Page 2 of 9
PY5.1-16 | Cardiovascular Physiology — SDL Guide (Part 2)
Arterial Blood Pressure (PY5.9, PY5.10)
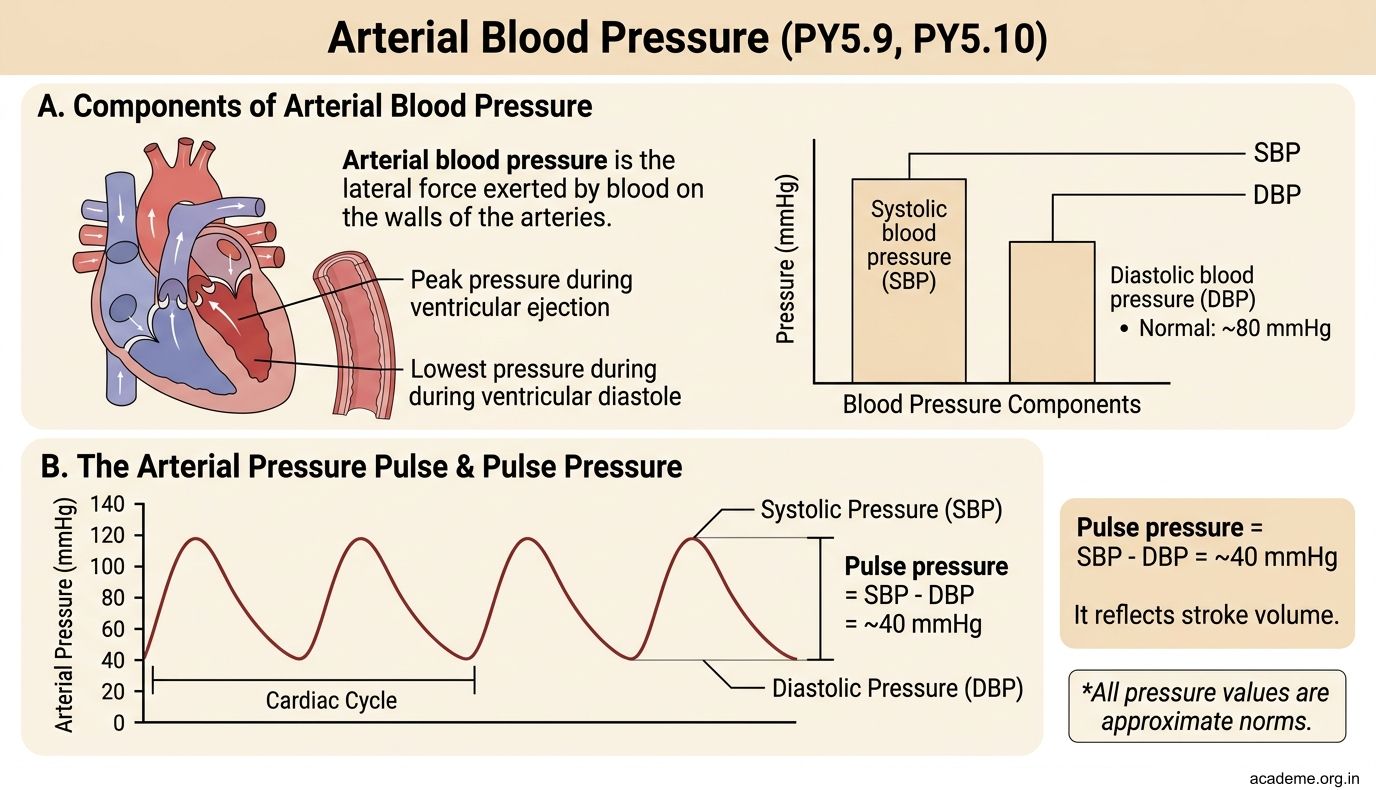
Arterial blood pressure is the lateral force exerted by blood on the walls of the arteries. It has two components:

Figure: Arterial Blood Pressure (PY5.9, PY5.10)

Figure: Arterial Blood Pressure (PY5.9, PY5.10)
- Systolic blood pressure (SBP) — the peak pressure during ventricular ejection. Normal: ~120 mmHg.
- Diastolic blood pressure (DBP) — the lowest pressure during ventricular diastole. Normal: ~80 mmHg.
- Pulse pressure = SBP - DBP = ~40 mmHg. It reflects stroke volume and arterial compliance.
- Mean arterial pressure (MAP) = DBP + 1/3(Pulse pressure) = 80 + 1/3(40) = ~93 mmHg. MAP is the average pressure driving blood through the systemic circulation. MAP below 60 mmHg = inadequate organ perfusion.
Factors affecting arterial BP:
1. Cardiac output (CO) — BP = CO x Total Peripheral Resistance (TPR)
2. Peripheral resistance — mainly determined by arteriolar smooth muscle tone
3. Blood volume — more volume = more pressure (think: overfilled balloon)
4. Elasticity of arterial walls — loss of elasticity (arteriosclerosis) increases systolic BP and pulse pressure
5. Viscosity of blood — increased viscosity (polycythaemia) increases resistance
The arterial pulse (PY5.10) — the pressure wave that travels along the arterial wall with each heartbeat. It travels much faster (4-12 m/s) than the blood itself (~0.5 m/s). The radial pulse at the wrist is where you routinely feel it.
Characteristics to assess: Rate, Rhythm, Volume (amplitude), Character (contour), Condition of the arterial wall, Symmetry (compare both sides).
Abnormal pulses: Pulsus paradoxus (exaggerated fall in BP during inspiration — cardiac tamponade), water-hammer pulse (wide pulse pressure — aortic regurgitation), pulsus alternans (alternating strong and weak beats — left ventricular failure).
Venous Pressure and JVP (PY5.11)
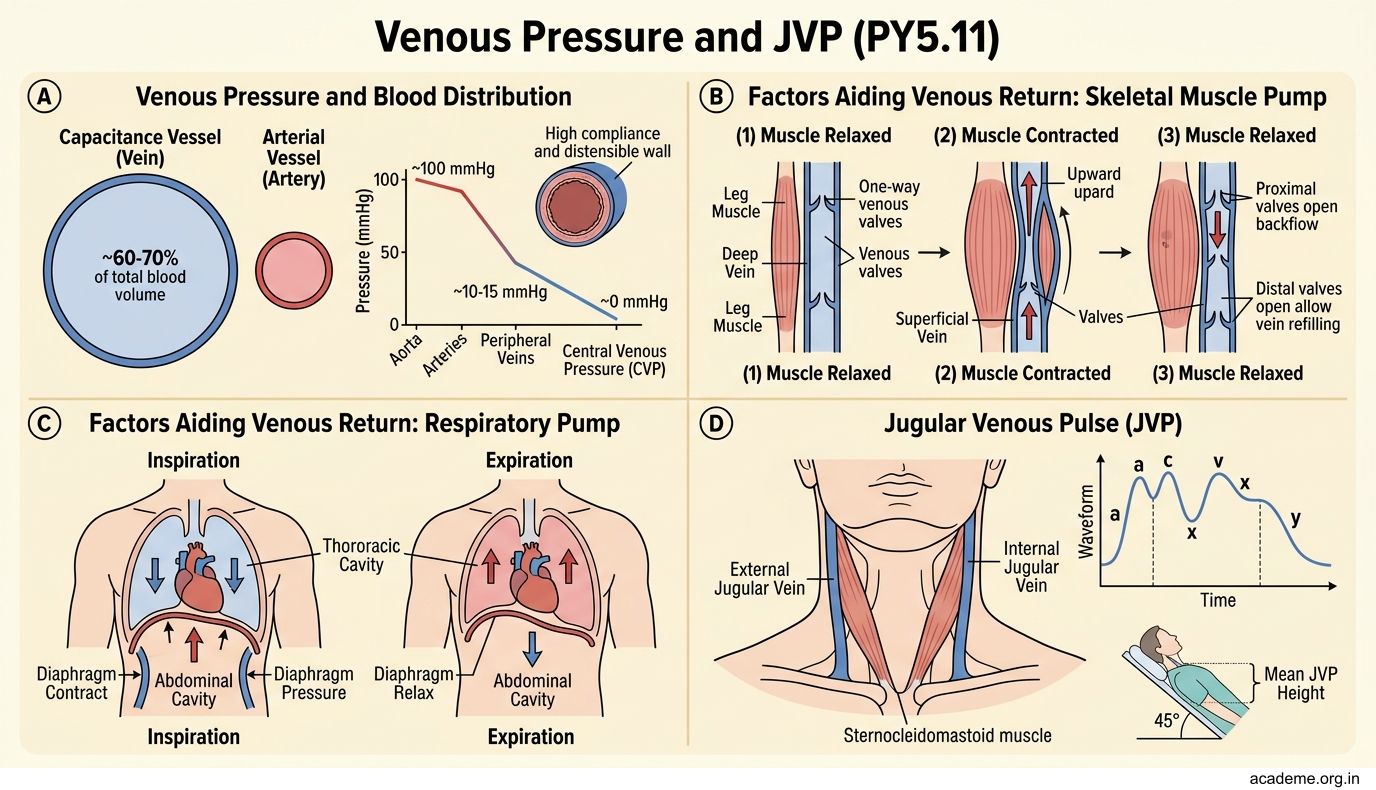
Venous blood pressure is much lower than arterial — about 10-15 mmHg in peripheral veins, falling to nearly 0 mmHg in the right atrium (central venous pressure, CVP). The veins are a capacitance system — they hold ~60-70% of total blood volume.

Figure: Venous Pressure and JVP (PY5.11)
Factors aiding venous return:
1. Skeletal muscle pump — contraction of leg muscles squeezes blood upward through one-way venous valves ('peripheral heart')
2. Respiratory pump — inspiration decreases intrathoracic pressure, creating a suction effect on the great veins
3. Venous valves — prevent backflow (especially important in the lower limbs)
4. Sympathetic venoconstriction — reduces venous capacitance, pushing blood toward the heart
5. Cardiac suction — ventricular relaxation creates a suction effect
6. Vis a tergo — the 'push from behind' — the residual pressure from arterial blood flowing through capillaries into veins
Jugular Venous Pressure (JVP) — examined in the internal jugular vein, it reflects right atrial pressure. The JVP waveform has 3 positive waves (a, c, v) and 2 descents (x, y):
- a wave — atrial contraction (right atrial systole)
- c wave — bulging of the tricuspid valve into the right atrium at the start of ventricular systole
- x descent — atrial relaxation + descent of the AV ring during ventricular systole
- v wave — passive filling of the right atrium while the tricuspid valve is closed
- y descent — opening of the tricuspid valve, blood flowing from atrium into ventricle
Clinical significance: Raised JVP = right heart failure, fluid overload, cardiac tamponade. Giant 'a' waves = tricuspid stenosis, pulmonary hypertension. Cannon 'a' waves = complete heart block (atrium contracts against a closed tricuspid valve). Absent 'a' waves = atrial fibrillation.
Blood Pressure Regulation — Baroreceptors and Beyond (PY5.8)
Blood pressure must be maintained within a narrow range — too low and organs don't get blood; too high and vessels are damaged. The body has short-term and long-term mechanisms.

Figure: Blood Pressure Regulation — Baroreceptors and Beyond (PY5.8)

Figure: Blood Pressure Regulation — Baroreceptors and Beyond (PY5.8)
SHORT-TERM REGULATION (seconds to minutes) — Neural:
- Baroreceptor reflex — THE most important short-term mechanism. Baroreceptors are stretch receptors in the carotid sinus (CN IX — glossopharyngeal nerve) and aortic arch (CN X — vagus nerve). When BP rises: baroreceptors fire more -> nucleus tractus solitarius (NTS) in medulla -> increased parasympathetic output (vagus) + decreased sympathetic output -> decreased HR, decreased contractility, vasodilation -> BP falls. When BP falls: the opposite occurs.
The baroreceptor reflex operates continuously — it is the reason your BP doesn't crash every time you stand up.
- Chemoreceptor reflex — peripheral chemoreceptors in the carotid body and aortic body respond to hypoxia, hypercapnia, and acidosis. They primarily regulate respiration but also cause vasoconstriction (increasing BP) when stimulated.
- CNS ischaemic response (Cushing response) — when cerebral blood flow is severely reduced, the vasomotor centre fires massively, causing intense vasoconstriction and hypertension. This is a last-resort mechanism — it operates only at MAP < 60 mmHg. The Cushing triad (hypertension + bradycardia + irregular respiration) is a sign of raised intracranial pressure.
LONG-TERM REGULATION (hours to days) — Renal and Hormonal:
- Renin-Angiotensin-Aldosterone System (RAAS) — when renal perfusion falls, the kidneys secrete renin -> angiotensinogen is converted to angiotensin I -> ACE (in lung capillaries) converts it to angiotensin II -> vasoconstriction + aldosterone release (Na+ and water retention) -> increased blood volume and BP.
- ADH (vasopressin) — released from the posterior pituitary when osmolarity rises or blood volume falls. Causes water retention and vasoconstriction.
- ANP (atrial natriuretic peptide) — released from atrial myocytes when the atria are stretched (volume overload). Causes Na+ and water excretion, vasodilation -> reduces BP. It opposes RAAS.
- Pressure natriuresis — the ultimate long-term mechanism. When BP rises, the kidneys excrete more Na+ and water, reducing blood volume until BP returns to normal. Guyton called this the 'infinite gain' mechanism — given enough time, it can return BP to its set point regardless of what other mechanisms do.
SELF-CHECK
A medical student stands up quickly from a lying position and feels dizzy for a few seconds before the feeling passes. Which reflex is primarily responsible for the rapid compensation that prevents the student from fainting?
A. Chemoreceptor reflex
B. Baroreceptor reflex
C. Renin-angiotensin-aldosterone system
D. CNS ischaemic response (Cushing response)
Reveal Answer
Answer: B. Baroreceptor reflex
The baroreceptor reflex is the primary short-term mechanism. On standing, blood pools in the lower limbs -> venous return falls -> CO and BP drop -> baroreceptors detect decreased stretch -> sympathetic activation (vasoconstriction + increased HR) corrects BP within seconds. RAAS takes hours. The Cushing response only activates at dangerously low MAP. Chemoreceptors primarily regulate respiration.