Page 2 of 11
PS10.1 | Childhood Neurodevelopmental Psychiatry — SDL Guide (Part 2)
Management of ADHD and ASD
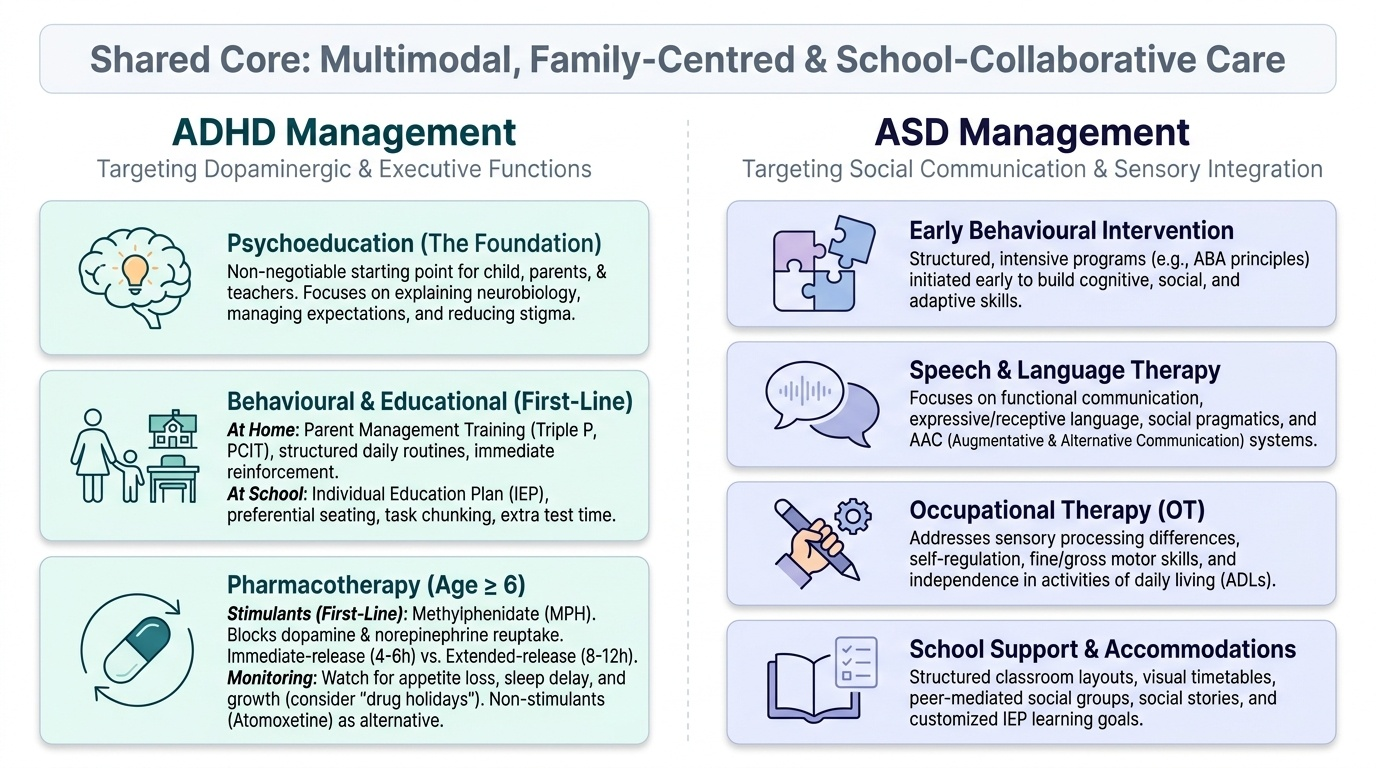
Management of ADHD and ASD is multimodal — no single intervention suffices for either condition. The approach combines psychoeducation, evidence-based behavioural and educational interventions, and (for ADHD) pharmacotherapy when indicated. Family-centred care and school collaboration are integral to success in both conditions.
Provided image
Management of ADHD
The foundation of ADHD management is psychoeducation for the child, parents, and teachers — explaining the neurobiological nature of ADHD, setting appropriate expectations, reducing stigma, and establishing a collaborative team around the child. This step is non-negotiable and must precede or accompany all other interventions.
Behavioural and educational interventions are first-line for preschool-aged children (under 6) and remain essential throughout. Behaviour therapy principles — immediate reinforcement, consistent routines, clear and simple instructions, task chunking — improve functioning at home and school. Parent management training programmes (e.g., Triple P, PCIT) equip caregivers with structured strategies. School-based accommodations — extended time for tests, preferential seating near the teacher, reduced homework volume, written rather than oral instructions — are evidence-based and can be formalised as an Individual Education Plan (IEP).
Pharmacotherapy is recommended when behavioural interventions alone are insufficient, particularly for school-age children (age ≥6) with moderate-to-severe functional impairment. Stimulants are first-line pharmacotherapy. Methylphenidate (MPH) is the most widely used and studied stimulant: it blocks the reuptake of dopamine and norepinephrine in the synapse, increasing prefrontal cortical tone and improving attention and impulse control. It is available as immediate-release (duration 4–6 hours) and extended-release (8–12 hours) formulations. Common adverse effects include reduced appetite, delayed sleep onset, and headache — all dose-dependent and often manageable. Growth monitoring is recommended with long-term use; medication breaks ('drug holidays') during school vacations may allow catch-up growth. Amphetamine-based stimulants (dexamphetamine) are an alternative where available. Non-stimulant alternatives include atomoxetine (a selective norepinephrine reuptake inhibitor — second-line; useful when stimulants are contraindicated or abused, or in co-occurring anxiety), and clonidine/guanfacine (alpha-2 agonists — useful adjuncts for hyperactivity, tics, or insomnia).
IMPORTANT: There is no curative drug for ADHD — medication manages symptoms while it is being taken and does not alter the underlying neurological trajectory. Medication in combination with behavioural therapy produces better outcomes than either alone (as established by the Multimodal Treatment of ADHD study).
Management of ASD
There is no pharmacological cure for ASD — the core social communication deficits and restricted/repetitive behaviours are not ameliorated by any currently approved drug. Management focuses on maximising functional skills, reducing distress, and supporting the family.
Early intensive behavioural intervention (EIBI) is the most evidence-supported treatment for ASD, particularly when started before age 5. Applied Behaviour Analysis (ABA)-based programmes provide structured, intensive therapy (20–40 hours/week) targeting communication, social skills, play, and adaptive behaviours. The EIBI evidence base for improving language and adaptive outcomes in young children is strong.
Speech and language therapy is essential for all children with ASD who have communication difficulties — targeting functional communication, pragmatics (the social use of language), and, where verbal communication is absent, augmentative and alternative communication (AAC) devices. Occupational therapy addresses sensory processing difficulties and fine motor skills. Social skills groups benefit higher-functioning older children and adolescents.
Pharmacotherapy in ASD addresses co-morbid symptoms rather than core ASD features. Risperidone and aripiprazole (atypical antipsychotics) are approved for irritability and aggression associated with ASD. SSRIs may be used for co-occurring anxiety or obsessive-compulsive behaviours. Melatonin is effective for sleep disturbance. If ADHD co-occurs, methylphenidate may be used, though response rates are lower and side effects more frequent than in ADHD without ASD.
Family support is a cornerstone of ASD management. Parent-mediated intervention programmes (e.g., PECS — Picture Exchange Communication System; ESDM — Early Start Denver Model) empower parents to implement intervention techniques in the home environment. Genetic counselling is offered when a specific genetic cause is identified, given recurrence risks within families.
SELF-CHECK
A 7-year-old boy with a confirmed diagnosis of ADHD (combined presentation) and moderate functional impairment despite 6 months of behaviour therapy is being considered for pharmacotherapy. Which of the following is the correct first-line pharmacological option according to evidence-based guidelines?
A. Atomoxetine (non-stimulant SNRI)
B. Risperidone (atypical antipsychotic)
C. Methylphenidate (stimulant)
D. Fluoxetine (SSRI)
Reveal Answer
Answer: C. Methylphenidate (stimulant)
Methylphenidate, a CNS stimulant that blocks reuptake of dopamine and norepinephrine, is the first-line pharmacotherapy for ADHD in school-age children when behavioural interventions alone are insufficient. Atomoxetine is a second-line non-stimulant option, used when stimulants are contraindicated, ineffective, or when co-occurring anxiety makes stimulants less suitable. Risperidone is used for irritability in ASD, not ADHD. Fluoxetine has no primary role in uncomplicated ADHD.
Self-Assessment — Integrating Knowledge of ADHD and ASD
This self-assessment section invites you to consolidate your understanding of childhood neurodevelopmental psychiatry by working through the key concepts covered in this module. Read each paragraph reflectively and test your recall before moving to the summary.
Classification framework. Both ADHD and Autism Spectrum Disorder are classified under the neurodevelopmental disorders grouping in ICD-11 (Section 06) and DSM-5. This grouping reflects their shared origin in altered brain maturation during the developmental period — they are not acquired psychiatric conditions but rather differences in how the brain develops. ICD-11 and DSM-5 criteria overlap substantially but differ in some threshold specifics — a clinician should state which system they are applying when recording a diagnosis.
Core diagnostic distinction. The defining features of ADHD are inattention and/or hyperactivity-impulsivity that are developmentally inappropriate, cross-situational (two or more settings), and functionally impairing. The defining features of ASD are persistent deficits in social communication and social interaction, combined with restricted, repetitive patterns of behaviour, interests, or activities. These are fundamentally different phenotypes — a child with ADHD typically has intact social communication (though impulse control may disrupt interactions), while a child with ASD has intrinsic deficits in social reciprocity and communication regardless of attentional state. Both conditions can co-occur, and both can co-occur with Intellectual Disability Disorder.
Onset criteria. For ADHD (DSM-5), several symptoms must have been present before age 12 — not necessarily causing full clinical impairment at that point, but present. For ASD, symptoms must be present in the early developmental period, though they may not fully manifest until social demands increase (often around school entry). For Intellectual Disability Disorder, onset must be during the developmental period.
First-line management. For ADHD, the first-line approach combines psychoeducation (for child, parents, and teachers), behaviour therapy and school accommodations, and — for school-age children with moderate-to-severe impairment — stimulant pharmacotherapy with methylphenidate as the evidence-based first-line drug. For ASD, the cornerstone is early intensive behavioural intervention (ideally before age 5), supported by speech and language therapy, occupational therapy, and family-mediated intervention — there is no curative drug for the core features of ASD. Pharmacotherapy in ASD targets co-morbid symptoms only.
Diagnostic tools. Rating scales (Conners', Vanderbilt) quantify ADHD symptoms in a multi-informant format. For ASD, the ADOS-2 (observational gold standard) and the CARS (widely used in India) are the primary instruments. Diagnosis requires integration of history, observation, and multiple informant reports — never a single test result.
Test yourself: Can you explain to a parent why their child's ADHD diagnosis does not mean the child is 'bad' or the parents have failed? Can you distinguish the social difficulties seen in ADHD from those in ASD in a clinical scenario? Can you name the first-line drug for ADHD and explain why it works? Can you explain why there is no pharmacological cure for ASD but why early intervention matters?
CLINICAL PEARL
The most common clinical mistake is to diagnose ADHD and ASD as mutually exclusive. Under DSM-IV, a diagnosis of ASD precluded an ADHD diagnosis. DSM-5 removed this exclusion — dual diagnosis is not only permitted but expected in a significant proportion of children with ASD (estimated 30–80% have co-occurring ADHD). Missing the ADHD component in a child with ASD leads to under-treatment of a highly manageable condition. Similarly, a child labelled with ADHD who shows social communication deficits, sensory sensitivities, and rigid routines deserves a structured ASD evaluation — the two diagnoses are not competing labels but co-occurring conditions that compound functional impairment.