Page 1 of 8
PS13.1 | Modified ECT Principles — SDL Guide
Learning Objectives
- Describe the process of modified electroconvulsive therapy (ECT) step-by-step, including anaesthetic preparation, electrode placement, seizure induction, and recovery.
- Identify why the 'modified' technique (general anaesthesia + muscle relaxant) is safer than unmodified ECT and prevents musculoskeletal complications.
- State the clinical indications for ECT, including conditions where rapid response is essential.
- Recognise and dispel the common misconceptions associated with ECT, including fears about pain, memory loss, and misuse.
- Describe the safeguards under the Mental Healthcare Act 2017 that govern the use of ECT in India.
INSTRUCTIONS
Electroconvulsive therapy is one of the most effective and evidence-based treatments in psychiatry, yet it remains among the most misunderstood. As a future clinician, your ability to counsel patients and their families confidently — and to counter misinformation — depends on understanding what modified ECT actually involves. This module walks you through the procedure from the moment of referral to post-treatment monitoring, while equipping you to address the misconceptions you will encounter in clinical practice.
References
- Ahuja N. A Short Textbook of Psychiatry, 8th ed. Jaypee Brothers, 2019. Ch 20 — Biological Therapies. (textbook)
- Sadock BJ, Sadock VA, Ruiz P. Kaplan and Sadock's Synopsis of Psychiatry, 11th ed. LWW, 2015. Ch 36 — Biological Therapies. (textbook)
- Mental Healthcare Act 2017, Government of India. Sections 94–95 (ECT regulations). (guideline)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
Picture this: a 35-year-old woman with severe depression has not eaten or spoken in four days. She is at imminent risk of death from self-neglect. Her family asks, 'Doctor, is there any treatment that can help her right now?' Antidepressants require weeks to work. The answer is yes — electroconvulsive therapy, given safely under general anaesthesia, can induce remission in days. Yet when you explain this, her brother objects: 'ECT? That's electric shock torture — she'll lose her mind!' Your task as a clinician is to simultaneously save the patient and educate the family. This module gives you the knowledge to do both.
WHY THIS MATTERS
Modified ECT is a life-saving procedure that every psychiatry-trained clinician must understand. You will encounter patients for whom ECT is the most appropriate — sometimes the only — treatment option: in severe depression with suicidal risk, catatonia that is not responding to benzodiazepines, or treatment-resistant psychosis. Beyond identifying these patients, you are legally and ethically required to obtain informed consent, explain risks accurately, and address misconceptions. The Mental Healthcare Act 2017 imposes specific legal obligations on the treating clinician. Factual knowledge of the procedure, its safety profile, and its statutory framework is non-negotiable for competent psychiatric practice.
RECALL
Before proceeding, bring to mind what you know about the following:
- Grand-mal seizure physiology: a generalised tonic-clonic seizure involves synchronous electrical discharge across the brain, tonic muscular rigidity followed by clonic jerks, and post-ictal suppression.
- General anaesthesia basics (from your pharmacology year): induction agents (e.g. thiopentone, propofol), depolarising muscle relaxants (suxamethonium/succinylcholine), airway management, and monitoring under anaesthesia.
- Psychiatric emergencies: you have covered severe depressive disorder, catatonia, and neuroleptic malignant syndrome — ECT is relevant to all three.
If any of these are hazy, a quick review of the relevant pharmacology or physiology section before this module will make the mechanism discussion clearer.
Orientation: What Is ECT and Why Does It Exist?
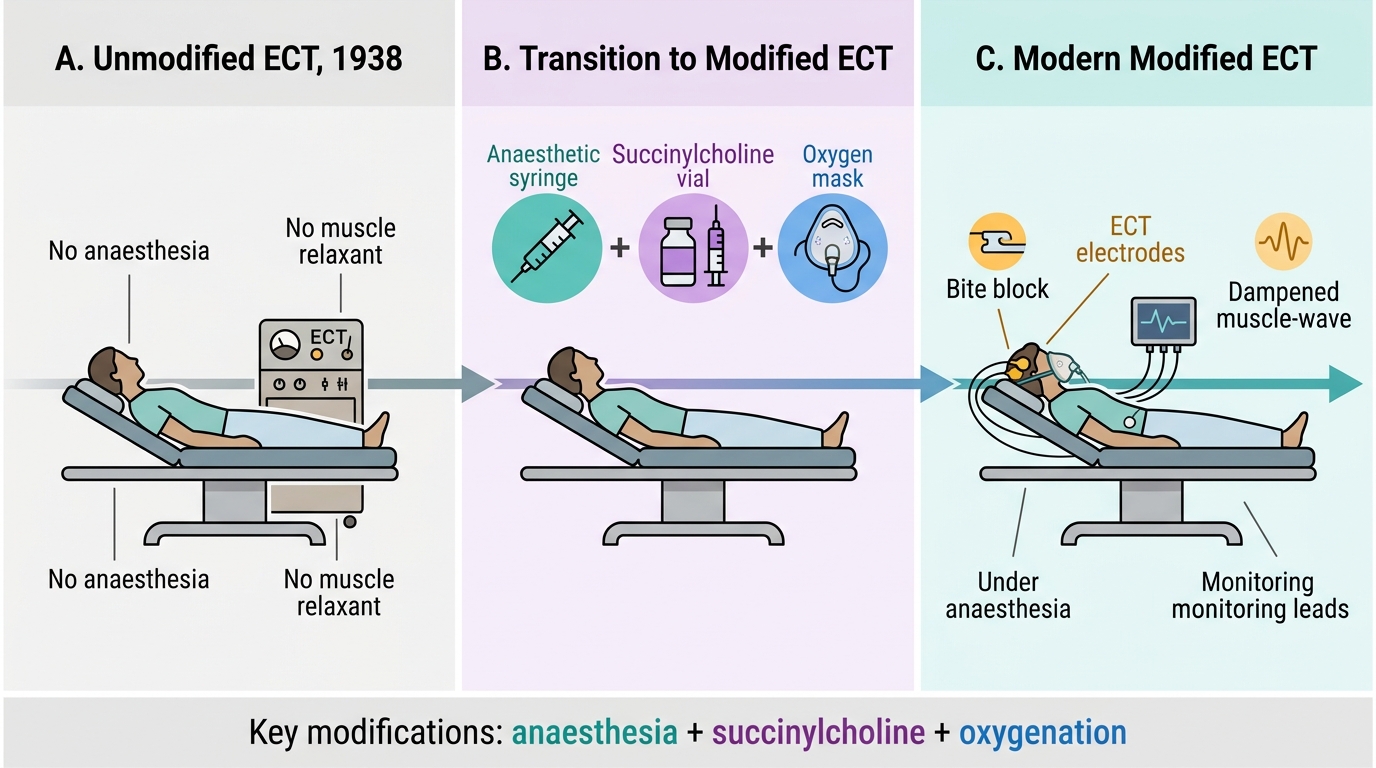
Electroconvulsive therapy is a treatment in which a brief, controlled electrical stimulus is applied to the scalp to induce a therapeutic generalised cerebral seizure in an anaesthetised patient. It was first introduced in clinical psychiatry by Cerletti and Bini in 1938, predating the era of modern psychopharmacology, and remains one of the most extensively studied biological treatments in all of medicine. Understanding its historical and clinical context is essential before examining the procedure itself.
In its earliest form, ECT was administered without anaesthesia, without muscle relaxants, and without oxygenation support — what we now call unmodified ECT. The generalised tonic-clonic seizure produced violent muscular contractions that caused serious complications: vertebral compression fractures, long-bone fractures, shoulder dislocations, and significant psychological distress for the awake patient. Public fear of ECT, which persists to this day, is largely rooted in images or accounts of this unmodified era or in dramatic (and inaccurate) cinematic depictions.
The term modified ECT refers specifically to the contemporary practice in which ECT is performed under short-acting general anaesthesia combined with a muscle relaxant (succinylcholine/suxamethonium) and oxygenation/ventilation support. This single modification transforms the procedure from a frightening, complication-prone intervention into a safe, controlled medical procedure. The generalised seizure still occurs — it is still detectable on EEG and drives the therapeutic effect — but the outward muscular manifestation is largely abolished, and the patient experiences nothing during the treatment.
The clinical relevance of ECT cannot be overstated. It consistently shows response rates of 70–90% in treatment-resistant severe depression — superior to pharmacotherapy alone in many studies — and it acts faster than any antidepressant, often producing meaningful improvement within 2–3 sessions. For a patient refusing food or at imminent suicidal risk, this speed of action is clinically decisive.
Evolution of ECT: From Unmodified to Modified Technique
Indications: When Is ECT Indicated?
The clinical indications for ECT are well-established and have been validated across decades of evidence. Understanding these indications requires grasping the underlying clinical logic: ECT is chosen either when the speed of response is critical (the patient cannot safely wait weeks for a drug to work), or when pharmacotherapy has failed or is contraindicated, or when pharmacotherapy itself poses an unacceptable risk in the specific patient (e.g. certain stages of pregnancy or severe cardiovascular disease). This framework — urgency, pharmacological failure, pharmacological contraindication — prevents both under-use of ECT (by recognising it as a first-line option in genuine emergencies) and over-use (by anchoring indications to specific, evidence-based criteria rather than vague clinical dissatisfaction). It is equally important to recognise that ECT is not exclusively a treatment for depression; its effectiveness spans several major diagnostic categories, each for distinct mechanistic or clinical reasons. A thorough knowledge of these indications is part of the core competency required at the level of a Year-3 MBBS student who may be participating in psychiatric ward rounds and consent discussions.
Provided image
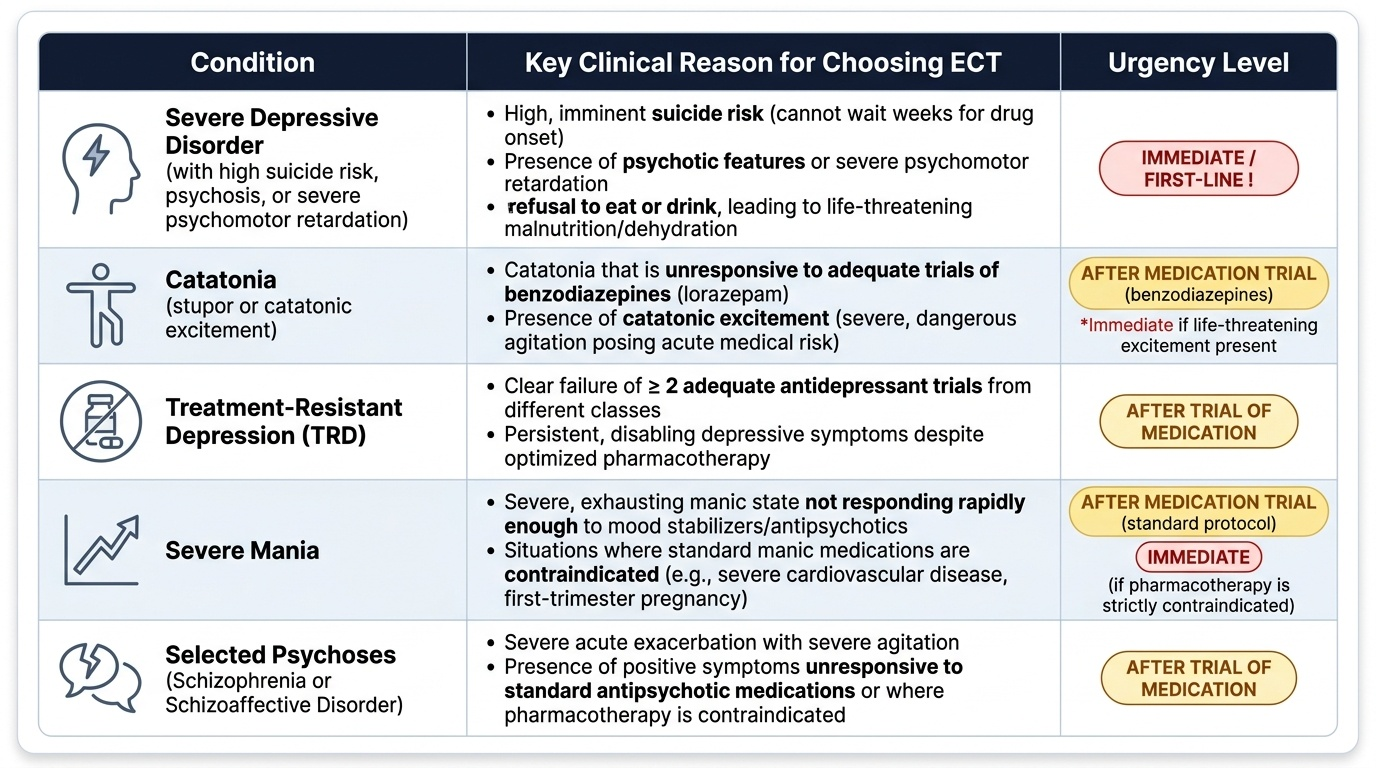
The major indications for ECT (per Ahuja, Kaplan & Sadock) are:
- Severe depressive disorder with high suicide risk: this is the most common indication. When a patient's suicidal risk is so high that waiting several weeks for antidepressants to work is dangerous, ECT can produce remission in days. Severe depression with psychotic features, severe psychomotor retardation, or refusal to eat or drink (creating a medical emergency from malnutrition and dehydration) also falls under this category.
- Catatonia: whether occurring in the context of a mood disorder, schizophrenia, or a medical condition, catatonia that is unresponsive to adequate trials of benzodiazepines (lorazepam) responds well to ECT. Catatonic excitement (the dangerous, agitated subtype) is also an indication.
- Treatment-resistant depression (TRD): defined as failure of ≥2 adequate antidepressant trials, TRD is a strong indication for ECT.
- Severe mania: when mania is severe and not responding rapidly enough to pharmacotherapy, or when medications are contraindicated (e.g. pregnancy), ECT may be used.
- Selected psychoses: in schizophrenia or schizoaffective disorder where antipsychotics have failed or are contraindicated, or where a rapid response is urgently needed, ECT may be considered — though it is less commonly used for psychosis than for mood disorders.
- Specific clinical circumstances where medication is hazardous: pregnancy (where ECT may be safer than certain psychotropic medications), elderly patients with severe cardiovascular disease limiting pharmacotherapy, and neuroleptic malignant syndrome (NMS) unresponsive to standard management.
SELF-CHECK
A 28-year-old woman at 20 weeks' gestation is hospitalised with severe postpartum psychosis and refuses all oral medications. She is mute, not eating, and at high suicidal risk. Which of the following is the most appropriate next step?
A. Initiate olanzapine oral disintegrating tablets and monitor for 4 weeks
B. Proceed with modified ECT after informed consent and obstetric clearance
C. Administer unmodified ECT immediately given the clinical urgency
D. Defer treatment and involve family-based crisis support
Reveal Answer
Answer: B. Proceed with modified ECT after informed consent and obstetric clearance
Modified ECT is indicated here on two grounds: (1) severe depression/psychosis with high suicidal risk and refusal of nutrition — an emergency requiring a fast-acting treatment; and (2) pregnancy, where ECT may be safer than prolonged high-dose psychotropics. Unmodified ECT (option C) is prohibited under the Mental Healthcare Act 2017 as it lacks anaesthetic protection. Options A and D do not address the immediacy of the clinical emergency.
The Modified ECT Procedure: Step by Step
The modified ECT procedure is a structured medical intervention with clearly defined stages. Each stage serves a specific safety or therapeutic purpose. Understanding the rationale behind each step is what separates a clinician who can explain and supervise ECT from one who merely knows its name.
Provided image
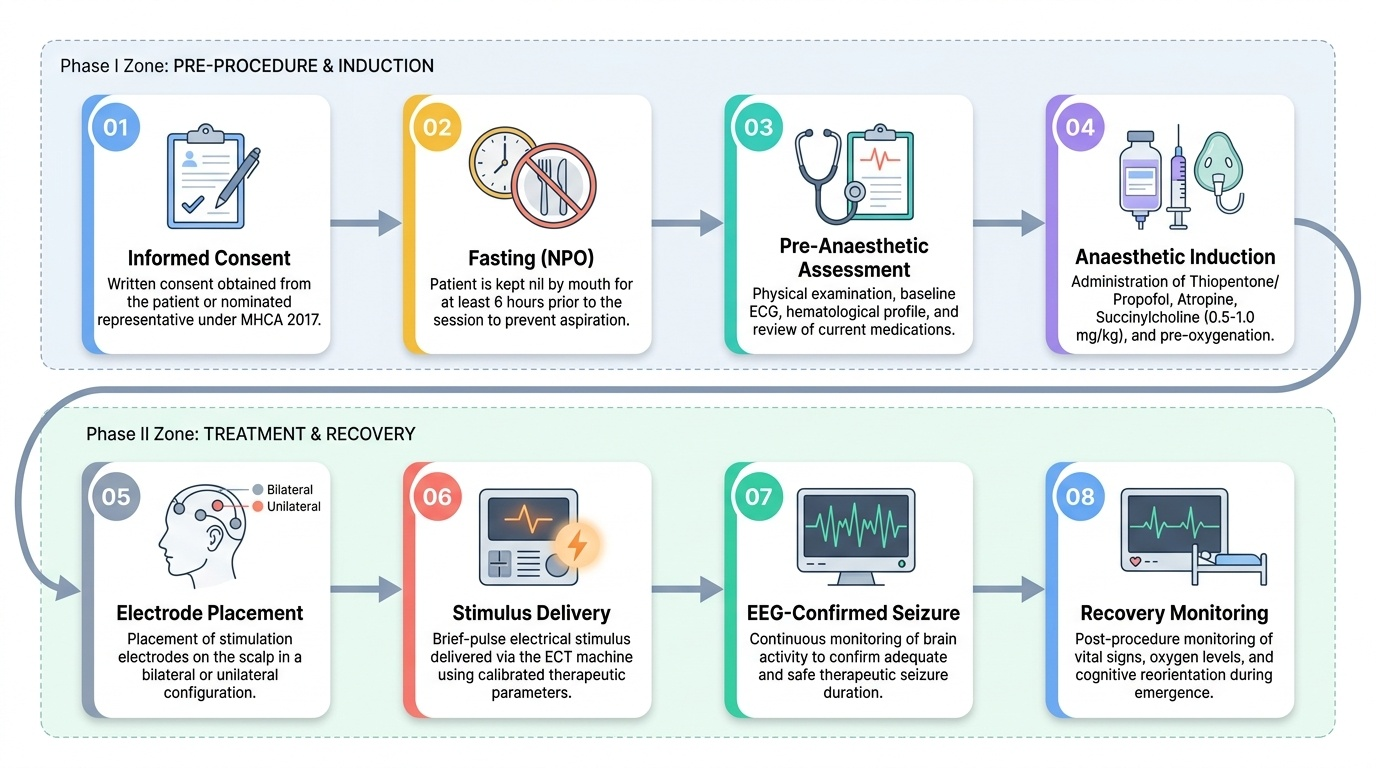
Pre-procedure preparation begins with comprehensive psychiatric assessment to confirm the indication and rule out alternatives. A pre-anaesthetic assessment is mandatory: baseline physical examination, ECG, haematological and biochemical profile, and documentation of current medications (especially those that may lower seizure threshold, such as theophylline, or that may interact with anaesthetic agents). Informed consent must be obtained in writing before the first treatment — from the patient if they have capacity, and from the nominated representative or guardian under the Mental Healthcare Act 2017 if they do not. The patient is kept nil by mouth (fasting) for at least 6 hours prior to each session because of the general anaesthetic.
Anaesthetic induction: a short-acting intravenous induction agent (commonly thiopentone or propofol in Indian practice) is administered to render the patient unconscious. An anticholinergic agent (atropine) may be given to reduce secretions and protect against bradycardia. The muscle relaxant succinylcholine (suxamethonium) — a depolarising neuromuscular blocking agent — is then administered intravenously in doses of approximately 0.5–1.0 mg/kg. It causes brief fasciculations followed by complete muscular paralysis within 30–60 seconds. Crucially, oxygenation and ventilation are maintained with a bag-mask or airway device throughout; the patient is also monitored with ECG, pulse oximetry, and blood pressure recording.
Electrode placement: electrodes are placed on the scalp according to one of two standard patterns. In bilateral (bitemporal) placement, one electrode is placed on each temple — this method is more efficacious and produces a faster response, but is associated with greater short-term cognitive side effects. In unilateral (right-sided or non-dominant hemisphere) placement, both electrodes are placed on the right (non-dominant) side — this approach produces fewer cognitive effects at the cost of somewhat reduced efficacy per session. The choice between bilateral and unilateral placement is made by the treating clinician, balancing clinical urgency against acceptable cognitive risk.
Stimulus delivery and seizure: a brief-pulse electrical stimulus of prescribed parameters (energy, pulse width, frequency) is delivered. A generalised seizure of adequate duration — conventionally ≥25 seconds on EEG, or ≥15–20 seconds of motor manifestation in the unmodified limb (a blood-pressure cuff is sometimes inflated on one forearm before succinylcholine to allow visual monitoring of the convulsion) — is the therapeutic target. If the seizure is too brief, the stimulus may be repeated. Because succinylcholine abolishes the motor component, seizure adequacy is confirmed by EEG monitoring in well-equipped centres.
Course of treatment: ECT is not a single treatment but a course of sessions, typically administered 2–3 times per week. A standard acute course is 6–12 sessions (average 8), though the number is determined by clinical response. Sessions continue until the patient achieves remission, then stop; some patients with recurrent or treatment-resistant illness receive maintenance ECT (monthly or less frequently) to prevent relapse.
Recovery monitoring: after the stimulus, the patient recovers from anaesthesia in a supervised recovery area. Vital signs are monitored until the patient is alert and stable. Post-ictal confusion (lasting minutes to tens of minutes) is normal and transient. The patient is not permitted to eat until fully recovered.