Page 2 of 8
PS13.1 | Modified ECT Principles — SDL Guide (Part 2)
Adverse Effects and Relative Contraindications
Modified ECT has a well-characterised adverse-effect profile. Understanding these effects accurately — particularly the cognitive ones — is essential for informed consent discussions and for dispelling the exaggerated fears patients and families often bring to the consultation.
Provided image
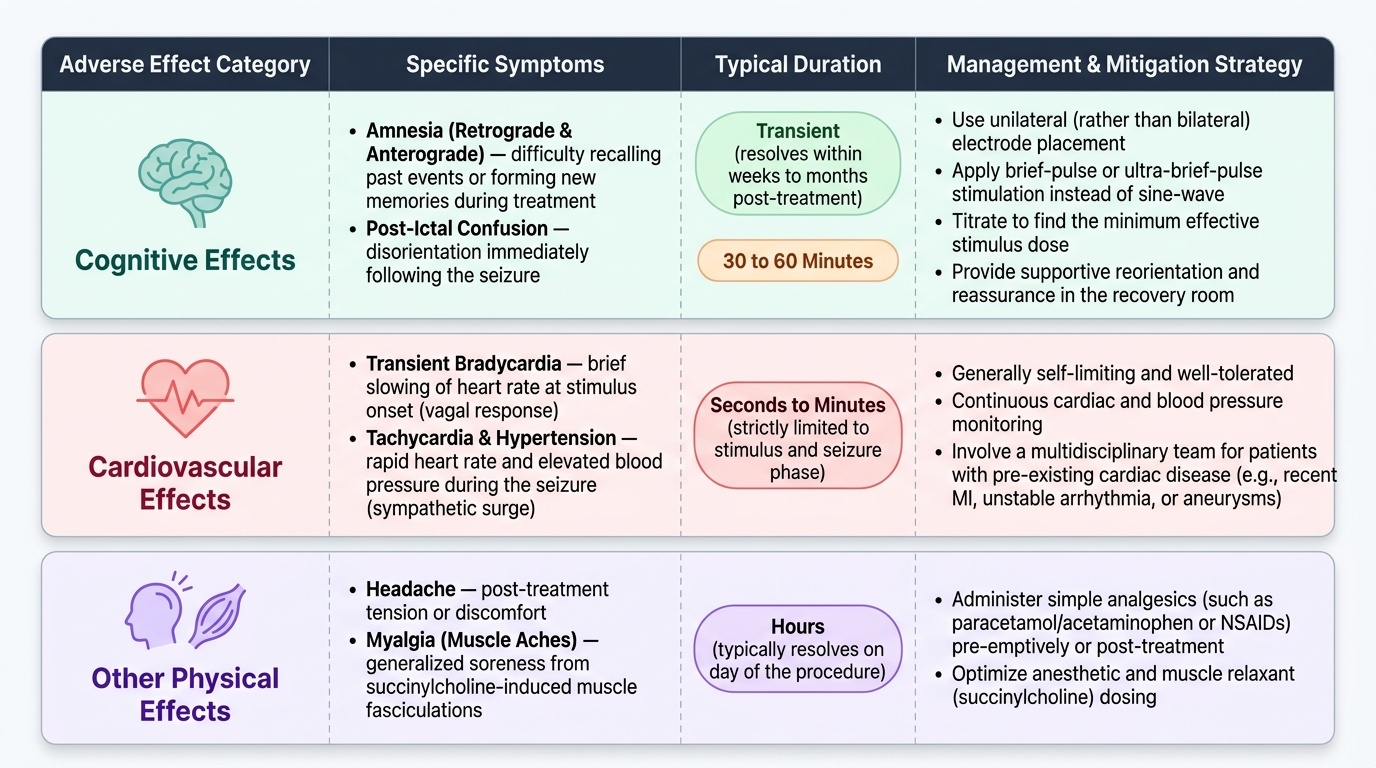
The most clinically important adverse effects are cognitive in nature. Retrograde amnesia (difficulty recalling events that occurred before the ECT course) and anterograde amnesia (difficulty forming new memories during the treatment course) are the most common complaints. Importantly, the majority of these memory effects are transient — they resolve within weeks to months after the ECT course ends. A minority of patients, however, report persistent memory gaps, particularly for events close to the treatment period. Bilateral electrode placement produces more cognitive effects than unilateral; using brief-pulse (rather than sine-wave) stimulation and titrating the minimum effective stimulus dose also reduces cognitive burden. Post-ictal confusion for 30–60 minutes after each session is expected and not a reason for alarm.
Cardiovascular effects include transient bradycardia (vagal, at stimulus onset) followed by tachycardia and hypertension (sympathetic surge) during the seizure. These are generally well-tolerated but require monitoring in patients with known cardiac disease. Muscle aches (from succinylcholine fasciculations) and headache following the session are common and manageable with simple analgesia.
There are no absolute contraindications to ECT in a strict sense — the risk-benefit analysis depends on the patient's clinical situation. However, relative contraindications or situations requiring special precautions include: raised intracranial pressure (brain tumour, recent cerebral haemorrhage — seizure can acutely raise ICP); recent myocardial infarction or unstable cardiac arrhythmia; phaeochromocytoma (hypertensive crisis from catecholamine surge); and aortic aneurysm. These are not reasons to refuse ECT if the clinical indication is compelling — they are reasons to involve a multidisciplinary team and take additional precautions.
Anaesthetic risks (including those of succinylcholine — hyperkalaemia in patients with burns, neuromuscular disease, or prolonged immobility; rare pseudocholinesterase deficiency causing prolonged paralysis; malignant hyperthermia) are managed by the anaesthetist and are not unique to ECT.
Dispelling Misconceptions About ECT
Few medical procedures carry as many entrenched misconceptions as ECT. These misconceptions are not merely academic curiosities — they prevent patients from accessing a life-saving treatment and place an ethical burden on clinicians to actively correct misinformation. Understanding and addressing each major myth is a core clinical skill.
Provided image
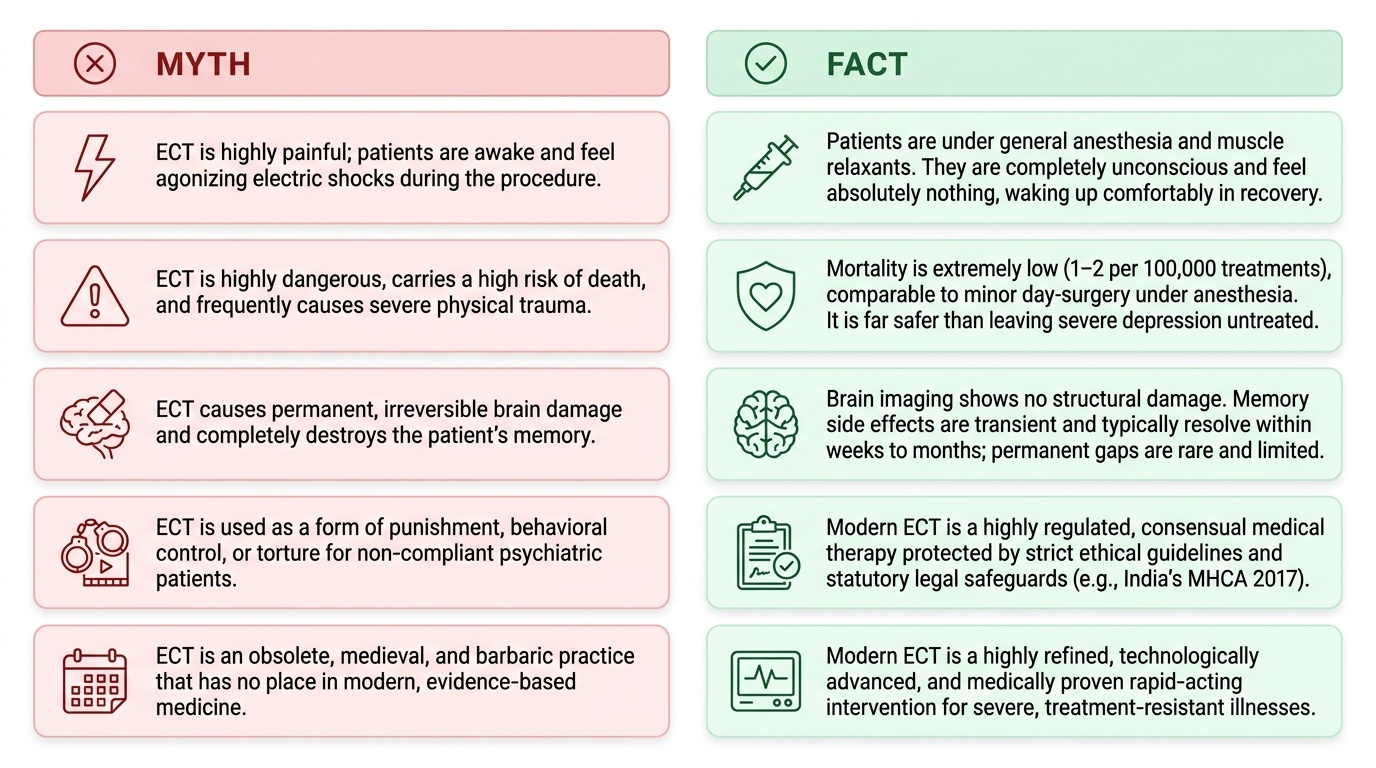
Misconception 1: ECT is painful — the patient feels electric shocks. This is false. The patient is under general anaesthesia during the entire procedure. They are completely unconscious from induction until recovery and feel nothing during the treatment. The experience is similar to undergoing any brief surgical procedure under general anaesthesia: the last thing they remember is the induction agent being administered, and the next thing they are aware of is waking up in the recovery area. This is categorically different from the unanaesthetised treatments depicted in older films and literature.
Misconception 2: ECT is dangerous and frequently causes serious harm. Mortality from ECT is extremely low — approximately 1–2 per 100,000 treatments, comparable to the risk of general anaesthesia for any minor procedure. This is far lower than the mortality risk of untreated severe depression (through suicide or medical deterioration). The modification of the technique — anaesthesia, succinylcholine, oxygenation — specifically exists to prevent the physical harms of unmodified ECT.
Misconception 3: ECT causes permanent brain damage or permanent memory loss. Brain imaging studies (MRI, fMRI) have not demonstrated structural brain damage from ECT. While transient memory difficulties are real and well-documented, the majority of patients recover their memory function within weeks to months. Persistent memory gaps are reported by some patients, particularly for events in the peri-treatment period, and should be acknowledged honestly — but the blanket claim of permanent memory destruction is not supported by evidence.
Misconception 4: ECT is used as punishment or behavioural control. This misconception is rooted in historical abuses and in cinematic depictions (notably the film 'One Flew Over the Cuckoo's Nest'). Modern ECT is a consensual medical treatment governed by strict legal and ethical safeguards. In India, the Mental Healthcare Act 2017 (MHCA 2017) provides explicit statutory protections:
- Informed consent is mandatory before ECT can be administered.
- ECT without anaesthesia (unmodified ECT) is prohibited for all adults under Section 94(2) of the MHCA 2017.
- ECT in minors (persons under 18 years) requires the additional approval of a High Court under Section 95 of the MHCA 2017 — it is not categorically banned but has a heightened consent and oversight threshold.
- Patients may issue an advance directive specifying their wishes regarding ECT, and this directive must be honoured.
Misconception 5: ECT is a last resort for hopeless cases. This framing understates ECT's role and may delay its use in situations where it should be first-line. In certain clinical scenarios — imminent suicidal risk, catatonia, ECT-responsive severe depression, high-risk pregnancy with psychiatric emergency — ECT may be the most appropriate treatment at the outset, not after months of failed pharmacotherapy.
SELF-CHECK
Under the Mental Healthcare Act 2017, which of the following statements about ECT in India is CORRECT?
A. Unmodified ECT is permitted with consent from the patient's family if the patient lacks capacity
B. ECT may be given without consent in a documented psychiatric emergency
C. Unmodified ECT is prohibited for all adults; ECT in minors requires High Court approval
D. Advance directives regarding ECT are advisory and may be overridden by the treating psychiatrist
Reveal Answer
Answer: C. Unmodified ECT is prohibited for all adults; ECT in minors requires High Court approval
The MHCA 2017 Section 94(2) categorically prohibits unmodified ECT for adults regardless of consent or clinical emergency. ECT in minors is not banned but requires a High Court's additional approval (Section 95). Informed consent is mandatory (invalidating option B). Advance directives are legally binding under the MHCA 2017, not merely advisory (invalidating option D).
Self-Assessment: Consolidating Your Understanding of Modified ECT
The following questions are designed to help you consolidate and test your understanding of the material covered in this module. Work through each item independently before reviewing the answers. The goal is not merely to recall facts but to be able to explain the reasoning — because in clinical practice, you will need to explain ECT to a patient or family member, not recite facts to an examiner.
Consider each of the following scenarios and questions:
Scenario A — Mechanism of modification: A colleague asks: 'If succinylcholine prevents convulsions, how does ECT still work?' Construct a clear, accurate response of 3–4 sentences that explains the distinction between the motor manifestation of a seizure and the underlying cerebral electrical event, and why the therapeutic effect depends on the latter.
Scenario B — Indication reasoning: A 62-year-old man with severe treatment-resistant depression is referred for ECT. His wife refuses, stating he has had two antidepressant trials and 'ECT will make him forget everything permanently.' Identify the clinical indication for ECT in this case. Identify the specific factual error in the wife's statement and explain what accurate information you would provide about memory effects.
Scenario C — Procedural steps: List, in correct sequence, the seven key procedural stages of a modified ECT session from preparation through recovery. For each, state one specific safety action taken at that stage.
Scenario D — Legal framework: A registrar proposes giving a 16-year-old patient with severe catatonic schizophrenia ECT, noting it 'should be fine because the parents have consented.' Identify the legal error in this reasoning and state the correct procedure under the MHCA 2017.
Scenario E — Contraindication analysis: A patient with a known intracranial meningioma (currently asymptomatic, no evidence of raised ICP) requires ECT for severe suicidal depression. Is the meningioma an absolute contraindication? Explain the risk-benefit reasoning a clinician should apply.
Reflecting on Scenario A is particularly instructive: succinylcholine paralyses only the peripheral neuromuscular junction — it crosses neither the blood-brain barrier nor blocks central neuronal firing. The cerebral seizure (the actual therapeutic mechanism) proceeds unimpaired and is detectable on EEG. The motor convulsion (the part that broke bones in the unmodified era) is abolished. This one fact answers the most common mechanistic misconception and explains why the 'modification' is purely about safety, not efficacy.
CLINICAL PEARL
The 'one cuff' technique is a practical bedside sign used when EEG monitoring is unavailable. Before administering succinylcholine, a blood-pressure cuff is inflated above systolic pressure on one forearm — typically the non-dominant arm. Because succinylcholine cannot reach the muscles distal to the cuff, the motor convulsion remains visible in that hand even though the rest of the body is paralysed. The duration of visible motor activity in that hand is used as a surrogate measure of seizure adequacy. This technique illustrates a key principle: the succinylcholine acts peripherally (at the neuromuscular junction) and has no central effect — the cerebral seizure is entirely unmodified by the drug.