Page 1 of 11
PS7.1 | Anxiety Disorders in Primary Care — SDL Guide
Learning Objectives
- Recognise the clinical presentation of GAD, Panic Disorder, Social Anxiety Disorder, and Specific Phobia
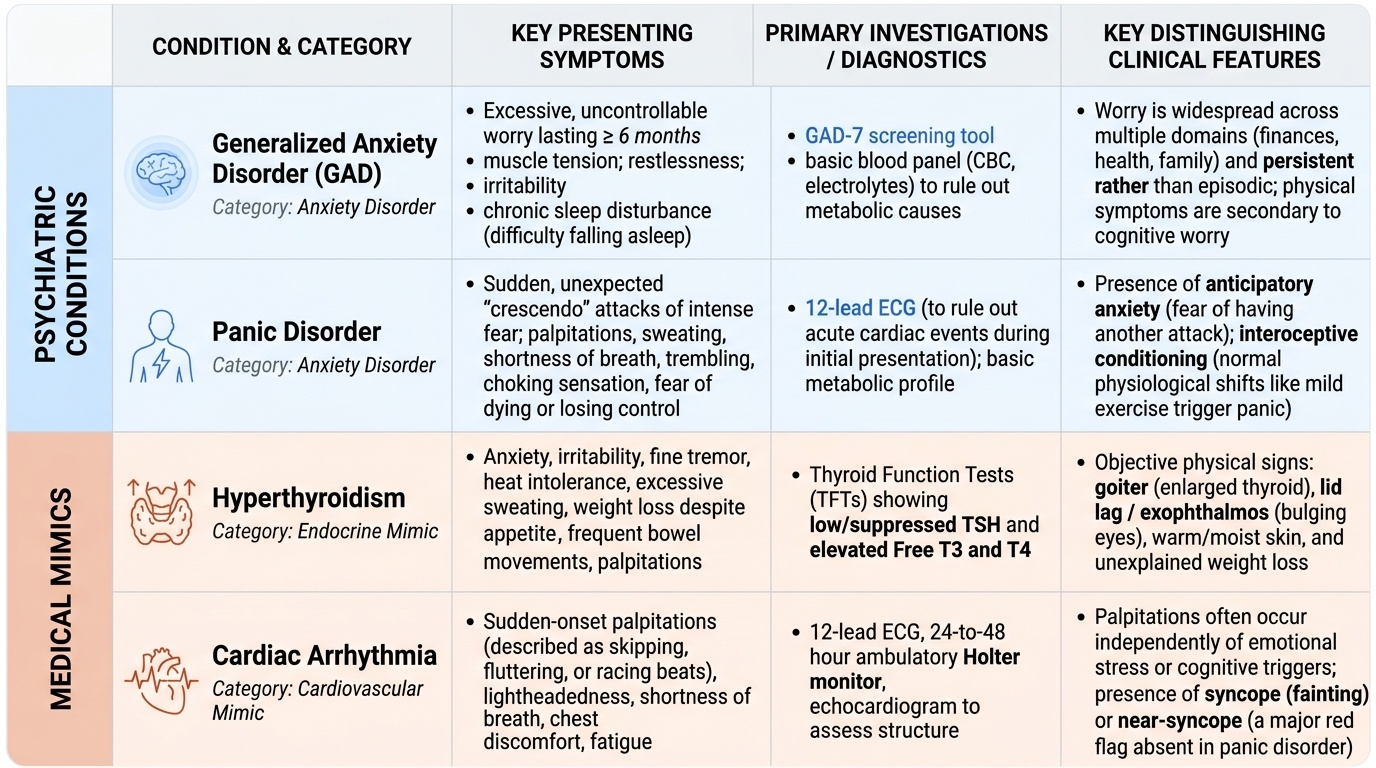
- Distinguish anxiety disorders from medical mimics such as hyperthyroidism and cardiac arrhythmia
- Apply DSM-5 diagnostic criteria for the common anxiety disorders, citing duration thresholds with their classification system
- Formulate an evidence-based management plan: SSRIs as first-line pharmacotherapy and CBT as psychological treatment
- Identify the appropriate use and limitations of benzodiazepines, and explain the dependence risk to patients
- Determine when a patient with anxiety disorder requires referral to secondary psychiatric services
INSTRUCTIONS
Anxiety disorders are the most prevalent mental health conditions in primary care worldwide, yet they are frequently unrecognised and undertreated. Missed diagnosis leads to unnecessary medical investigations, patient distress, and avoidable morbidity. As a Year-3 student soon entering internship, you will encounter anxious patients in every clinical posting — as the general practitioner in a community health centre, you need to diagnose and initiate treatment without delay. This module provides the skills to do so confidently and safely.
References
- Ahuja N. A Short Textbook of Psychiatry, 8th ed. Jaypee Brothers, 2022. Ch. 7: Anxiety and Related Disorders (textbook)
- Kaplan & Sadock's Synopsis of Psychiatry, 12th ed. Wolters Kluwer, 2022. Ch. 13: Anxiety Disorders (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
Clinical scenario: A 34-year-old schoolteacher presents to your primary health centre with a 9-month history of 'constant tension.' She reports waking up most mornings with a tight chest, cannot stop worrying about her daughter's school performance, her husband's job security, and whether she will be able to pay the rent. She knows the worries are disproportionate but cannot switch them off. She has visited a cardiologist twice — ECG and echocardiogram were normal. Her thyroid-stimulating hormone (TSH) was 2.1 mIU/L. She is sleeping poorly, feels fatigued throughout the day, and finds it increasingly difficult to concentrate on lessons. Today she broke down at the clinic: 'Doctor, I think I'm going mad.'
What is the most likely diagnosis? How will you distinguish it from other conditions? What treatment will you start today, and what will you tell her about her prognosis?
WHY THIS MATTERS
Anxiety disorders are the most prevalent class of psychiatric illness globally, affecting approximately 1 in 13 people at any point. In Indian primary care settings, studies estimate that 15–30% of adult attendees have a clinically significant anxiety disorder — the majority of them undiagnosed. As an intern or junior resident in a government PHC, a district hospital, or a general practice, you will not have a psychiatrist in the next room. The expectation under NMC Competency PS7.1 is explicit: you must be able to diagnose and manage anxiety disorders at primary care level. The skills you build today — pattern recognition, evidence-based pharmacotherapy, and CBT psychoeducation — will directly reduce patient suffering in your first posting.
RECALL
Before we map out anxiety disorders, let us recall two pieces of prior science that underpin today's learning.
First, from Physiology (PY): the autonomic nervous system has a sympathetic (fight-or-flight) and parasympathetic (rest-and-digest) limb. Sympathetic activation — mediated by noradrenaline at synapses and adrenaline from the adrenal medulla — produces tachycardia, palpitations, sweating, pupillary dilatation, hyperventilation, tremor, and dry mouth. Anxiety disorders involve sustained or easily triggered activation of this system in the absence of real external threat.
Second, from Medicine/Pharmacology (PH): hyperthyroidism increases adrenergic sensitivity, producing symptoms almost identical to anxiety — palpitations, sweating, irritability, weight loss, heat intolerance. A TSH measurement is therefore a mandatory investigation before diagnosing a primary anxiety disorder. Similarly, caffeine, sympathomimetic decongestants, and stimulant drugs can provoke anxiety-like states. Substance withdrawal (especially from alcohol or benzodiazepines) can mimic acute anxiety. Always screen for these before attributing symptoms to a primary psychiatric cause.
Recognising Anxiety Disorders: Clinical Presentation
Anxiety disorders share a common substrate — excessive, disabling fear or worry — but differ in their trigger, pattern, and duration. The primary care physician's task is to identify the predominant symptom cluster and map it to the correct diagnosis. This determines both the treatment choice and the prognosis.
Generalised Anxiety Disorder (GAD) presents as pervasive, free-floating worry about multiple everyday domains (finances, health, family, work), present on more days than not. The patient typically cannot control the worry and experiences associated features: restlessness, easy fatigability, difficulty concentrating, irritability, muscle tension, and disturbed sleep. It is the 'always-on' form of anxiety — unlike panic disorder, there are no discrete sudden attacks. GAD is the most common anxiety disorder seen in primary care and is frequently comorbid with depression.
Panic Disorder presents with recurrent, unexpected panic attacks — discrete surges of intense fear that peak within minutes and include ≥4 of 13 DSM-5 somatic and cognitive symptoms: palpitations, sweating, trembling, shortness of breath, choking sensation, chest pain, nausea, dizziness, chills or hot flushes, paraesthesiae, derealisation/depersonalisation, fear of losing control, and fear of dying. Crucially, the attacks are 'unexpected' — they arise without an obvious trigger. After one or more attacks, the patient develops ≥1 month of anticipatory worry about future attacks or maladaptive behavioural change (agoraphobia — avoidance of situations where escape might be difficult).
Social Anxiety Disorder (Social Phobia) centres on intense fear of scrutiny or negative evaluation in social or performance situations — public speaking, meeting strangers, eating in public, using a telephone. Patients fear that they will embarrass or humiliate themselves, or that others will notice their anxiety. They avoid these situations or endure them with marked distress. This is distinct from ordinary shyness in its severity and functional impairment.
Specific Phobia involves intense, disproportionate fear of a circumscribed object or situation: needles, blood, heights, animals, flying, closed spaces. The patient recognises the fear as excessive but cannot control it. Exposure triggers immediate anxiety, often meeting criteria for a panic attack. The patient structures their life around avoidance.
| Disorder | Core feature | Trigger pattern | Duration criterion (DSM-5) |
|---|---|---|---|
| GAD | Pervasive worry, multiple domains | Continuous, non-specific | ≥6 months |
| Panic Disorder | Discrete panic attacks | Unexpected, any time | ≥1 month post-attack concern |
| Social Anxiety | Fear of scrutiny/embarrassment | Social/performance contexts | ≥6 months |
| Specific Phobia | Fear of specific object/situation | On exposure | ≥6 months |
SELF-CHECK
A 28-year-old woman describes sudden episodes of racing heart, shortness of breath, and fear of dying that last 10–15 minutes and occur without warning — while watching TV, during sleep, or waiting in a queue. Between episodes she is terrified of when the next one will happen. Which disorder best fits?
A. Generalised Anxiety Disorder
B. Panic Disorder with agoraphobia
C. Social Anxiety Disorder
D. Specific Phobia
Reveal Answer
Answer: B. Panic Disorder with agoraphobia
The key features are RECURRENT, UNEXPECTED panic attacks (discrete surges peaking within minutes, not a medical trigger) plus ≥1 month of anticipatory worry about future attacks — hallmarks of Panic Disorder (DSM-5). The episodes arising during sleep or while relaxed confirm they are not stimulus-bound (ruling out specific/social phobia). GAD features pervasive worry without discrete attacks.
Psychopathology and Aetiology of Anxiety Disorders
Anxiety disorders arise from a complex interplay of neurobiological vulnerability, learned fear responses, and psychosocial stressors. Understanding these mechanisms both deepens clinical insight and directly informs the rationale for specific treatments.
Provided image
The neurobiological model centres on the amygdala — the brain's threat-detection nucleus. In anxiety disorders, the amygdala is hyperresponsive: it triggers the hypothalamic-pituitary-adrenal (HPA) axis (releasing cortisol) and activates the sympathetic nervous system (releasing adrenaline and noradrenaline) in response to stimuli that objectively pose little or no threat. Three neurotransmitter systems are critically involved. GABA (gamma-aminobutyric acid), the principal inhibitory neurotransmitter, normally damps amygdala firing; reduced GABAergic activity leads to sustained fear responses — this is the pharmacological target of benzodiazepines. Serotonin (5-HT) modulates emotional tone through prefrontal cortical pathways; serotonin dysregulation accounts for both the mood and the anxiety components of GAD, and is the principal target of SSRIs. Noradrenaline, released from the locus coeruleus, mediates the physical arousal symptoms — palpitations, sweating, tremor — that dominate the presentation of panic attacks.
The fear-conditioning model (Pavlovian) explains panic disorder and specific phobias elegantly: an initial panic attack (unconditioned stimulus) becomes paired with a neutral context or internal cue (conditioned stimulus), such that the context alone subsequently triggers panic. This 'interoceptive conditioning' — where normal physiological sensations like a slight increase in heart rate become triggers — explains why attacks feel random to the patient but are actually conditioned responses.
The biopsychosocial risk factors include: genetic predisposition (heritability of GAD and panic disorder is 30–40%); temperament (behavioural inhibition in childhood — excessive shyness and fearfulness — strongly predicts adult anxiety disorders); adverse childhood experiences (abuse, neglect, parental loss); chronic life stress; and personality traits such as neuroticism and harm avoidance. Protective factors include secure attachment, social support, and high resilience.
Important: anxiety disorders rarely occur in isolation. GAD has a lifetime comorbidity with major depression exceeding 60%. Panic disorder commonly co-occurs with agoraphobia. Alcohol misuse may develop as a maladaptive coping mechanism, and its withdrawal exacerbates anxiety — creating a vicious cycle the primary care physician must identify and address.
Diagnosis and Distinguishing Anxiety from Medical Mimics
The single most important diagnostic discipline in primary care psychiatry is exclusion of medical causes before labelling anxiety as 'primary.' Several medical conditions produce symptoms virtually identical to anxiety disorders, and missing them causes serious harm to the patient — both by delaying appropriate medical treatment and by exposing them to unnecessary psychiatric stigma and inappropriate psychotropic medication. In clinical practice, the experienced primary care physician approaches every new anxiety presentation with two simultaneous tasks running in parallel: gathering the psychiatric symptom profile while simultaneously scanning for biological red flags that demand investigation first. The three commonest medical mimics — hyperthyroidism, cardiac arrhythmia, and phaeochromocytoma — each have distinguishing clinical features and targeted investigations. Hypoglycaemia is an additional mimic specific to diabetic patients on insulin or sulfonylureas. The mandatory baseline investigations for every new anxiety presentation are TSH, fasting blood glucose, and ECG; further investigations are ordered based on specific clinical indications.
Key medical mimics and their distinguishing investigations:
- Hyperthyroidism: palpitations, sweating, anxiety, tremor, weight loss, heat intolerance, diarrhoea; distinguish by TSH (suppressed in hyperthyroidism), free T4 (elevated). The patient may have a goitre. Unlike GAD, the worry content is not the predominant feature — the somatic symptoms dominate.
- Cardiac arrhythmia (supraventricular tachycardia, paroxysmal atrial fibrillation): episodic palpitations that may be indistinguishable from panic by symptoms alone. A 12-lead ECG during an episode, or a 24-hour Holter monitor, is required if the history suggests arrhythmia (abrupt onset, regular fast pulse, terminated by vagal manoeuvres).
- Phaeochromocytoma: episodic hypertension, headache, sweating, pallor, and palpitations — the classic 'surgical' mimic of panic disorder. Investigate with urine catecholamines/metanephrines when episodic hypertension accompanies the anxiety symptoms.
- Hypoglycaemia: in diabetic patients on insulin or sulfonylureas, hypoglycaemia causes sweating, tremor, palpitations, and anxiety. Check capillary blood glucose during symptoms.
DSM-5 diagnostic criteria (attribute system):
For GAD (DSM-5): excessive anxiety and worry about multiple events or activities, present on more days than not for ≥6 months (DSM-5 criterion; note that ICD-11 uses 'several months' without specifying a fixed six-month floor), which the patient finds difficult to control, with ≥3 associated symptoms (of 6: restlessness, fatigue, concentration difficulty, irritability, muscle tension, sleep disturbance). Causes clinically significant distress or functional impairment, not attributable to a substance or medical condition.
For Panic Disorder (DSM-5): recurrent unexpected panic attacks (≥4 of 13 specified symptoms, peaking within minutes), followed by ≥1 month of persistent concern about further attacks, their implications, or significant behavioural change.
For Social Anxiety Disorder (DSM-5): marked fear or anxiety about ≥1 social situation in which the person is exposed to possible scrutiny; fear out of proportion to actual threat; duration ≥6 months; causes significant distress or impairment.
Mental Status Examination (MSE) features in anxiety:
- Appearance: anxious facies, psychomotor restlessness or fidgeting; may be pale and sweating
- Speech: may be rapid, pressured, or halting
- Affect: anxious, apprehensive, tense
- Thought content: excessive worry (GAD), fear of dying or losing control (panic), fear of embarrassment (social anxiety)
- Perception: no hallucinations or illusions (hallucinations suggest psychosis or substance intoxication)
- Cognition: intact; concentration may be impaired due to worry
- Insight: usually preserved — patients recognise their fear is excessive, which distinguishes anxiety from delusional disorder
Mandatory baseline investigations in all new presentations: TSH, fasting blood glucose, ECG, FBC (anaemia can worsen anxiety). Reserve further investigations (echocardiogram, Holter, urine catecholamines) for specific clinical indications.
SELF-CHECK
A 42-year-old man presents with 8-month history of excessive worry about his business, health, and family — he finds the worry uncontrollable. He has muscle tension, poor sleep, difficulty concentrating, and fatigue. TSH and ECG are normal. By DSM-5, how long must symptoms have been present to diagnose GAD?
A. 2 weeks
B. 1 month
C. 3 months
D. 6 months
Reveal Answer
Answer: D. 6 months
DSM-5 GAD criterion A requires excessive anxiety and worry on more days than not for AT LEAST 6 MONTHS. Note: ICD-11 states 'several months' without specifying a fixed 6-month floor — always attribute the threshold to the classification system you are using. 2 weeks = MDE duration threshold; 1 month = panic disorder post-attack worry threshold.