgery, and emergency medicine depends on understanding how this pump works.
RECALL
From Anatomy (AN22), you know the heart has four chambers — two atria (receiving chambers) and two ventricles (pumping chambers). You know the AV valves (mitral and tricuspid) guard the AV orifices, and the semilunar valves (aortic and pulmonary) guard the outflow tracts. You know the coronary arteries supply the heart muscle itself. Now we ask: how do these structures work together as a coordinated pump?
Properties of Cardiac Muscle (PY5.1, PY5.5)
Cardiac muscle is unique — it shares features with both skeletal and smooth muscle, yet has properties found in neither.

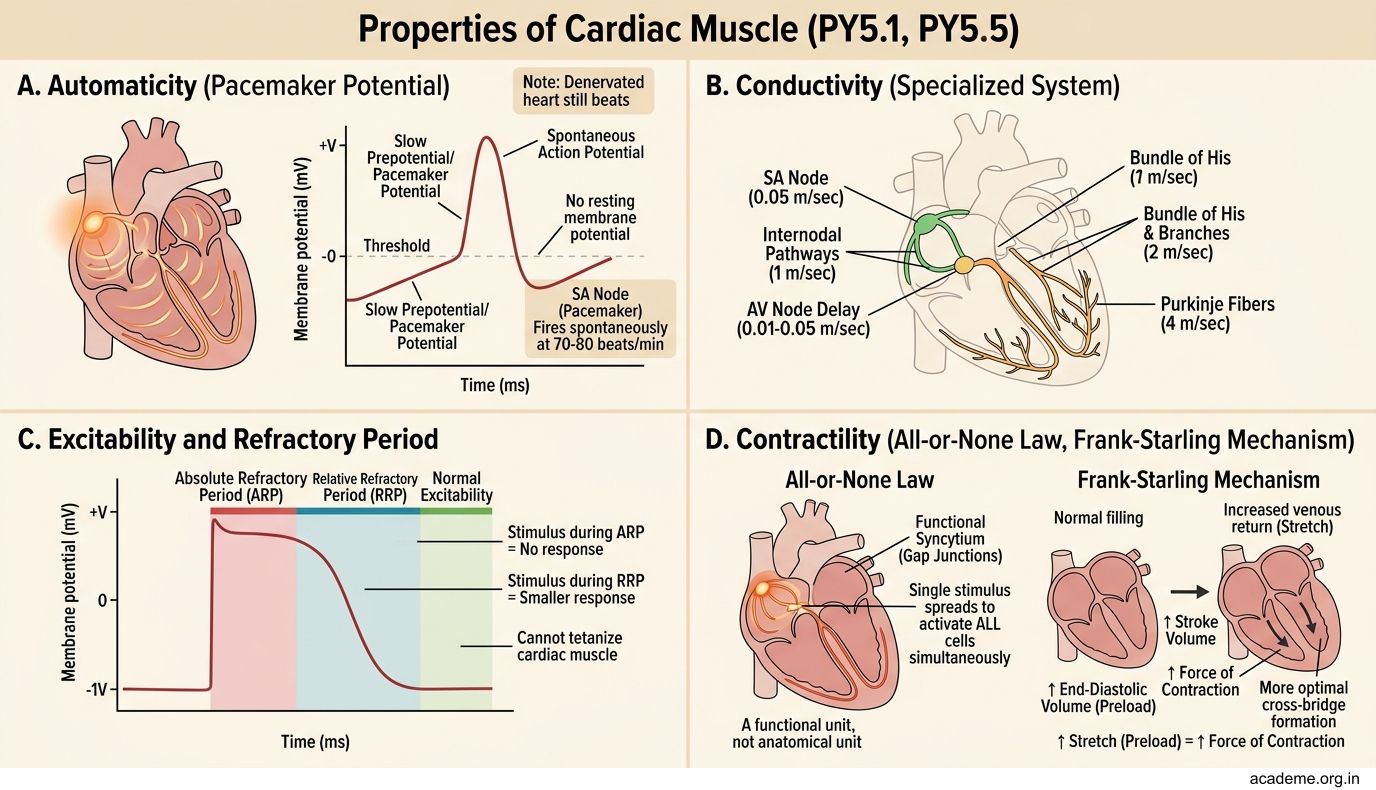
Figure: Properties of Cardiac Muscle (PY5.1, PY5.5)

Figure: Properties of Cardiac Muscle (PY5.1, PY5.5)
Five special properties of cardiac muscle:
- Automaticity (self-excitation) — cardiac muscle can generate its own action potentials WITHOUT neural input. The SA node (sinoatrial node) is the 'pacemaker' — it fires spontaneously at ~70-80 beats/min. Even a denervated heart (after transplant) keeps beating.
- Rhythmicity — the SA node fires at a regular rhythm. Each part of the conduction system has an intrinsic rate: SA node ~70-80/min, AV node ~40-60/min, Purkinje fibres ~15-40/min. The fastest pacemaker controls the heart — normally the SA node.
- Conductivity — the action potential spreads from cell to cell through gap junctions (intercalated discs). This makes the entire atrium (or ventricle) contract as a single unit — a functional syncytium. The atria and ventricles are electrically insulated from each other by the fibrous skeleton of the heart; the ONLY electrical connection between them is the AV bundle (Bundle of His).
- Excitability — cardiac muscle responds to stimuli with an action potential. But unlike skeletal muscle, it has a long refractory period (~250 ms) because of the prolonged plateau phase (Phase 2) of the cardiac action potential. This prevents tetanus — the heart cannot sustain a continuous contraction, which would be fatal.
- Contractility — the force of contraction can be increased (positive inotropic effect) by sympathetic stimulation, catecholamines, digoxin, or increased calcium. Decreased contractility (negative inotropic effect) occurs with heart failure, acidosis, or beta-blockers.
The cardiac action potential has 5 phases (0-4), unlike the simple depolarization-repolarization of skeletal muscle. The key difference is Phase 2 (plateau) — a sustained inflow of Ca2+ through L-type calcium channels that maintains depolarization for ~200-300 ms. This plateau is responsible for the long refractory period and for triggering contraction via calcium-induced calcium release (CICR) from the sarcoplasmic reticulum.
The Cardiac Cycle (PY5.2)
The cardiac cycle is one complete sequence of contraction and relaxation of the heart. At a heart rate of 75 bpm, one cycle = 0.8 seconds.

Figure: The Cardiac Cycle (PY5.2)
The cycle has 7 phases — follow this sequence carefully:
1. Atrial systole (0.1 s) — The atria contract, pushing the final 20-30% of blood into the ventricles (the 'atrial kick'). The ventricles are already ~70% filled from passive filling during diastole. P wave on ECG precedes this.
2. Isovolumetric (isovolumic) ventricular contraction (0.05 s) — The ventricles begin contracting. Pressure rises rapidly. Both AV valves AND semilunar valves are CLOSED — so volume doesn't change. First heart sound (S1, 'lub') occurs here — caused by closure of the AV valves (mitral and tricuspid).
3. Rapid ventricular ejection (0.1 s) — When ventricular pressure exceeds aortic/pulmonary pressure, the semilunar valves open. Blood rushes out. About 70% of stroke volume is ejected in this phase.
4. Reduced ventricular ejection (0.15 s) — Ejection slows as the pressure gradient decreases. T wave on ECG occurs during this phase (ventricular repolarization).
5. Isovolumetric ventricular relaxation (0.08 s) — The ventricles relax. Pressure drops rapidly. Both semilunar AND AV valves are CLOSED — volume doesn't change again. Second heart sound (S2, 'dub') occurs here — caused by closure of the semilunar valves (aortic and pulmonary).
6. Rapid ventricular filling (0.1 s) — When ventricular pressure falls below atrial pressure, the AV valves open. Blood rushes in passively (no atrial contraction needed). Third heart sound (S3) may be heard here — caused by rapid filling stretching the ventricular wall. Normal in children, pathological in adults (indicates heart failure with a dilated, compliant ventricle).
7. Reduced ventricular filling (diastasis) (0.2 s) — Filling slows as atrial and ventricular pressures equalize. Then the P wave fires and the cycle repeats.
Key numbers: End-diastolic volume (EDV) = ~120 mL; End-systolic volume (ESV) = ~50 mL; Stroke volume (SV) = EDV - ESV = ~70 mL; Ejection fraction = SV/EDV = ~58-60%.

Heart Sounds and Cardiac Output (PY5.2, PY5.6)
Heart sounds in clinical practice:

Figure: Heart Sounds and Cardiac Output (PY5.2, PY5.6)

Figure: Heart Sounds and Cardiac Output (PY5.2, PY5.6)
- S1 ('lub') — AV valve closure. Best heard at the apex (mitral area, 5th intercostal space, mid-clavicular line). Marks the START of ventricular systole.
- S2 ('dub') — Semilunar valve closure. Best heard at the base (aortic area = right 2nd intercostal space; pulmonary area = left 2nd intercostal space). Marks the END of ventricular systole. S2 normally splits during inspiration (A2 before P2) because the right ventricle takes slightly longer to empty.
- S3 — Rapid ventricular filling. Low-pitched, best heard at the apex with the bell of the stethoscope. Normal in children and young adults; pathological in older adults (indicates volume overload, heart failure).
- S4 — Atrial contraction into a stiff ventricle. Occurs just before S1. Always pathological — indicates decreased ventricular compliance (hypertrophic cardiomyopathy, hypertensive heart disease).
Cardiac output (CO) = Heart Rate x Stroke Volume = ~75 x 70 mL = ~5.25 L/min at rest.
Regulation of cardiac output:
- Preload (Frank-Starling mechanism) — the more the heart is filled (increased venous return), the more it stretches, and the more forcefully it contracts. Within physiological limits, 'the heart pumps whatever comes to it.' This is the most important intrinsic mechanism.
- Afterload — the resistance the ventricle must overcome to eject blood (primarily arterial blood pressure). Increased afterload = decreased stroke volume (the heart works harder but pumps less).
- Contractility — the force of contraction independent of preload/afterload. Sympathetic stimulation increases contractility (positive inotropic effect). Heart failure decreases contractility.
- Heart rate — regulated by the autonomic nervous system. Sympathetic increases HR; parasympathetic (vagus) decreases HR. The vagus is dominant at rest (resting vagal tone).
Measurement of CO — Fick's principle: CO = O2 consumption / (arteriovenous O2 difference). If the body consumes 250 mL O2/min, and arterial blood carries 200 mL O2/L while venous blood carries 150 mL O2/L, then CO = 250 / (200-150) = 250/50 = 5 L/min.
SELF-CHECK
During isovolumetric ventricular contraction, which valves are open and which are closed?
A. AV valves open, semilunar valves closed
B. All four valves closed
C. AV valves closed, semilunar valves open
D. All four valves open
Reveal Answer
Answer: B. All four valves closed
During isovolumetric contraction, ALL FOUR valves are closed. The AV valves have just closed (causing S1), and the semilunar valves haven't opened yet (ventricular pressure hasn't exceeded aortic/pulmonary pressure). Similarly, during isovolumetric relaxation, all four valves are closed — semilunar valves have just closed (causing S2), and AV valves haven't opened yet.