Page 2 of 11
PS7.1 | Anxiety Disorders in Primary Care — SDL Guide (Part 2)
Management of Anxiety Disorders at Primary Care Level
The management of anxiety disorders at primary care level integrates psychoeducation, psychological interventions, and judicious pharmacotherapy — with the goal of reducing symptom burden, preventing chronicity, and restoring functional capacity. The WHO and NICE guidelines, and the NMC's expectation for PS7.1, specify that primary care physicians must be competent in initiating this management without defaulting immediately to specialist referral.
Step 1 — Psychoeducation: Begin by explaining the nature of anxiety to the patient — that it is a medical condition, not a character failing or 'going mad'; that it involves a sensitised nervous system and is highly treatable; that avoidance perpetuates the disorder (the 'safety behaviour' trap); and that recovery involves gradual engagement with feared situations, not permanent withdrawal.
Step 2 — Psychological treatments (first-line):
Cognitive-Behavioural Therapy (CBT) is the most evidence-based psychological treatment for all anxiety disorders. It targets two components: the cognitive distortions that maintain anxiety (catastrophic thinking, probability overestimation) and the behavioural avoidance that prevents natural extinction. For panic disorder, CBT includes interoceptive exposure — deliberately inducing mild physical sensations to extinguish the conditioned fear response. For specific phobia, graduated systematic desensitisation is the treatment of choice. At primary care level, brief CBT psychoeducation (2–4 sessions) or self-help bibliotherapy guided by the physician can be initiated before the patient reaches a psychologist.
Relaxation training — progressive muscle relaxation, controlled breathing (diaphragmatic breathing, paced breathing at 5–6 breaths/minute), and mindfulness-based stress reduction — are adjuncts that reduce physiological arousal and empower patients.
Step 3 — Pharmacological treatment:
SSRIs (Selective Serotonin Reuptake Inhibitors) are the first-line pharmacological treatment for all anxiety disorders including GAD, Panic Disorder, Social Anxiety Disorder, and OCD. Common agents: sertraline (50–200 mg/day), escitalopram (10–20 mg/day), fluoxetine (20–60 mg/day). An adequate SSRI trial requires 4–6 weeks at therapeutic dose before assessing response; partial responders may require 8–12 weeks. Inform patients that SSRIs may cause a transient worsening of anxiety in the first 1–2 weeks — warn them in advance to prevent premature discontinuation.
SNRIs (Serotonin-Noradrenaline Reuptake Inhibitors — venlafaxine, duloxetine) are effective second-line alternatives, particularly when depression co-exists with anxiety.
Benzodiazepines (diazepam, lorazepam, alprazolam) provide rapid anxiolytic effect within 30–60 minutes. However, they carry a significant risk of physical dependence with regular use extending beyond 2–4 weeks. Their role at primary care level is strictly limited to: (a) short-term bridging (≤2–4 weeks) while awaiting SSRI onset; (b) acute situational use (e.g. a single dose for a flight in a patient with specific phobia). Do NOT prescribe benzodiazepines as maintenance therapy for anxiety disorders. Withdrawal from long-term benzodiazepines itself resembles an anxiety disorder and may precipitate seizures — a serious iatrogenic harm.
Buspirone is a non-sedating, non-dependence-producing azapirone anxiolytic effective for GAD; onset is delayed 2–4 weeks. It has no role in acute anxiety or panic disorder.
Beta-blockers (propranolol) reduce peripheral adrenergic symptoms (palpitations, tremor) and may be used for situational performance anxiety (e.g. before a public presentation). They are not effective for the cognitive components of anxiety.
Stepped care and referral: Most patients with mild-to-moderate anxiety disorders can be managed entirely in primary care. Refer to secondary psychiatry services when: symptoms are severe and not responding to two adequate trials of pharmacotherapy; there is comorbid serious psychiatric disorder (psychosis, bipolar disorder, severe depression with suicidality); the patient has substance dependence requiring detoxification; or diagnostic uncertainty persists.
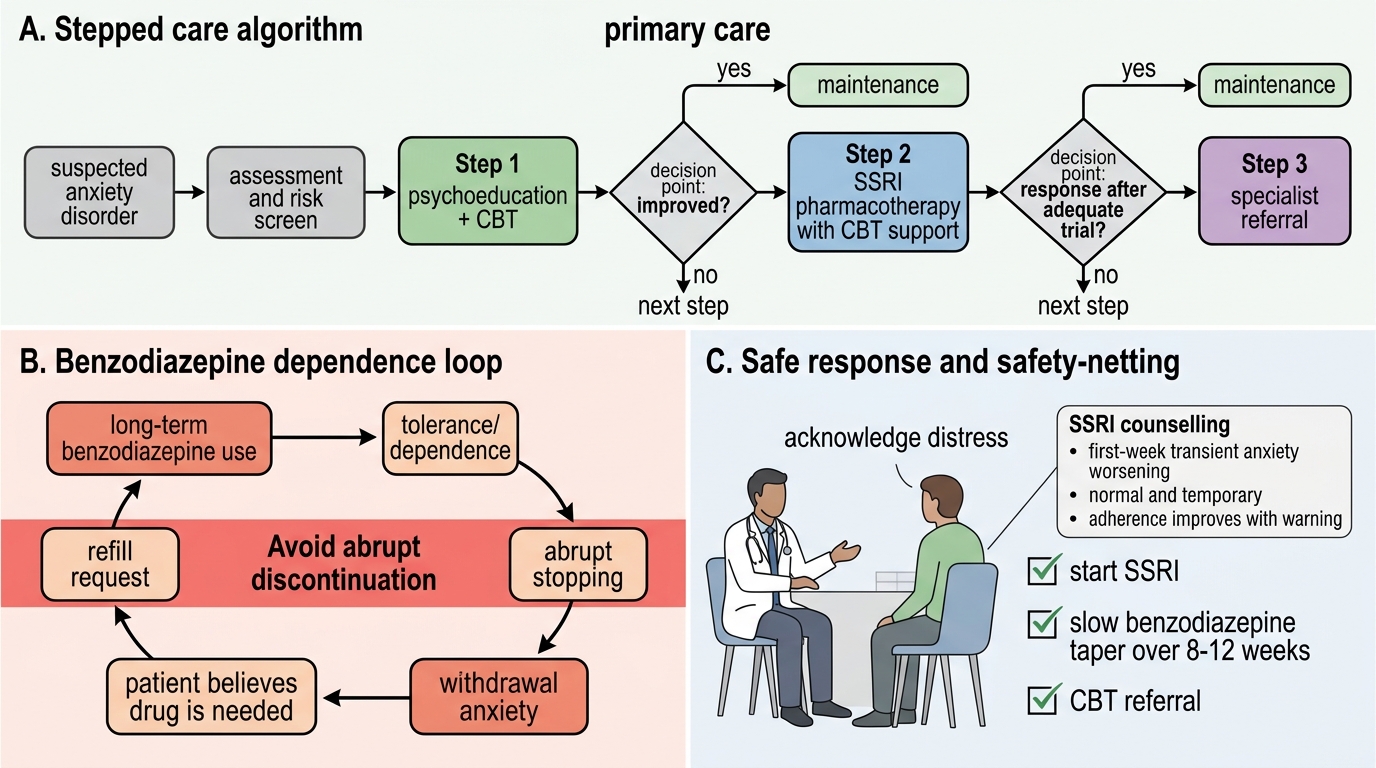
Stepped Care for Anxiety Disorders in Primary Care
CLINICAL PEARL
The benzodiazepine trap in primary care: When a patient requests a refill of 'nerve tablets' prescribed 18 months ago, resist the reflex to continue. Long-term benzodiazepine use (>4 weeks) causes pharmacological dependence — stopping abruptly causes a withdrawal syndrome identical to severe anxiety, reinforcing the false belief that the drug is still 'needed.' The appropriate response is: (1) acknowledge the patient's distress; (2) explain the dependence concept; (3) initiate an SSRI; (4) formulate a slow, structured benzodiazepine taper over 8–12 weeks; (5) provide a CBT referral. Never abruptly discontinue benzodiazepines in a dependent patient.
A second pearl: SSRIs transiently worsen anxiety in the first week. Warn patients explicitly before starting — many stop the medication in the first week believing it is 'making things worse.' A safety-netting conversation ('this is normal, temporary, and a sign the medication is working on your serotonin system') dramatically improves adherence and treatment outcomes.
Self-Assessment: Anxiety Disorders in Practice
You have now worked through the clinical presentation, psychopathology, diagnostic criteria, and management of anxiety disorders at primary care level. Self-assessment is not merely about recalling facts — it is an opportunity to apply your knowledge to clinical scenarios that mirror real internship decisions. Use these questions to test whether you can move from pattern recognition to a complete management plan. The self-assessment also prompts you to cross-check your knowledge of the diagnostic thresholds, the first-line pharmacotherapy hierarchy, and the limits of benzodiazepine prescribing.
Work through each scenario below before looking at the explanations. For each case, identify: (a) the most likely anxiety disorder and classification system applied; (b) the necessary investigations to exclude medical mimics; (c) your first-line treatment choice; and (d) any referral considerations.
Scenario A: A 19-year-old college student avoids all oral presentations, skips group seminars, and is failing her course. She is terrified that she will 'go blank' and be humiliated in front of peers. She has no panic attacks outside social situations, and her baseline anxiety between social encounters is low. What is the diagnosis?
Answer: Social Anxiety Disorder (DSM-5) — fear is specifically tied to social/performance situations with fear of negative evaluation, duration exceeding 6 months, causing significant functional impairment (academic failure). Note that the 6-month duration criterion is from DSM-5; ICD-11 also uses 6 months for social anxiety. First-line: CBT (graduated exposure to social situations) + sertraline if psychological treatment alone is insufficient.
Scenario B: A 52-year-old civil servant presents with 12 months of constant excessive worry about retirement finances, his wife's health, and minor health complaints. He reports neck pain (muscle tension), waking at 3 AM, fatigue, and difficulty making decisions. TSH is normal. He denies discrete panic attacks.
Answer: Generalised Anxiety Disorder (DSM-5: ≥6 months of excessive, uncontrollable worry in multiple domains + ≥3 associated symptoms). Investigations: TSH (done, normal), FBC, fasting glucose, ECG. Treatment: sertraline 50 mg once daily (titrate to 100–150 mg as needed over 4 weeks), psychoeducation, progressive muscle relaxation instruction, and a referral letter for CBT within the district psychiatry outreach service.
Scenario C: A 38-year-old nurse asks you to prescribe diazepam 10 mg daily 'for her nerves,' stating she has been on it for 2 years and cannot function without it. She is anxious but has no current psychiatric comorbidity.
Answer: Likely benzodiazepine dependence superimposed on the original anxiety disorder. Do NOT prescribe further diazepam. Plan: (1) acknowledge distress; (2) explain dependence; (3) start escitalopram 10 mg; (4) structured taper diazepam over 8–12 weeks (reduce by 10% of current dose per 1–2 weeks); (5) refer to CBT; (6) follow-up weekly during the taper. She requires primary care management, not necessarily immediate psychiatric referral unless taper fails or suicidality emerges.
SELF-CHECK
You prescribe sertraline 50 mg/day for GAD. The patient calls you 5 days later reporting 'feeling more jittery and nervous.' What is the most appropriate response?
A. Stop sertraline immediately — it is causing worsening anxiety
B. Switch to a benzodiazepine instead
C. Reassure that a transient worsening in the first 1-2 weeks is expected and ask her to continue
D. Reduce dose to 25 mg and re-assess in 4 weeks
Reveal Answer
Answer: C. Reassure that a transient worsening in the first 1-2 weeks is expected and ask her to continue
SSRIs commonly cause a transient increase in anxiety symptoms in the first 1–2 weeks of treatment due to initial serotonergic activation before autoreceptor downregulation produces anxiolysis. This is expected, temporary, and does not indicate treatment failure. Patients who are not warned in advance frequently stop the medication prematurely. Benzodiazepines should not be substituted (dependence risk). Stopping abruptly is incorrect. A dose reduction to 25mg is sometimes used for very sensitive patients but reassurance and continuation is the primary response.