Page 1 of 11
PS10.1 | Childhood Neurodevelopmental Psychiatry — SDL Guide
Learning Objectives
- Classify neurodevelopmental disorders of childhood and adolescence using ICD-11 and DSM-5 frameworks
- Describe the core clinical features, onset criteria, and diagnostic requirements of ADHD
- Describe the core clinical features, diagnostic criteria, and severity spectrum of Autism Spectrum Disorder
- Differentiate ADHD from ASD and from Intellectual Disability Disorder
- Outline evidence-based management strategies for ADHD and ASD including pharmacological and non-pharmacological approaches
INSTRUCTIONS
Neurodevelopmental disorders are among the most common psychiatric conditions presenting in childhood and adolescence. Understanding their clinical features, diagnostic criteria, and management is essential for every clinician, since these conditions affect learning, social development, and daily functioning. Unrecognised or misdiagnosed ADHD and ASD carry significant consequences for the child's educational trajectory, mental health, and family wellbeing.
References
- Ahuja N. A Short Textbook of Psychiatry, 8th ed. Jaypee Brothers, New Delhi. Chapter 16: Child and Adolescent Psychiatry (textbook)
- Kaplan HI, Sadock BJ. Synopsis of Psychiatry, 11th ed. Wolters Kluwer. Chapter 31: Neurodevelopmental Disorders (textbook)
- ICD-11 Classification of Mental and Behavioural Disorders. WHO, Geneva, 2022. Section 06: Neurodevelopmental Disorders (guideline)
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5). APA, 2013. Chapter: Neurodevelopmental Disorders (guideline)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A mother brings her 8-year-old son to the paediatric outpatient clinic because his class teacher has complained that he cannot sit still, frequently interrupts, and has not completed a single homework assignment this term. At home, he starts tasks but never finishes them, loses his school bag almost every week, and seems to be 'in his own world' during conversations. His mother assumed he was simply naughty, but a different child in the same class — a quiet girl who never makes eye contact, has an unusual passion for train timetables, and becomes distressed when the classroom routine changes — has just been told she may have autism. Both families are asking the same question: is this a behavioural problem, or something neurological? As a future clinician, you need the knowledge to answer that question accurately — and the two conditions, while they share a neurodevelopmental origin, are fundamentally distinct in their core features, diagnostic criteria, and management.
WHY THIS MATTERS
ADHD and Autism Spectrum Disorder together affect an estimated 5–10% of school-age children worldwide, making them the most prevalent neurodevelopmental conditions you will encounter in general practice, paediatrics, and psychiatry. Both conditions are chronically underdiagnosed, particularly in girls and in resource-limited settings. Misidentification leads to years of unnecessary academic failure, social exclusion, and mental health co-morbidity. The Indian context adds complexity: cultural norms around children's behaviour, stigma attached to psychiatric labels, and limited access to specialist services mean that primary care physicians must be the first line of clinical reasoning. Being able to classify these disorders, apply the correct diagnostic criteria, and initiate or recommend appropriate management is therefore a core competency for every NMC-trained doctor.
RECALL
Before proceeding, recall what you know about normal neurodevelopment. Typically developing children achieve language milestones (first words ~12 months, two-word phrases ~18-24 months, sentences ~3 years), social milestones (joint attention by 9-12 months, symbolic play by 18-24 months), and motor milestones across the first 5 years of life. Any significant delay in one or more domains raises a developmental concern. You should also recall from your Year-1 Physiology the role of the prefrontal cortex in executive function — working memory, inhibitory control, and cognitive flexibility — since these are precisely the functions disrupted in ADHD.
Developmental and Clinical Presentation of ADHD and ASD
Neurodevelopmental disorders are conditions that arise during the developmental period (usually before school age, though diagnosis may occur later) and are characterised by developmental deficits that produce impairments in personal, social, academic, or occupational functioning. Both ICD-11 and DSM-5 group these conditions together, recognising their shared aetiology in altered brain maturation rather than acquired pathology.
Provided image
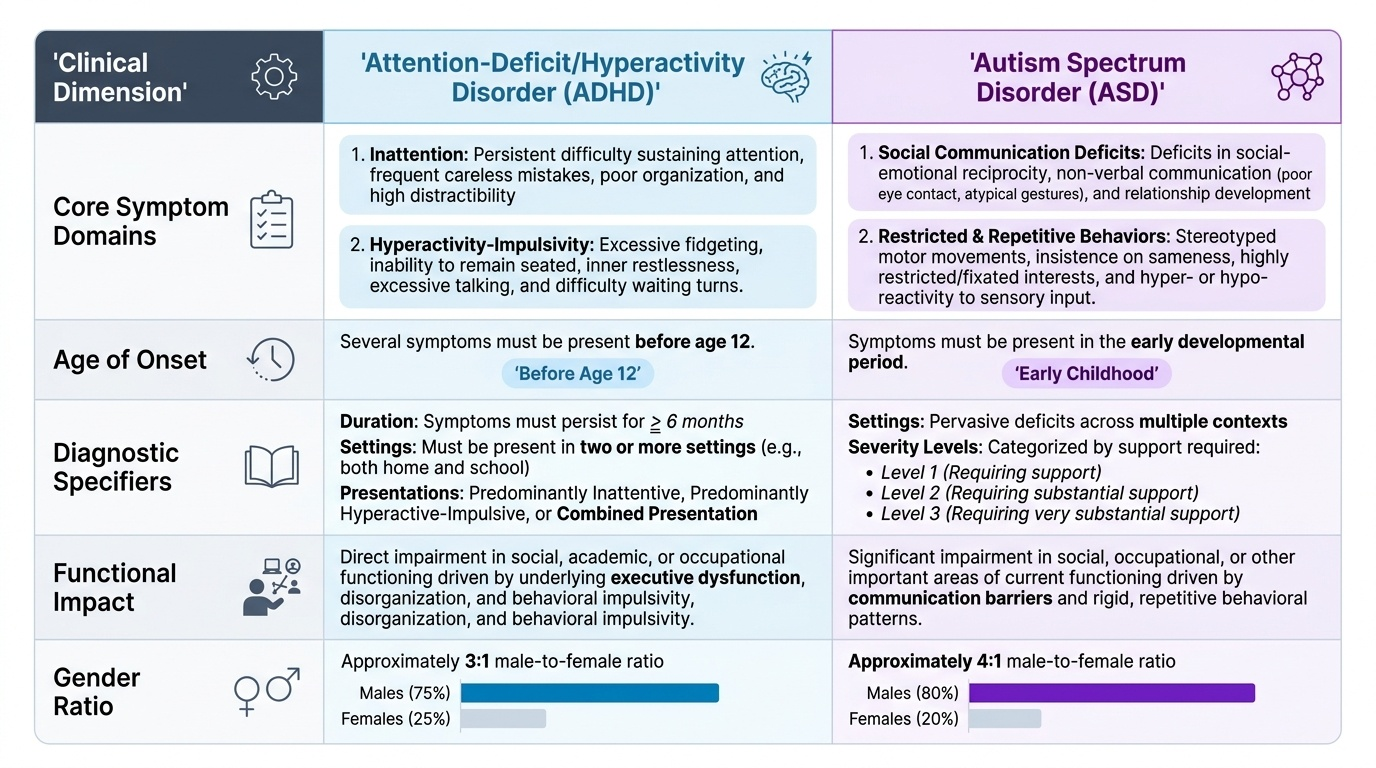
Attention-Deficit/Hyperactivity Disorder (ADHD) presents with two core symptom domains. The first domain is inattention — difficulty sustaining attention on tasks or play activities, frequent careless mistakes in schoolwork, apparent failure to listen when spoken to directly, difficulty organising tasks and activities, frequent loss of items needed for tasks, and easy distraction by extraneous stimuli. The second domain is hyperactivity-impulsivity — often fidgeting or squirming, leaving seat in situations where remaining seated is expected, excessive running or climbing in inappropriate situations (in adolescents/adults, often a subjective feeling of restlessness), talking excessively, blurting out answers before a question is completed, and difficulty waiting for a turn. These symptoms must be present in two or more settings (e.g., both home and school) and must cause functional impairment in social, academic, or occupational domains.
DSM-5 recognises three presentations: (1) predominantly inattentive, (2) predominantly hyperactive-impulsive, and (3) combined presentation. ICD-11 uses analogous specifiers. The developmental onset criterion in DSM-5 requires that several inattentive or hyperactive-impulsive symptoms were present before age 12 — a deliberate relaxation from the DSM-IV requirement of onset before age 7, reflecting evidence that parental recall of exact symptom onset is unreliable. The symptom duration must be at least 6 months.
Autism Spectrum Disorder (ASD) presents with two core feature domains. The first is persistent deficits in social communication and social interaction across multiple contexts — including deficits in social-emotional reciprocity (reduced back-and-forth conversation, difficulty sharing interests), non-verbal communicative behaviours (poor eye contact, atypical gestures or facial expression, limited use of pointing), and developing, maintaining, and understanding relationships (difficulty adjusting behaviour to social contexts, absent imaginative play, lack of interest in peers). The second domain is restricted, repetitive patterns of behaviour, interests, or activities — stereotyped or repetitive motor movements or speech (echolalia, idiosyncratic phrases), insistence on sameness and inflexible adherence to routines, highly restricted and fixated interests that are abnormal in intensity or focus, and hyper- or hypo-reactivity to sensory input.
In ASD, symptoms must be present in the early developmental period (though they may not fully manifest until social demands exceed capacity), must cause clinically significant impairment, and must not be better explained by intellectual disability or global developmental delay alone. ASD represents a spectrum of severity — ICD-11 specifies severity based on the degree of support needed (Level 1: requires support; Level 2: requires substantial support; Level 3: requires very substantial support).
IMPORTANT clinical note: ADHD and ASD can and do co-occur. DSM-5 explicitly permits dual diagnosis, a change from DSM-IV which excluded ADHD when ASD was present. Co-occurring ADHD in a child with ASD is common (estimated 30–80% prevalence) and significantly worsens functional outcomes.
SELF-CHECK
A 9-year-old boy is referred because of poor school performance and disruptive classroom behaviour. His teacher reports he talks out of turn, cannot wait his turn in games, and walks around the classroom. At home, his parents note he loses his school bag frequently and cannot finish homework. Symptoms have been present since age 5. According to DSM-5, what is the minimum number of settings in which these symptoms must cause impairment for a diagnosis of ADHD?
A. 1 setting (school alone is sufficient)
B. 2 or more settings
C. 3 or more settings
D. The child must be observed directly in a clinic setting
Reveal Answer
Answer: B. 2 or more settings
DSM-5 requires that several symptoms of inattention or hyperactivity-impulsivity are present in two or more settings (e.g., home AND school) and cause functional impairment. This multi-setting criterion ensures the symptoms are pervasive and not situational. The diagnostician does not need to directly observe the child in clinic — informant reports from parents and teachers, supplemented by rating scales, are the standard evidence base.
Psychopathology and Aetiology
Understanding the neurobiological and aetiological underpinnings of ADHD and ASD helps clinicians counsel families, set realistic expectations, and avoid blaming parenting style for what are fundamentally neurodevelopmental conditions.
Neurobiological basis of ADHD. The core dysfunction in ADHD lies in the prefrontal-striatal-cerebellar networks that regulate executive function. Neuroimaging studies demonstrate reduced volume and delayed cortical maturation in the prefrontal cortex, caudate nucleus, and cerebellum in children with ADHD compared to age-matched controls. The neurotransmitter systems primarily implicated are dopamine (especially in the mesocortical and nigrostriatal pathways) and norepinephrine (in the prefrontal cortex). Reduced dopaminergic and noradrenergic tone in the prefrontal cortex impairs inhibitory control, working memory, and sustained attention — the three core executive function deficits in ADHD. This neurotransmitter model directly explains the mechanism of action of effective pharmacotherapy: stimulant medications such as methylphenidate block the reuptake of dopamine and norepinephrine, acutely restoring prefrontal function.
Aetiology of ADHD. ADHD has a strong genetic component — heritability estimates from twin studies range from 70–80%, among the highest of any psychiatric condition. First-degree relatives of children with ADHD have a 5–10-fold increased risk. Multiple common genetic variants of small effect size have been identified (genome-wide association studies), involving genes in dopaminergic and noradrenergic pathways (e.g., DRD4, DAT1/SLC6A3). Environmental risk factors are additive and include low birth weight, prematurity, prenatal exposure to tobacco or alcohol, and perinatal hypoxia. Despite popular belief, refined sugar, food additives, and poor parenting do not cause ADHD, though certain dietary factors may exacerbate symptoms in some individuals.
Neurobiological basis of ASD. The social brain network — encompassing the superior temporal sulcus, amygdala, fusiform gyrus, and medial prefrontal cortex — shows atypical activation and connectivity in ASD. The amygdala, which processes social-emotional signals, is often over-reactive to faces and social stimuli, contributing to social anxiety and gaze avoidance. Reduced connectivity between frontal-temporal regions underlies impaired theory of mind (the ability to understand that others have different mental states, beliefs, and intentions — sometimes called 'mentalising'). Neuroimaging consistently shows altered long-range connectivity (reduced) and local connectivity (sometimes increased), consistent with theories of altered cortical organisation.
Aetiology of ASD. ASD is highly heritable (concordance ~70–90% in monozygotic twins). The genetic architecture is complex: hundreds of rare single-gene mutations and copy number variants (e.g., 16p11.2 deletion, SHANK3, NRXN1, MECP2) each account for a small proportion of cases, while common variants collectively contribute to population-level risk. Monogenic causes include Fragile X syndrome (ASD in ~30% of affected males), Tuberous Sclerosis, and MECP2 mutations (Rett syndrome, an X-linked condition almost exclusively in females). Environmental risk factors include advanced parental age and prenatal exposure to valproate. The debunked 1998 MMR–ASD hypothesis was based on fraudulent data — there is no causal link between vaccines and autism.
Diagnostic Assessment — Criteria, Developmental History, and Standardised Tools
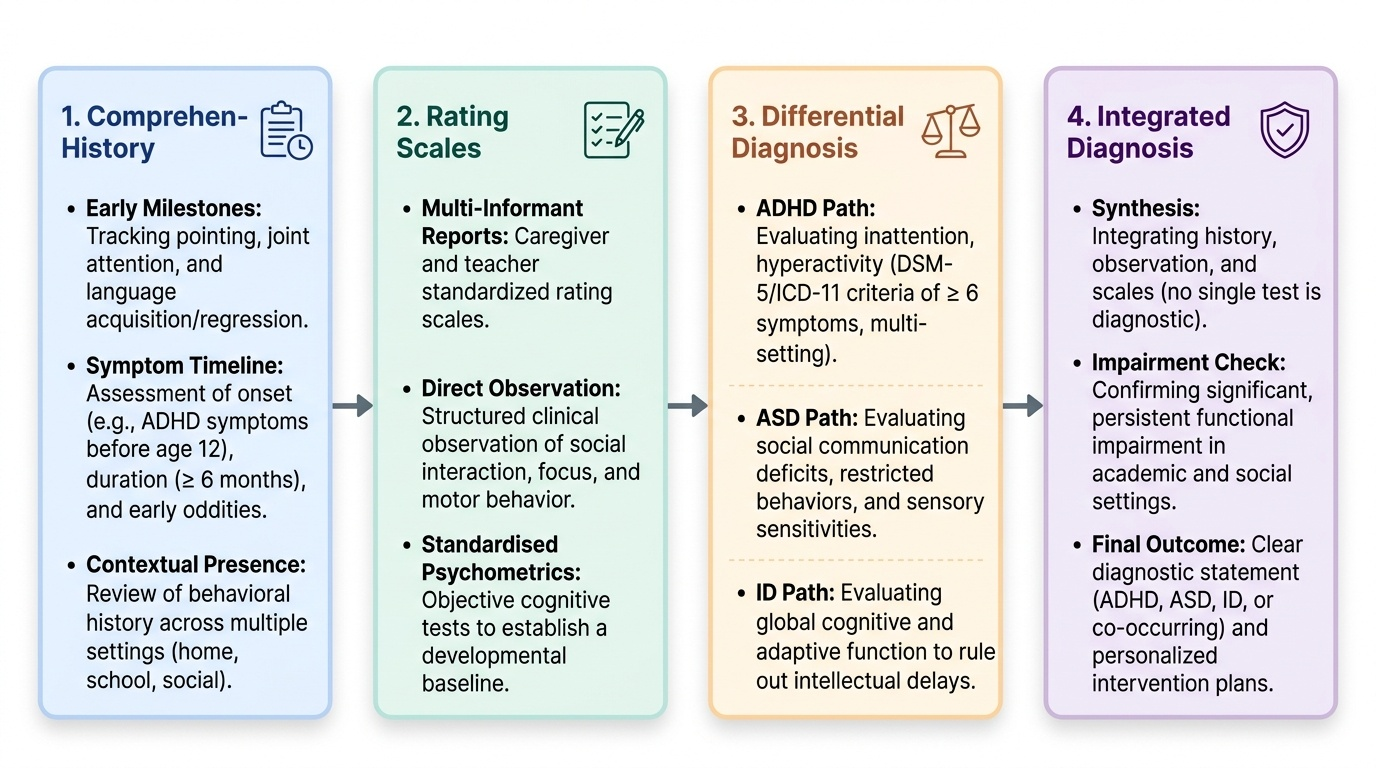
Diagnosis of both ADHD and ASD rests on a multi-informant, multi-method assessment — there is no blood test, brain scan, or single rating scale that establishes either diagnosis. The diagnostic process integrates a detailed developmental history, direct clinical observation, caregiver and teacher report, and standardised psychometric instruments.
Provided image
Developmental history is the cornerstone of assessment. For ADHD, the clinician seeks a history of symptom onset (several symptoms before age 12 in DSM-5), duration (≥6 months), multi-setting presence, and functional impairment in school performance and peer relationships. For ASD, the history focuses on the child's early social milestones — did the child point to share interest (protodeclarative pointing) by 12 months? Did joint attention emerge? Was there loss of previously acquired language or social skills? Were there sensory sensitivities or restricted interests from infancy? Parents often recall early oddities in retrospect once the diagnosis is framed.
ICD-11 diagnostic criteria for ADHD (6A05): a persistent pattern of inattention and/or hyperactivity-impulsivity that is more frequent/severe than typically observed in individuals at a comparable level of development, is not better accounted for by another condition, and that directly impacts adversely on academic/occupational or social functioning. ICD-11 requires impairment across multiple settings.
DSM-5 diagnostic criteria for ADHD: ≥6 symptoms of inattention OR ≥6 symptoms of hyperactivity-impulsivity (≥5 each for adolescents ≥17 years), present for ≥6 months, several symptoms present before age 12, present in ≥2 settings, clear impairment, and not better explained by another mental disorder.
ICD-11 for ASD (6A02): persistent deficits in social communication and social interaction, plus restricted/repetitive behaviours, interests, or activities; onset during developmental period; causing significant impairment.
DSM-5 for ASD: (A) persistent deficits in social communication/interaction across multiple contexts in all 3 sub-domains; (B) ≥2 of 4 types of restricted/repetitive behaviours; (C) symptoms present in early developmental period; (D) significant functional impairment; (E) not better explained by ID alone.
Standardised assessment tools: For ADHD — the Conners' Rating Scales (parent and teacher versions) and the Vanderbilt ADHD Diagnostic Rating Scales quantify symptom frequency and severity. For ASD — the Autism Diagnostic Observation Schedule, 2nd edition (ADOS-2) is the observational gold standard, assessing social communication, play, and restricted/repetitive behaviour through structured play-based interaction; the Autism Diagnostic Interview – Revised (ADI-R) is the parent interview gold standard. The Childhood Autism Rating Scale (CARS) is widely used in India as a screening and severity measure.
Differential diagnosis is a common clinical challenge. The following framework guides differentiation:
IMPORTANT: ADHD inattention can mimic ASD's social withdrawal — the key distinction is that in ADHD social skills are present but inconsistently applied (the child knows how to interact but is too impulsive or distractible), whereas in ASD social communication deficits are intrinsic and pervasive regardless of arousal level.
Intellectual Disability Disorder (ID) must also be considered: a child with moderate ID may appear hyperactive and have limited social communication, but the distinguishing feature is a global deficit in intellectual functioning (IQ ≤70) alongside adaptive functioning deficits — whereas in ADHD and ASD, intellectual ability may be average or above average. ASD and ADHD can co-occur with ID, in which case all three diagnoses may be warranted.
| Feature | ADHD | ASD | ID |
|---|---|---|---|
| Core domain | Attention/executive function | Social communication + RRBs | Intellectual + adaptive function |
| Social skills | Present but inconsistent | Intrinsically impaired | Globally reduced |
| Language | Usually intact | Often atypical; may be absent | Delayed, concurrent with cognition |
| Onset criterion | Symptoms before age 12 | Early developmental period | During developmental period |
| IQ | Usually average or above | Ranges from gifted to severe ID | Definitionally below average |
SELF-CHECK
A 5-year-old girl shows no eye contact, does not respond to her name, has no functional language, and spends hours arranging toy cars in lines by colour. Which of the following additional findings would most support a diagnosis of Autism Spectrum Disorder rather than Intellectual Disability alone?
A. A global IQ of 55 on psychometric testing
B. Deficit specifically in social-emotional reciprocity and restricted repetitive behaviour with IQ of 80
C. Delayed achievement of all developmental milestones by 18 months
D. Normal adaptive functioning on the Vineland Adaptive Behavior Scales
Reveal Answer
Answer: B. Deficit specifically in social-emotional reciprocity and restricted repetitive behaviour with IQ of 80
ASD is characterised by domain-specific deficits in social communication and restricted/repetitive behaviours, and can occur at any intellectual level including average or above-average IQ. A child with an IQ of 80 (above the ID threshold of approximately 70) who shows the core ASD features points strongly to ASD rather than ID alone. A global IQ of 55 with associated adaptive deficits would suggest ID (which may also co-occur with ASD). Delayed milestones and normal Vineland scores are non-specific or inconsistent with ID, respectively.